1800
Views & Citations800
Likes & Shares
Applying Health Promotion Model in research:
Research applying the theory: Health Promotion Model (HPM) by Nola Pender (1996). The model focuses on explaining behaviors in health promotion. According to the model, perceived barriers and benefits in improve caring practices will lead to motivate behavior promoting health. A good assessment of health behaviors is the foundation for adjusting the health promotion and prevention plan in children. Assessment provides a basis for making clinical assessments, health problems, nursing diagnoses, desired health or behavioral outcomes, and measures intervention may be effective [9]. In this study, the theory has provided methods to evaluate mothers' health-promoting behaviors and guide nursing interventions to improve mothers' behaviors in caring for children
Sample: Mothers who fulfill the inclusion criteria
Sampling criteria
Inclusion criteria:
Mothers who:
- Have children under 5 years old
- Were present in the selected community
- Were willing to participate in the study
- Were living in a rural area from October 2020 to December 2021.
Exclusion criteria: Mothers are unable to write or communicate.
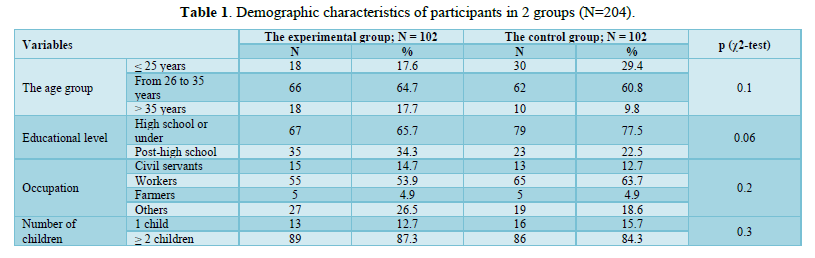
Sampling technique: The simple random technique used to select the samples based on inclusion and exclusion criteria. Mothers in each commune by own number in the list. Use Excel software to randomly select mothers. Mothers who do not agree to participate in the study or do not meet the selection criteria will be eliminated and replaced with another random number, ensuring that subjects participate meet the inclusion and exclusion criterias. In the end, the actual number of mothers participating was a total of 204 mothers include 102 mothers in the experimental group and 102 mothers in the control group. The questionnaire was based on the WHO guidelines [10]. The tool was validated by 5 pediatric experts with CVI = 0.98. And then, the questionnaire was tested for structural validity and reliability by testing on 130 mothers with children under 5 years old in rural areas in Viet Nam (these 130 mothers didn't participate in the later survey). The result of reliability with Cronbach's Alpha value was greater than 0.70 for the total scale of the knowledge, attitude and practices. Evaluating the structural validity of the questionnaire by analyzing the exploratory factor (EFA) with the KMO coefficient (Kaiser-Meyer-Olkin) was 0.57. Therefore, this questionnaire meets the standards used in this study. The questionnaire contains 34 items, including 8 items about the general information characteristics of mothers and 26 items to assess the knowledge, attitude, and practices; 3 checklists about practical skills of mothers in the prevention and caring for children with ARI. It is divided into 2 sections.
Section A: This section deals with the general information characteristics of mothers: The information about the age, educational level, occupation, residence and number of children of mothers. This section includes 8 items.
Section B: Including 3 parts:
Part 1: This section deals with the knowledge about the ARI disease including 2 main contents: Signs and symptoms; Prevention and caring for children with acute respiratory infections including 2 main contents: Nutrition and nasal hygiene for children. This section includes 8 multiple-choice questions. The different levels of knowledge are categorized as follows:
Satisfactory knowledge ≥ 70%
Unsatisfactory knowledge < 70%
Part 2: This section deals with the attitude of mothers about ARI including 3 main contents: Mother's attitude about the disease, care, and prevention of ARI. This section includes 10 items using a five-point Likert scale with answers in 5 levels corresponding to the score 1, 2, 3, 4, 5: Strongly disagree, disagree, neutral, agree, strongly agree. The items score was added to calculate the total scores, where a higher score indicates a better attitude. The total score of the attitude divides by 10 (items). Satisfactory level of attitude from 4-5 points (the answer: strongly agree, agree). In contradiction, an unsatisfactory level of attitude is less than 4 points (the answer: strongly disagree, neutral, disagree).
