2990
Views & Citations1990
Likes & Shares
Background: Individuals living with HIV/AIDS have a higher risk of cardiovascular complications, including hypertension. We, therefore, assess the prevalence of hypertension and its association with Tuberculosis in HIV patients on ART in Bagamoyo district eastern Tanzania.
Methods: This was a cross-sectional study involving HIV-infected individuals on ART, consecutively enrolled from two selected care and treatment clinics (CTC), between March and May 2019. Hypertension was defined as systolic blood pressure (SBP) ≥ 140 mm Hg, diastolic blood pressure (DBP) ≤ 90 mm Hg or being on-ant hypertensive medication regardless of blood pressure measurement on the day of the visit.
Results: We investigated 328 HIV patients on ART, 64.6% were female, 92.68% on non-protease inhibitors, 0.61% had current TB and 14% had a history of Tuberculosis in the past 5 years. The overall prevalence of hypertension in HIV patients on ART was 29.3% and it was significant and positively associated with increasing age, obesity, family history of hypertension, and, current history of TB. However, having a history of Tuberculosis in the past 5 years was not associated with increased odds of having hypertension.
Conclusion: The prevalence of hypertension in HIV patients on ART was higher and it was associated with traditional risk factors and the current history of tuberculosis and but not with a history of Tuberculosis in the past 5 years. Regular monitoring of blood pressure is crucial among HIV/AIDS patients attending HIV outpatient clinics.
Keywords: HIV, Hypertension, ART, CTC, Tuberculosis
Abbreviations: ART: Anti-Retroviral Therapy; BMI: Body Mass Index; CTC: Care and Treatment Clinic; HIV: Human Immunodeficiency Virus; TB: Tuberculosis
INTRODUCTION
Effective use of antiretroviral therapy (ART), has greatly improved the quality of life and survival of people living with HIV/AIDS [1]. However, the incidence rate and mortality from cardiovascular risk factors including hypertension are reported to be growing up [2-4]. For example, in a recent meta-analysis study prevalence of hypertension was 34.7% among those on ART compared to 12.7% in ART naïve individuals [5]. In Tanzania, hypertension prevalence of (28.3%) in HIV patients on ART has been reported at 28.3% which is higher compared to 5.3% in HIV ART-naïve and 16.3% in HIV negative individuals [6].
Hypertension (the leading risk factor of deaths) is a growing health problem in individuals living with HIV/AIDS [7,8]. However, the contributions of HIV related factors include Tuberculosis to hypertension have not been extensively investigated in Tanzania. In addition to the traditional risk factors, hypertension in HIV patients can be attributed to, inflammation, ART toxicity and immune response [9].
Traditional risks include risks such as increasing age, sex and increasing Body mass index [10]. However, it’s unclear whether traditional risk factors may interact with HIV related factors such as Tuberculosis (TB) to increase the risk of hypertension.
Evidence exists that TB may contribute to overall cardiovascular risk including hypertension perhaps through inflammation and autoimmune processes [11,12]. Although TB is the most prevalent and severe co-infection in HIV patients [13,14], little is known about its association with hypertension in HIV patients, especially in developing countries.
Therefore, we undertook a cross-sectional study to investigate the prevalence of hypertension and its association with TB in HIV patients on ART adjusting for potential confounders. To the best level of our knowledge, this cross-sectional study is the first of its kind to investigate the association between TB and hypertension among HIV patients on ART while adjusting for confounders.
METHODS
Study design and location
We conducted a cross-sectional study involving HIV patients who were on ART between March and April 2019, in Bagamoyo district, eastern Tanzania. The district is located in the coastal region with an HIV prevalence rate of 6.4% [15]. Data were collected from 2 public clinics which were purposely selected based on their relatively large size and presence of patient’s record database (computer-based record system). These clinics provide services to individuals living with HIV/AIDS based on national HIV/AIDS guidelines [16].
The inclusion criteria were being HIV positive, aged above 18, on ART, who gave consent for participation. Women who reported to be pregnant and those on contraceptive pills were excluded. The patients were then consecutive enrolled until the target sample size of 328 was achieved.
