728
Views & Citations10
Likes & Shares
Results: The education levels and smoking status of office workers affected the occurrence of COPD. On the other hand, the income level of self-employed workers affected the occurrence of COPD and the smoking status did not. There was a difference in smoking status between office workers and self-employed workers. There was also a difference in the proportional risk of COPD according to the smoking status of office workers. There were more cases where office workers were currently smoking than self-employed workers, and there were differences in COPD incidence by smoking status. Unlike non-smoking and past smoking status, COPD incidence continued to increase from the start of observation.
Conclusion: The results of this study can be used to encourage the general public's awareness of the risk of COPD and induce long-term smokers to quit smoking. In addition, based on the results of this study, nurses should educate smokers about the need to periodically perform pulmonary function tests (PFT) in clinical, community settings and the cycle of performing PFT leading to COPD prevention and early diagnosis.
Keywords: Chronic obstructive pulmonary disease, Pulmonary function test, Smoking, Office workers, Self-employed workers, Job
Abbreviations: COPD: Chronic Obstructive Pulmonary Disease; PFT: Pulmonary Function Test
Chronic obstructive pulmonary disease (COPD) is caused by chronic inflammation of the airway, lung parenchyma and pulmonary blood vessels, resulting in lung damage to the lungs. Smoking is known to be the main factor in causing this chronic inflammation [1]. Exposure to harmful dust and gasses from cigarette smoke overtime causes chronic inflammation, resulting in destruction of lung tissue, suppression of defense and recovery mechanisms. It damages lung tissue resulting in hyper secretion of mucus, airway stenosis and fibrosis. Furthermore destruction of lung parenchyma and changes in blood vessels, resulting in chronic obstructive pulmonary disease due to decreased expiratory flow [2]. According to the 2016 National Health and Nutrition Survey report, the prevalence of chronic obstructive pulmonary disease in Koreans is 19.6% for men and 5.8% for women, with one in five men being sick, about three times that of women [3]. It is noteworthy that the significant difference in smoking rate in 2018 between men and women was 37.7% and 3.5% respectively [4].
Spirometry is one of most common pulmonary function tests (PFT) that can diagnose COPD and confirm the progress of lung function reduction. It checks and detects airway obstruction from clinical symptoms of dyspnea, chronic cough, sputum or exposure to harmful substances such as smoking [5]. According to the COPD guidelines from The Korean Academy of Tuberculosis and Respiratory Diseases, lung capacity are easy to measure and the best way to measure airflow limitation. If the ratio of FEV1/FVC is less than 0.70 then it will be diagnosed as COPD [6]. When diagnosed COPD patients undergo pulmonary function tests, treatment commences with airflow restriction to prevent symptoms from worsening [7]. In order to prevent COPD, it is necessary to take pulmonary function tests before any clinical symptoms appear. Changes in lifestyle might be advised and followed based on test results.
From previous studies, different smoking statuses (current smoker, former smoker, never smoked) and their occupation have been linked to COPD. In a study that analyzed health behavior between health insurance subscribers (regular workers) and local subscribers (self-employed). It found that local subscribers smoked more than health insurance subscribers [8]. In a study that analyzed smoking statuses by occupation in Korea’s five major cities, office workers, public officials, and professionals had a high non-smoking rate, but self-employed workers had a high smoking rate [9]. On the other hand, health insurance subscribers have a higher frequency of smoking with one of the main factors being the quality of life between the different occupational groups [10]. Recently, the prolonged social distancing due to COVID-19 has affected people's lives worldwide and increased the risk of mental health [11]. In particular, self-employed people were directly affected by the economic impact and found to have significant stress [12]. Due to the economic difficulties of self-employed people, non-smokers may start smoking or the smoking intensity of existing smokers may increase [13].
COPD is a progressive disease and is estimated to be the third leading cause of death worldwide in 2020 but the cause factors are relatively clear and preventable [5]. Therefore, smoking cessation is recommended first for COPD patients, but 55.1% of Korean smokers have no smoking cessation plan at the moment when looking at the will of Korean adults to quit smoking in 2019. In addition, 36.2% of smokers have a smoking cessation plan someday, although not within 6 months even if they have a smoking cessation plan, which is not specific even if most smokers do not have a smoking cessation plan, and 43.6% of them have a low smoking cessation attempt [14]. COPD is a chronic disease with a high prevalence and mortality rate, and active intervention is needed, such as not only treating patients in medical institutions but also inducing lifestyle changes such as smoking cessation such as chronic diseases such as diabetes and high blood pressure. Therefore, it is necessary to check the period until a smoker is diagnosed with COPD and regularly perform lung function tests before being diagnosed to check the degree of airway obstruction and detect it early. In addition, when confirming the degree of airway obstruction of smokers through objective test results, smokers may be motivated to quit smoking to prevent COPD.