Part 3: This section deals with the practices of mothers in caring for children with ARI including 4 main contents: Practice taking children to go to the doctor, giving them water to drink, relieving cough, cleaning the nose; About prevention of ARI including 4 main contents: Avoid to cigarette smoke, dust and animal hair, breastfeed, vaccinated fully according to regulations. This section includes 8 multiple-choice questions and 3 checklists about practical skills. The different levels of practice are categorized as follows:
Satisfactory practices ≥ 70%
Unsatisfactory practices < 70%
The different levels of knowledge, attitude and practices (KAP) are categorized as follows:
Satisfactory knowledge, attitude and practices ≥ 70%
Unsatisfactory knowledge, attitude and practices < 70%
INTERVENTION
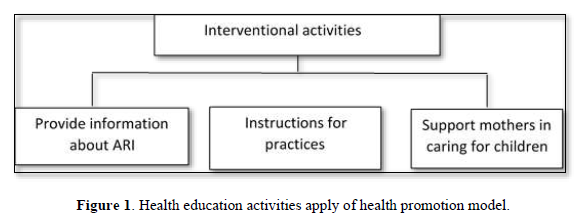
The educational intervention program includes theoretical lectures with PowerPoint presentations, short videos, folded pictures/leaflets and instructions for practices in caring and prevention of ARI for mothers. Interventional activities in many forms:
Large group: Each educational session was conducted within 90 min by pediatric experts/ health workers. The remaining time was for the practice group, the research team divided all members of the experimental group into small groups of 5-10 mothers/group to discuss and practices in caring for children with ARI.
Direct consultation for mothers at the commune health station and at mothers’ home
Indirect consultation via commune media, mobile phone, Zalo network, sending documents via email or social media.
Evaluating after intervention about caring and prevention of ARI after 12 months of intervention (Figure 1).
Research ethics: This study was approved by the Ethical Review Committee of Nam Dinh University of Nursing (no.2359/GCN-HĐĐD), and permission for data collection from the authorities of the community. Participants were informed verbally and in writing about the study’s aim and their role. All participants reviewed and signed the study informed consent form as their agreement to participate. Research respondents participated voluntarily and were free to withdraw from the study without consequence. During the post-intervention monitoring and evaluation period, the control group did not receive any form of intervention from us. However, after the end of the intervention period, we conducted health educational intervention for the control group.
Statistical analysis: All variables entered into the regression models were coded or transformed into categorical measurements. Collected data were coded and tabulated using a personal computer. Using an SPSS 25.0 program for Windows. Descriptive statistical analysis (Frequency, Percentage) and inferential statistical analysis (Chi square test) was used to analyze the data. In addition, the McNemar's test, and Chi-square test also were used to compare 2 proportions in evaluating intervention effectiveness. The result was projected with appropriate figure and tables.