Blood pressure measurement
Blood pressure was measured in the right arm, using a mercury sphygmomanometer of appropriate size, with individual participants sitting in a relaxed position and upright position [17], two readings were taken 10 min apart and an average of two readings was used. Hypertension was defined as systolic blood pressure (SBP) of ≥ 140 mm Hg, diastolic blood pressure (DBP) of ≥ 90 mm Hg [17] or taking ant-hypertensive medications regardless of blood pressure findings.
Anthropometric measurement
Body weight (accuracy of 0.1 kg) was measured using Seca patients weighing machines with individual participants at minimal clothes and wearing no shoes. Body height was measured using a stadiometer (accuracy of 0.1 cm) participant wearing no shoes. Body mass index (BMI) was calculated using the formula: weight in kilogram (kg) divided by the square of height in meters (kg/m2). BMI was categorized and defined using the WHO protocol as follows, underweight 2, normal body weight 18.5-24.9 kg/m2, overweight 25-29.9 kg/m2 and obese ≥ 30 kg/m2 [18].
Collection of socio-demographic and HIV related information
The study used a structured questionnaire administered by trained health care workers (nurses and doctors) was used to gather information with respect to participants’ socio-demographic, family history of hypertension, current history of tuberculosis and history of tuberculosis in the past 5 years.
The following information was extracted directly from patient record card or computerized patient database system: Duration since HIV diagnosed, Recent CD4+ cell count, the current class of ART medication, individual combination therapy and duration on ART medication.
Definition of terms
Recent CD4+ cell count was defined as the amount of CD4+ T cell count which was measured in the past 6 months. Current TB was defined as currently being on anti-TB medication after sputum analysis or chest radiography. History of TB in the past 5 years was defined as being on anti-TB medication for at least 6 months within the last 5 years.
Study variables
The outcome variable of interest was hypertension defined as blood pressure ≥ 140/90 mm Hg or being on ant-hypertensive medication. Exposure variables of interest during the analysis were current TB/HIV co-infection and the history of TB in the past 5 years.
Data management and analysis
Data was collected using a study questionnaire, then coded using a codebook followed by the manual entrance in an excel sheet. Before data entry in the excel sheet completed questionnaire was reviewed for completeness and clarity. Before data analysis, another review was done for errors, missing data, and inconsistencies. The analysis was done using Stata software version 13.
We included 328 participants in the final analysis and 33 participants had missing data regarding the recent CD4+cell count. Recent CD4+ cell count was defined as the one which was taken within the last 6 months. In 33 participants with missed data on CD4+ cell count, they had CD4+ cell count either not taken at all or taken in a period of more than 6. A descriptive analysis (percentage) was used to summarize the data. Logistic regression, both univariate and multivariate analysis was performed to establish the risk factors of hypertension. In the multivariate analysis, we included factors with p-value ≤ 0.005, age, sex and the current class of ART.
ETHICAL APPROVAL
The study was approved by institutional review of the Ifakara Health Institute, Bagamoyo district executive director office as well as the authority of the respective health facility. Written informed consent was obtained from all study participants prior to study procedures.