Most of the studies on smoking and COPD have been conducted on the search for the cause of COPD [15,16], and studies have been conducted to analyze the factors affecting the death of COPD patients [17,18]. Therefore, it was found that one of the biggest causes of COPD was smoking, but it is difficult to find a study on when COPD occurs depending on the amount of smoking and the duration of smoking. If the time when COPD occurs is known, depending on the amount of smoking and the duration of smoking, it will be more helpful in understanding the cycle that smokers should proceed with PFT, to prevent COPD.
Purpose of the study
The purpose of the longitudinal study is to present lung function test cycles to two cohort groups; smoking statuses of adult office workers and self-employed workers in their 40s respectively. In turn cumulative incidence and proportional risk of chronic obstructive pulmonary disease could be identified within these two groups.
MATERIALS AND METHODS
Research Design
This study is a prospective cohort study to confirm the lung function test cycle to prevent chronic obstructive pulmonary disease due to smoking conditions of adult office workers and self-employed workers in their 40s using data from the 6th Korean Genome Epidemiology Study (KoGES) every 2 years conducted from 2001 to 2014.
Research data and targets
- Community-based cohort data of the Korean Genome Epidemiology Study (KoGES)
The Korean Genome and Epidemiology Study (KoGES) of the National Institute of Health at the Korea Disease Control and Prevention Agency is the largest cohort study in Korea to identify risk factors for chronic diseases common to Koreans. It establishes scientific guidelines for preventing chronic diseases. KoGES' community-based cohort was conducted in Ansan and Anseong on a two-year basis, starting with the 2001 base survey. Ansan-si is a rural area with a combination of industrial complexes, commercial areas and small-scale agriculture. The age and gender demographics within Ansan-si were evenly distributed with low population movement. KoGES' community-based cohort data, constructed through this process and used for analysis in this study. Since the data was reliable therefore it can be representative of Korea. In this study, since the results of the lung function test confirmed whether there was a residue of chronic obstructive pulmonary disease (COPD), it was analyzed using the 6th follow-up data, excluding the 7th and 8th follow-up data that were not investigated. This is because survey results of PFT were not included.
- Selection of research subjects
The subjects of the study were selected as those who did not have a history of being diagnosed with COPD among 40-year-old adults at the time in 2001 base survey of the KoGES community-based cohort. The job was divided into office workers (office workers, sales workers, production workers and professional workers) and self-employed workers (agriculture, self-employment and other self-employed type of roles) as responding to the question, "What kind of job are you in?" In the base survey, if the essential information on demographic characteristics, smoking status and COPD diagnosis were not populated then it was treated as incomplete and excluded from the study. In addition, the timing of the new chronic obstructive pulmonary disease was confirmed, excluding those who did not participate in the follow-up at least once, those who had a history of COPD diagnosis before the base investigation and those with a ratio of FEV1 to FVC of less than 70% (Figure 1).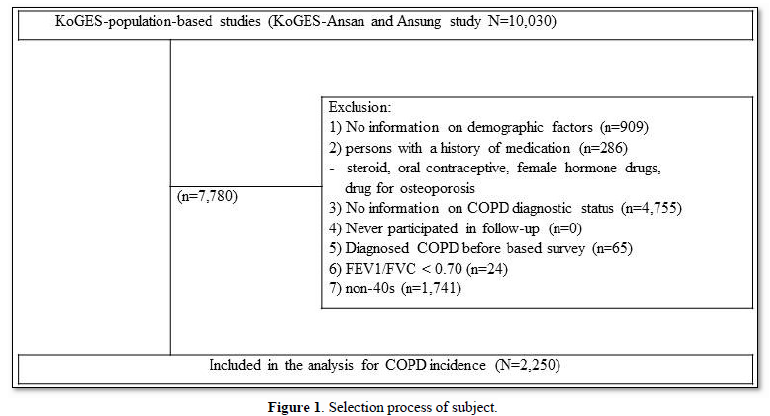
- Tracking observation period and time
The follow-up period was from the start of participation in the base survey of community-based cohorts to the end of follow-up. This was the first diagnosed period to the sixth follow-up with the follow-up stopped due to several reasons such as moving, refusing to participate and death (Figure 2).
Variables in the study
- Independent variable
The independent variables are demographic characteristics and smoking status. The demographic characteristics can act as confusion variables in the occurrence of COPD in Korean adult smokers. This includes gender, spouse presence, education level, and income level and body mass index. The age of the subject was selected for adults in their 40s in a community-based cohort. The presence or absence of a spouse was categorized as "no spouse" in response to the question "How is your current marital status?" and "no spouse" in response to "unmarried, bereavement, separation, divorce, etc." The education level was categorized as elementary school graduation, middle school graduation, high school graduation and college graduation. While income level was categorized as less than 1 million won per month, more than 1 million won to 3 million won per month and more than 6 million won per month. The body mass index was categorized into underweight (less than 25), standard weight (more than 25 to less than 30) and obese (more than 30).