RESULTS
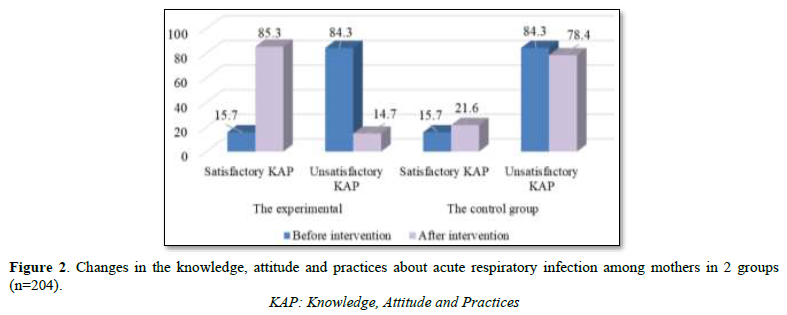
General characteristics of participants (Table 1-5 & Figure 2)




DISCUSSION
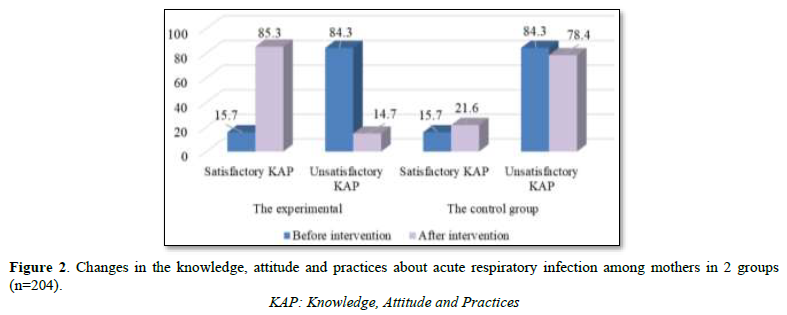
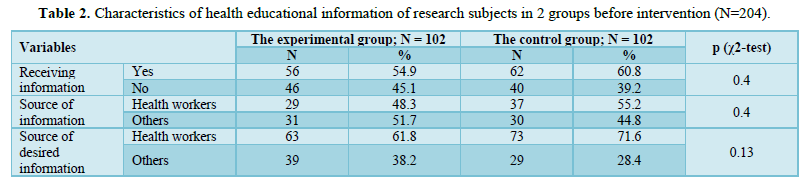
The result was no difference about the socio-demographic and educational health information characteristics of mothers between the experimental and the control group before the intervention. This difference was no statistically significant with p> 0.05. The proportion of mothers receiving health educational information about prevention and caring for children with ARI in the intervention group and the control group were 54.9% and 60.8%, respectively. A cross-sectional descriptive study on 132 mothers having children under 5 years old in Nepal about the knowledge and practice of managing ARI, the results showed that most of mothers had information about the disease (93%), including information sources from health workers accounted for 30%. The lack of knowledge about dangerous signs of the disease has led to a proposal for a community-based education program for mothers about ARI [11]. Therefore, it is necessary to strengthen and enhance the role of health workers in health education about ARI for mothers at the primary health level. Analysis results showed that mothers' knowledge about ARI in the experimental and control groups before intervention was not statistically significant with p> 0.05. After intervention, mothers' knowledge about ARI in the experimental group increased from 10.8% (before intervention) to 52.9% (after intervention). The difference was statistically significant with p< 0.05. The knowledge about ARI in the control group changed after intervention. The percentage of the satisfactory knowledge increased from 12.7% to 14.7%. However, the difference was not statistically significant with p> 0.05. The results reflect the effectiveness of the intervention that was similar to the study of author Raval B in 2015 about the intervention based on the structured training program with 45-min lectures for mothers with children under 5 years old, which improved knowledge compared to the results of 7 days after intervention. The study of Raval B and et al, indicated the mothers' knowledge was remain low: 52% mothers had poor knowledge, 48% mothers had average knowledge and no any mother had good knowledge. After the intervention, mothers' knowledge improved: good knowledge increased at 64%, fair knowledge increased at 36% and there were no any mother had poor knowledge [12]. The study of Bhatti Z.I and et al showed that the positive impact of educational interventions on knowledge of mothers regarding ARI and shows a prominent difference in pre and post knowledge scores of participants after an educational intervention [13]. The research of Tunny I.S in 2020 also showed the effectiveness of health educational intervention through leaflets to mothers, which can improve knowledge and increase awareness of ARI prevention for children [14]. The result was similar to the study of Mahalakshmi in 2023, the educational intervention program showed that the mothers' knowledge about ARI increased from 8.51 ± 4.59 (before intervention) to 19.31 ± 2.54 (after intervention) [15]. The percentage of satisfactory attitude of mothers about ARI was remain low (50%). This result was similar to the study of Saeed and et al in 2020, found 146 mothers (48.7%) had a good attitude about ARI [16]. After the intervention, the mothers’ attitude in the intervention group improved significantly. In the intervention group, the satisfactory attitude of mothers about ARI increased from 50.0% (before intervention) to 94.1% (after intervention). The difference was statistically significant with p < 0.05. After the intervention, the mothers’ attitude about ARI in the control group changed. The proportion of the satisfactory attitude increased from 58.8% to 63.7%. However, this difference was not statistically significant with p > 0.05. Our study revealed the mothers’ practices about ARI were low. After intervention, the satisfactory practices of mothers were improved significantly from 11.8% to 85.3% with p<0.001. The mothers’ knowledge, attitude and practices in the intervention group and control group were remain low. The percentage of satisfactory knowledge, attitude and practices (KAP) achieved in the experimental and control groups before intervention were 15.7%. This result was also consistent with the study of Mutalik A and Raje V. V in 2017, assessing knowledge, attitude and practices about ARI of