RESULTS
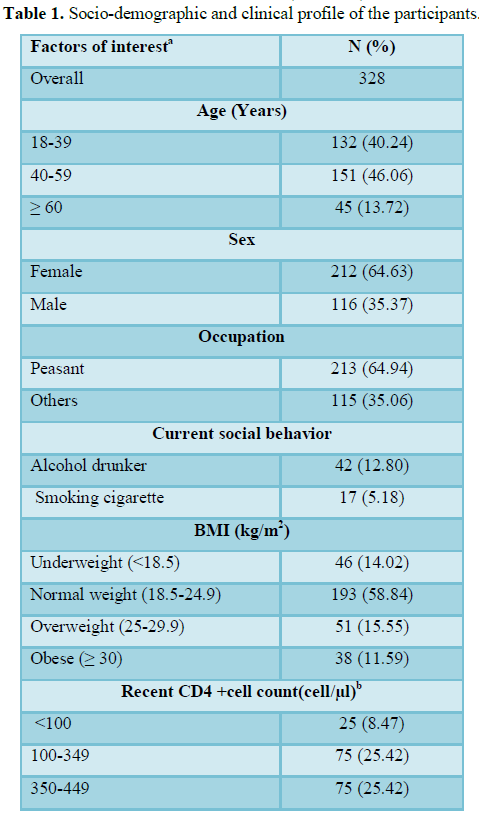
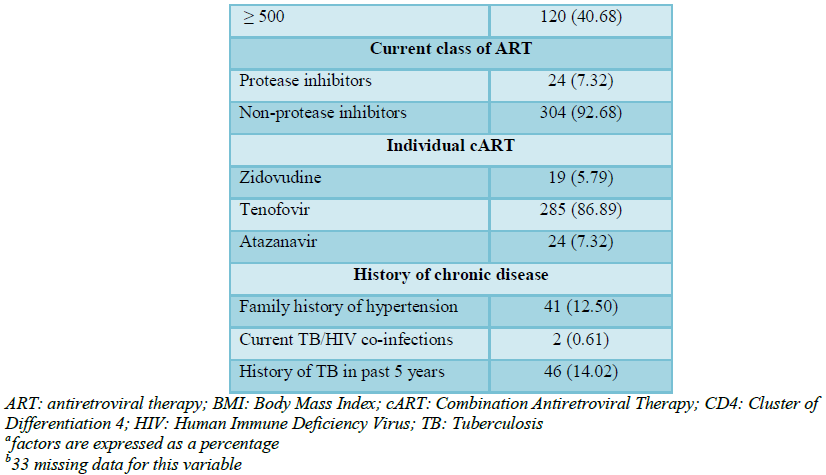
Table 1 summarizes the socio-demographic and TB characteristics of the participants. We included 328 HIV infected individuals who were on ART for the analysis. Out of all participants, 212 (64.6%) were female and 116 (35.4%) male. In the description of the age categories, 132 (40.24%), 151 (46.06%) and 45 (13.72%) were individuals aged 18-39, 40-59 and ≥ 60, respectively. Out of 328, 89 (25%) of the participants were either obese or overweight. Current alcohol drunker and smoking cigarettes were observed in 42 (12.8%) and 17 (5.18%), respectively.
Out of 328, 2 (0.61%) patients had HIV/TB co-infected and 46 (14%) of patients had a history of TB in the past 5 years (Table 1). There were 