mothers in the rural areas of Maharashtra [5]. The research showed that mothers' knowledge, attitude and practices about ARI were remain low. The percentage of mothers with poor knowledge, attitude and practices about ARI were high at 68.9%, 74.3%, and 68.9%, respectively. The number of mothers with unsatisfactory knowledge, attitude and practices (poor knowledge, attitude and practices) accounted for a high percentage of 71.6%. The satisfactory knowledge, attitude and practices of mothers were 28.4%. The average knowledge, attitude and practices were 20.3%. The percentage of mothers with good knowledge, attitude and practices were remain low at only 8.1%. Therefore, it is necessary to improve mothers' knowledge, attitude and practices about ARI. Furthermore, mothers are the primary caregivers for children in society. Thus, mothers' knowledge, attitude and practices have a significant influence on the disease status and survival in children [5]. In our study, there was no statistically significant difference between mothers' knowledge, attitude and practices about ARI in the 2 groups before intervention with p> 0.05. After the intervention, the knowledge, attitude and practices of mothers in the intervention group improved significantly: the satisfactory knowledge, attitude and practices of mothers about ARI increased from 15.7% to 85.3% compared to the satisfactory knowledge, attitude and practices in the control group increased from 15.7% to 21.6%. The results showed that there was an improvement in knowledge, attitude and practices of mothers in the experimental and control groups between before and after the intervention. This result may be explained by the time of the research was the period of the Covid-19 pandemic that was not under the control. Health information and educational programs implemented in the community have an impact on assessment results. However, the impact of this error factor can be eliminated due to the research performed the intervention with the control group. The research results were clearly improved in the intervention group between before and after the intervention and compared to the control group. Therefore, nurses need to strengthen health educational information for mothers about prevention and caring for children with ARI to improve knowledge, attitude and practices of mothers, contribute to reduce the incidence of ARI as well as improving the condition of ARI in under-five children. According to Pender's health promotion model [9], mothers reduce difficulties in caring for children and aware of the benefits of improving knowledge, attitude and practices about prevention and caring for children with ARI that lead to health-promoting behavior. At the same time, mothers are supported in caring for children with ARI at home which also contributes to create the advantages to perform health-promoting behaviors. Therefore, it is necessary to improve caring practices for children with ARI and create a favorable environment for mothers to perform behaviors that are beneficial to children's health which lead to improve children's health.
CONCLUSION
The knowledge, attitude and practices of mothers in the intervention group improved significantly after the intervention. Satisfactory knowledge, attitude and practices of mothers about prevention and caring for children with ARI increased from 15.7% to 85.3% in the intervention group. While the satisfactory knowledge, attitude and practices in the control group increased from 15.7% to 21.6%. The satisfactory knowledge, attitude and practices increased significantly compared to before intervention and compared to the control group. This research results illustrated the effectiveness of educational intervention based on the Health Promotion Model.
RECOMMENTDATION
From the results of the study, there are some recommendations as follows:
Health workers need to strengthen consultation and health education for mothers about the disease and prevention and caring for children with ARI in many different forms and means: direct consultation, distribute leaflets, guiding books, and indirect advices through the media, mobile phones, and social networks. At the same time, providing support in caring for children with ARI at home for mothers having children under 5 years old. Propose solutions to integrate the programs with activities to improve children's health in the community to increase the effectiveness of interventional programs, reduce the rate of serious illness/complications of ARI in children under 5 years old.
- Sarkar A, Bhavsar S (2017) Assessment of common childhood diseases in 1 - 5 yr age group children and determination of knownedge health care practices & health seeking behaviour of parents in Jamnagar dictrict. Glob J Res Anal 6(4): 53-55.
- Honglei H, Readon CI, Evelyn G, Thézénas ML, Jallow M, et al. (2014) Discovery and Validation of Biomarkers to Guide Clinical Management of Pneumonia in African Children, Published by Oxford University Press on behalf of the Infectious Diseases Society of America. Oxford J 58(12): 1707-1715.
- Gyawali M, Rama P, Safala M, Khadka RR (2016) Knowledge on acute respiratory infection among Mothers of under five-year children of Bhaktapur District, Nepal. Int J Sci Res Publ 6(02): 85-89.
- Alluqmani MA, Aloufi AA, Abdulwahab AMA (2017) Knowledge, Attitude and Practice of Mothers on Acute Respiratory Infection in Children under Five Years in Saudi Arabia. Egypt J Hosp Med 69(2): 1959-1963.
- Mutalik AV, Raje VV (2017) Study to assess the knowledge, attitude, and practice about acute respiratory infections among school going children and their parents in rural Maharashtra. Int J Med Sci Public Health 6(11): 1584-1587.
- Prasanna KL, Sharma NK (2014) Effectiveness Of Structured Teaching Programme Vs. Self Instructional Module Regarding Prevention Of Acute Respiratory Infections In Children Among Mothers. IOSR J Nurs Health Sci 3(1): 09-15.
- Lalisa CG, Sheka SS (2021) The Knowledge and Practice of Mothers Caring for their Children with Acute Respiratory Infection among those attending the Under-Five Unit at Bedele Hospital, Southwest Ethiopia. Clin Mother Child Health 18(7): 1-4.
- Alidha NR, Nita A, Meita D, Wiwaha G, Mutyara K, et al. (2020) A Qualitative Study on Family Role in the Care and Prevention of Acute Respiratory Infection Among Children in Primary Health Care. Glob Pediatr Health 7: 1-8.
- Pender NJ, Murdaugh CL, Parsons M.A (2015) Health promotion in nursing practice, University of Michigan, School of Nursing, Ann Arbor, Michigan, pp: 26-53.
- World Health Organization (2014) World Health Organization guidelines, Infection prevention and control of epidemic- and pandemic-prone acute respiratory infections in health care. Geneva 2014; WHO. Available online at: who.int
- Acharya D, Ghimire UC và, Gautam S (2014) Knowledge and practice of management of acute respiratory infection among mothers of under five years children in rural Nepal. Sci J Biol Sci 3(1): 11-16.
- Raval B, Pandya A, Ravindra HN (2015) A Study to assess the effectiveness of Structured Teaching Programme on Knowledge Regarding Acute Respiratory Tract Infection among Mothers of Under Five Children at Piparia, Vadodara. Int J Nurs Educ 7(3): 51-55.
- Bhatti ZI, Nawaz K, Ali M, Bhatti SZ (2020) Effectiveness of Educational Interventions on Knowledge Towards Prevention of Acute Respiratory Tract Infection among the mothers of under five year children. PJMHS 14(3): 672-674.
- Tunny IS, Soamole I, Wibowo SA, Purnamasari I, Rumaolat W (2020) Effect of Health Education on Mothers’ Knowledge in the Prevention of Acute Respiratory Infection in Toddlers in Waimital Village, Maluku. Jurnal Ners 15 (Speacial issue 02): 188-192.
- Mahalakshmi B, Bharatbhai PN, Sivasubramanian N, Ramalakshmi G, Krishnan A, et al. (2023) Awareness among mothers on acute respiratory tract infections in under five children at north Gujarat, India. Bioinformation 19(6): 713-715.
- Saeed Esraa AM, Awadalla H (2020) Knowledge, Attitude and, Practice among Mothers of Under- Five Children about Acute Lower Respiratory Tract Infections an a Locality in Khartoum Urban Area, Sudan. J Environ Sci Public Health 4(4): 455-468.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5




QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Journal of Pathology and Toxicology Research
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)