304 (92.68%) patients on non-protease inhibitors and 24 (7.32%) on protease inhibitors, with the majority of patients 285(86.89%) were on Tenofovir-based combination therapy and the rest were either on Zidovudine based combination therapy or Atazanivir (Table 1). Data on CD4+ cell count in the last 6 months was available in 25 (8.47%), 75 (25.42%), 75 (25.42%) and 120 (40.68%) patients had CD4+ cell count, <100, 100-349, 350-499 and ≥ 500, respectively (Table 1).
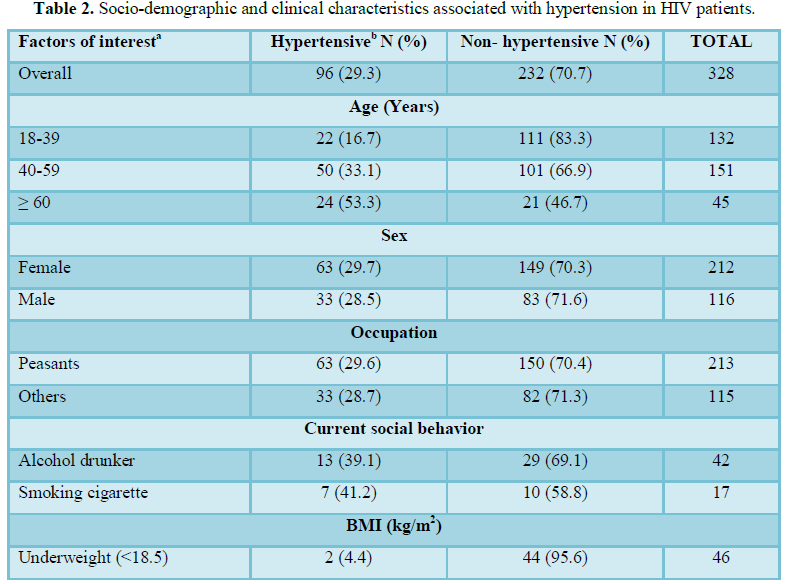
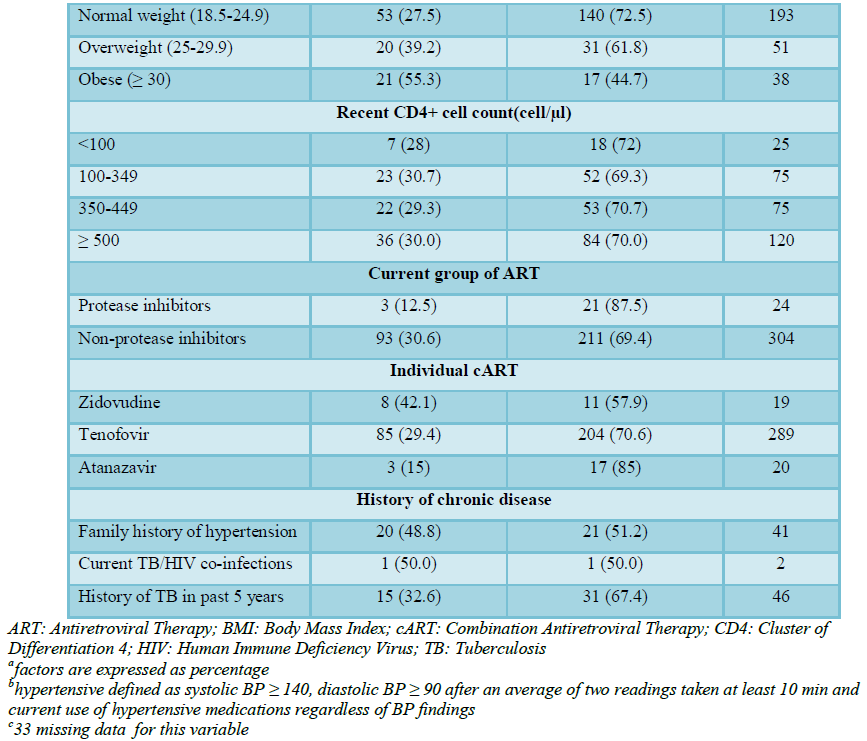
In our current study, the overall prevalence of hypertension in HIV patients on ART was 96 (29.3%). According to gender, the prevalence was 33 (28.5%) in males and 63 (29.7%) in females (Table 2). Regarding TB infection, the prevalence of hypertension was 1 (50%) in those with current TB/HIV and 15 (32.6%) in those with a history of TB in the past 5 years (Table 2).
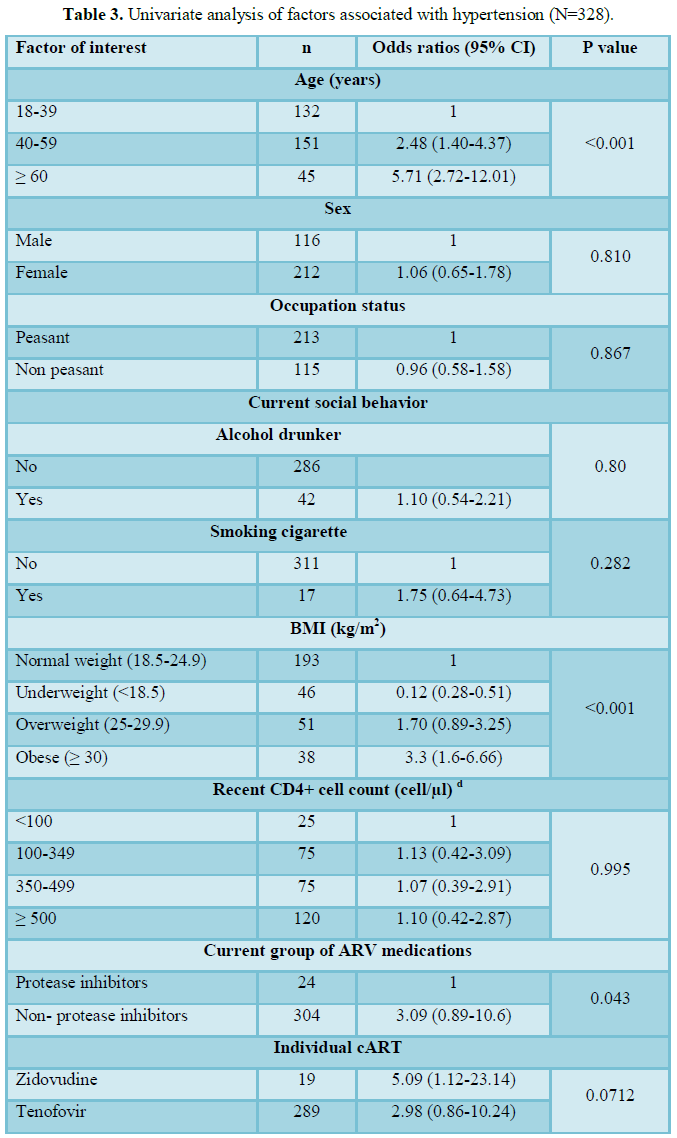
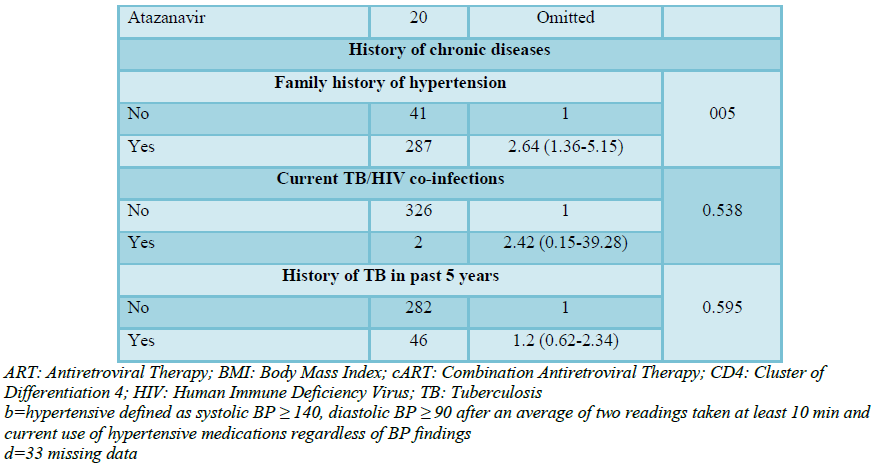
In univariate logistic regression analysis, the factors that were significantly associated with increased odds of having hypertension were: increasing age, higher BMI, family history of hypertension and non-protease inhibitors (Table 3). The odds for hypertension were highest among individuals ≥ 60 years of age, odds ratio 5.71 (2.72-12.01) (Table 3). Moreover, regarding body mass index obese hold the highest odds ratio of 3.3 (1.60-6.66) (Table 3). A family history of hypertension and non-protease inhibitors had an odds ratio of 2.64 (1.36-5.15) (Table 3).
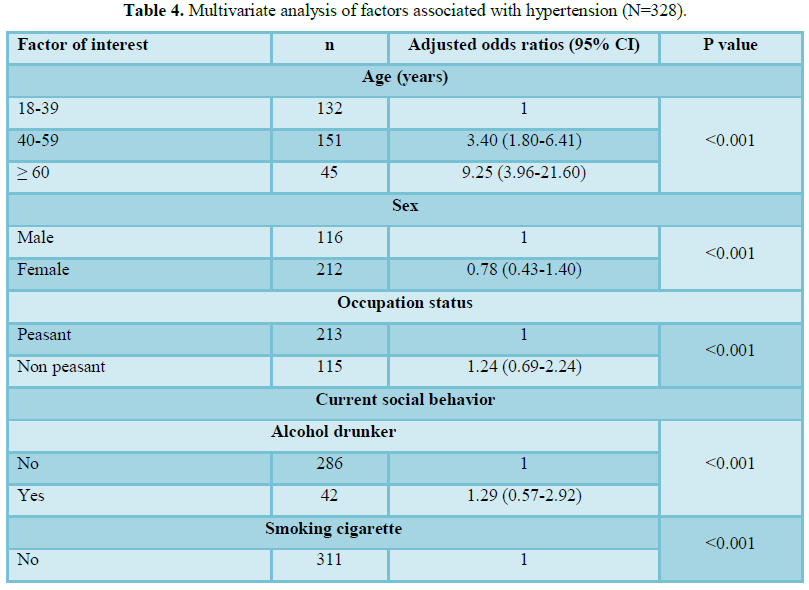
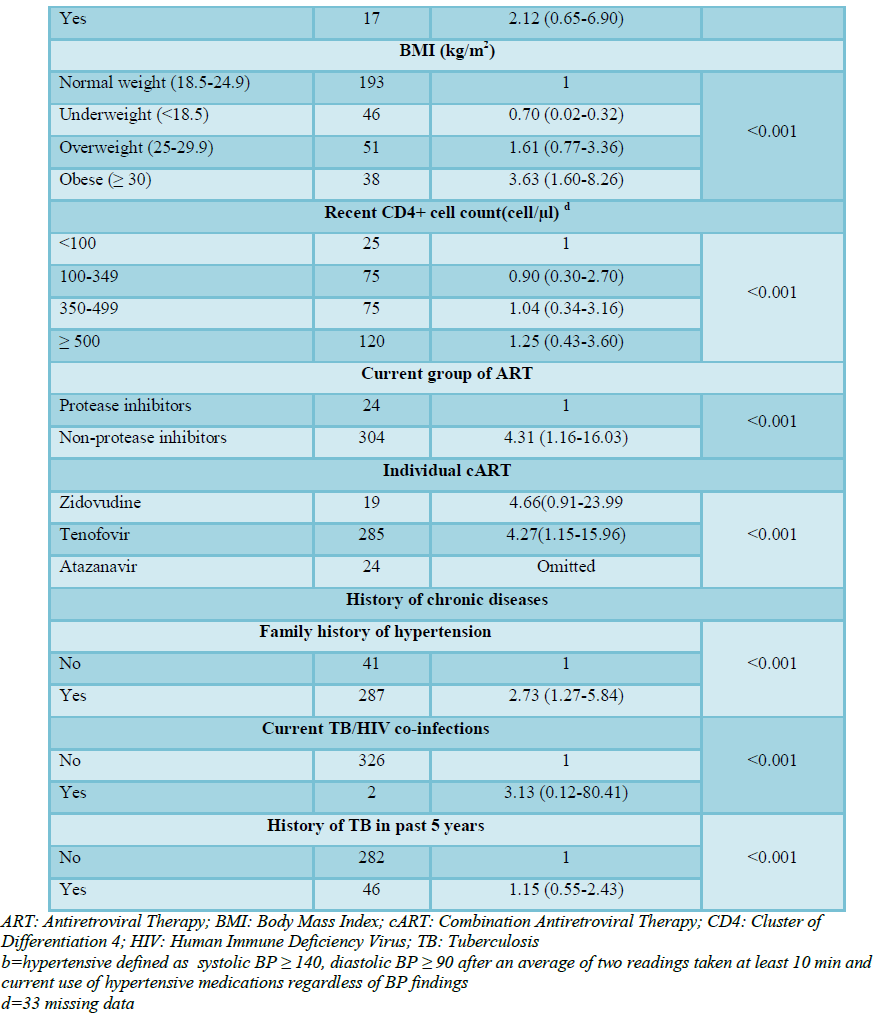
In the multivariate analysis, HIV related factors that were independently associated with increased odds of having hypertension were, non-protease inhibitors 4.31 (1.16-16.03) <0.001, current TB/HIV co-infection 3.13 (0.12-80.41) <0.001, Zidovudine 4.66 (0.91-23.99) (Table 4).
DISCUSSION
In this cross-sectional study analyzing the prevalence of hypertension and its association with TB among HIV patients, we found the prevalence of hypertension to be 29.3%. We also observed that the odds of having hypertension were significantly associated with increasing age, obesity, and family history of hypertension and non-protease inhibitors. Current TB/HIV co-infection was found to increase the odds of having hypertension in multivariate analysis.
The high prevalence (29.3%) in our current study appears similar to that of the observed prevalence in previous studies in HIV patients [5,6]. This strengthens the evidence that the prevalence of hypertension is higher in HIV patients on ART.
We also observed factors that were significant and positively associated with increased odds of hypertension which included: increasing age, obesity and family history of hypertension. These findings are consistent with previous studies [19,20]. This supports the evidence that traditional risk factors are potential predictors of hypertension even in HIV patients.
The interaction between TB infection and hypertension in HIV patients has been reported in the literature [11]. The possible mechanism by which TB can cause hypertension is through the inflammatory process which can end up with atherosclerosis [11]. Furthermore, TB can contribute to hypertension, because it can lead to diabetes mellitus [21] and diabetes mellitus itself is the risk factor of hypertension [22]. Additionally, hypertension may occur secondarily from renal failure after TB causing extensive destruction of kidney parenchyma tissues [23]. In our current study, we found that current TB/HIV co-infection increases the odds of having hypertension 3.13 (0.12-80.41)
In our current study, we also found that having a history of TB in the past 5 years did not increase the odds of having hypertension, contrary to the previous study in Dar es Salaam, Tanzania which reported a protective effect of prior history of TB against hypertension [24]. An important difference to note is that in our current study we limited the history of the previous TB to within 5 years while the study by Njelekela et al. [24], had no time limit concerning the prior history of TB. We recommend further studies to investigate more about the association between TB and hypertension in HIV patients on ART.
CONCLUSION
The prevalence of hypertension in HIV patients on ART was higher and it was associated with traditional risk factors but not with the history of Tuberculosis in the past 5 years. We cannot justify the association between current TB infection and hypertension based on 2 patients with current TB infection which is a very small number to conclude.
Routine screening of blood pressure and health education, body weight control, healthy diet, physical activity should be emphasized as essential components of treatment and care of HIV patients. We recommend further longitudinal studies to explore more on the association between TB and hypertension in HIV patients.
We faced the followings limitations: being cross-sectional we cannot establish causality between selected exposure variable and outcome variable. Also, we did not include HIV-negative individuals to make a comparison between the two groups. Again we cannot justify the association between current TB infection and hypertension based on 2 patients with current TB infection which is a very small number.
Despite the mentioned limitations, this study provided important results regarding the association between TB and hypertension in HIV patients on ART, particularly in low-income countries.
1. Chastain DB, Henderson H, Stover KR (2015) Epidemiology and management of antiretroviral - Associated cardiovascular disease. Open AIDS J 9: 23-37.
2. Fahme SA, Bloomfield GS, Peck R (2018) Hypertension in HIV-infected adults. Hypertension 72: 44-55.
3. Korem M, Wallach T, Bursztyn M, Maayan S, Olshtain-Pops K (2018) High prevalence of hypertension in Ethiopian and non-Ethiopian HIV-infected adults. Int J Hypertens 2018: 1-7.
4. Fatou N, Gueye N, Ka D, Tall AB, Ndiaye K, et al. (2017) Prevalence of hypertension and associated factors in patients living with HIV followed at the ambulatory treatment center (CTA of Fann National University Hospital in Dakar). Sci Res 9: 727-737.
5. Xu Y, Chen X, Wang K (2017) Global prevalence of hypertension among people living with HIV: A systematic review and meta-analysis. J Am Soc Hypertens 11: 530-540.
6. Peck RN, Shedafa R, Kalluvya S, Downs JA, Todd J, et al. (2014) Hypertension, kidney disease, HIV and antiretroviral therapy among Tanzanian adults: A cross-sectional study. BMC Med 12: 1-11.
7. Nduka CU, Stranges S, Sarki AM, Kimani PK, Uthman OA (2016) Evidence of increased blood pressure and hypertension risk among people living with HIV on antiretroviral therapy: A systematic review with meta-analysis. J Hum Hypertens 30: 355-362.
8. Gakidou E, Afshin A, Abajobir AA, Abate KH, Abbafati C, et al. (2017) Global, regional and national comparative risk assessment of 84 behavioral, environmental and occupational and metabolic risks or clusters of risks, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 390: 1345-1422.
9. Madhur MS, Barbaro NR, Moreno H, Itani HA, Kirabo A, et al. (2016) Immune activation caused by vascular oxidation promotes fibrosis and hypertension. J Clin Invest 126: 1607-1607.
10. Romesser PB, Riaz N, Wolden SL, Gelblum DY, Eric J, et al. (2016) Percutaneous endoscopic gastrostomy in oropharyngeal cancer patients treated with intensity-modulated radiotherapy with concurrent chemotherapy. Cancer J Clin 118: 6072-6078.
11. Villa G, Phillips RO, Smith C, Stockdale AJ, Beloukas A, et al. (2018) Renal health after long-term exposure to tenofovir disoproxil fumarate (TDF) in HIV/HBV positive adults in Ghana. J Infect 76: 515-521.
12. Okello S, Kanyesigye M, Muyindike WR, Annex BH, Hunt PW, et al. (2016) Incidence and predictors of hypertension in adults with HIV-initiating antiretroviral therapy in southwestern Uganda. 33: 2039-2045.
13. Calisman E (2017) Effects of tuberculosis and HIV co-morbidities on the cardiovascular system and cardiovascular disease: A review of current literature. Medical University of Graz.
14. FawziW, Liu E, Makubi A, Drain P, Spiegelman D, et al. (2015) Tuberculosis incidence rate and risk factors among HIV-infected adults with access to antiretroviral therapy. HHS Public Access 29: 1391-1399.
15. (2017) Tanzania HIV Impact Survey.
16. MoHCDGEC (2017) National Guideline for the Mangement of HIV and AIDS. 6th Edn, p: 384.
17. U.S Department of Health and Human Services, National Institutes of Health, National Heart, Lung and Blood Institute Program, N. high blood pressure education (2004) National high blood pressure education program complete report. The 7th Report of the Joint National Prevention, Detection, Evaluation and Treatment of High Blood Pressure.
18. World Health Organization (2004) Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation. World Health Organ Tech Rep Ser. WHO, pp: 1-253.
19. Furrer H, Hatz C, Tanner M, Battegay M, Letang E, et al. (2017) Incidence and risk factors for hypertension among HIV patients in rural Tanzania - A prospective cohort study 630: 1-14.
20. Chireshe R, Naidoo K, Nyamakura R, Africa S (2017) Hypertension among human immunodeficiency virus-infected patients on treatment at Parirenyatwa Hospital: A descriptive study. Afr J Prim Health Care Fam Med 11: 1-8.
21. Ogbera AO, Kapur A, Abdur-Razzaq H, Harries AD, Ramaiya K, et al. (2015) Clinical profile of diabetes mellitus in tuberculosis. BMJ Open Diabetes Res Care 3: 1-6.
22. Petrie JR, Guzik TJ, Touyz RM (2018) Diabetes, hypertension and cardiovascular disease: Clinical insights and vascular mechanisms. Can J Cardiol 34: 575-584.
23. Shen TC, Huang KY, Chao CH, Wang YC, Muo CH, et al. (2015) The risk of chronic kidney disease in tuberculosis: A population-based cohort study. QJM 108: 397-403.
24. Njelekela M, Muhihi A, Aveika A, Spiegelman D, Hawkins C, et al. (2016) Prevalence of hypertension and its associated risk factors among 34,111 HAART Naïve HIV-Infected Adults in Dar es Salaam, Tanzania. Int J Hypertens 2016: 1-10.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6
-
Table 7
-
Table 8
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Clinical Trials and Research (ISSN:2637-7373)
- International Journal of Clinical Case Studies and Reports (ISSN:2641-5771)
- Journal of Renal Transplantation Science (ISSN:2640-0847)
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- International Journal of Anaesthesia and Research (ISSN:2641-399X)
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- Ophthalmology Clinics and Research (ISSN:2638-115X)