As of the time of the 2001 base survey, those who answered "I have never smoked at all" were classified into non-smoking groups, those who answered "I have smoking experience but don't smoke now" were classified into past smoking groups, and those who answered "I smoke sometimes" and "I continue to smoke habitually" is classified into current smoking groups. Furthermore, the current smoking group was defined into less than 20 packs and more than 20 packs, calculated as "the number of packs smoked per day × the total number of years of smoking" based on the evidence [19]. In other words, it was divided into four groups: non-smoking group, past smoking group, current smoking group (less than 20 pack years), and current smoking group (more than 20 pack years).
- Dependent variable
In this study, the dependent variable is the occurrence of chronic obstructive pulmonary disease. For the occurrence of chronic obstructive pulmonary disease, the time when the ratio of FEV1 to FVC was measured to be less than 70% based on lung function test results was the time when the disease occurred. The period until chronic obstructive pulmonary disease occurred was the period when the ratio of FEV1 to FVC was less than 70%, subtracting the base investigation time from the first measured survey time.
Data analysis method
For data analysis, SPSS statistics 23 were used to review the demographic characteristics and smoking status of these subjects which were confirmed as the frequency and percentage. The cumulative incidence of chronic obstructive pulmonary disease according to the smoking status of adult office workers and self-employed people in their 40s was identified using Kaplan-Meier curve analysis. The homogeneity of the survival curve by smoking status was confirmed using the log-rank test. In addition, the proportional risk of chronic obstructive pulmonary disease among adult office workers and self-employed workers in their 40s was confirmed by Cox's professional hazard regression model. The measure fitting of the data was to verify that Cox's professional hazard regression model satisfies the basic assumptions used in a significance test on the interaction between covariates and time through the Log Minus Log survival plot (LML plot) and also the time-dependent Cox regression model.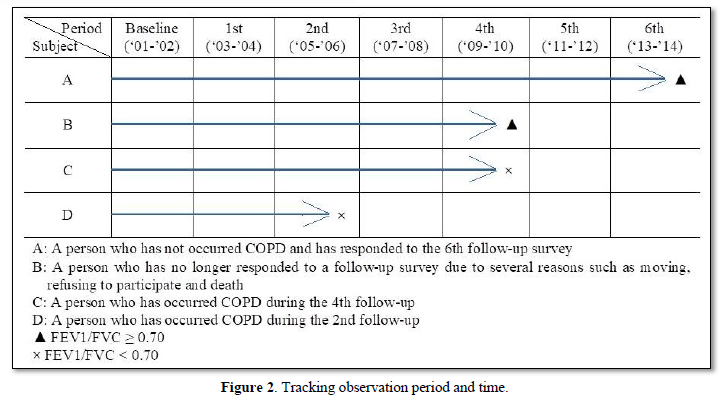
- Cumulative incidence
The cumulative incidence rate is confirmed by Kaplan-Meier curve analysis, which calculates the cumulative incidence rate by listing the study subjects in the order of short observation period and multiplying the incidence rate at each point at which the disease occurs. The time is displayed on the X-axis. The disease incidence rate at each point in time is displayed on the Y-axis and at each point in time; a cumulative occurrence curve appears in the shape of a staircase [20]. The Log-rank Test checks whether the survival curve is statistically significant between each group shows [20]. When it is statistically significant, there is a difference in the COPD cumulative incidence according to the smoking status of adult office workers and self-employed people in their 40s compared with the Log-rank Test.
- Survival analysis
Survival analysis is used as one of the time-series analysis methods that observe and analyze the occurrence of a specific disease over time in longitudinal studies. In other words, when the occurrence of a disease changes over time, it is a method of analyzing the probability of occurrence of a disease using it as a function of time [20]. In the survival analysis, Cox's professional hazard regression model is used as the ultimate target of interest in survival and survival period corresponding to the occurrence of disease. This is a multivariate analysis technique that models the effect of independent variables on outcome variables by identifying factors related to the occurrence of a specific disease. Thus quantifying and evaluating the effect of complex effects on the incidence of the disease at relative risk. The goodness-of-fit test of Cox's professional hazard regression model was interpreted to check whether each curve in the smoking state was maintained vertically at a certain distance using the Log Minus Log survival plot (LML Plot). In addition, through the time-dependent cox regression model, the significance probability of COPD incidence proportional risk according to smoking status was confirmed and it was judged that the assumption of proportional risk was satisfied due to not being statistically significant.
Ethical considerations
The contents and methods of this study were approved by the Research Ethics Deliberation Committee. The KoGES data used in the study was used only for research purposes and the study was conducted after obtaining approval from KoGES through various procedures necessary. During the study, the data was not used for profit by individuals, institutions and personal information was protected by not lending or transferring it to others. In addition, after the study was completed, a confirmation of data disposal was submitted to the Korea Centers for Disease Control and Prevention to discard the data used in the study.
RESULTS
Demographic and sociological characteristics according to smoking status of adult office workers and self-employed people in their 40s
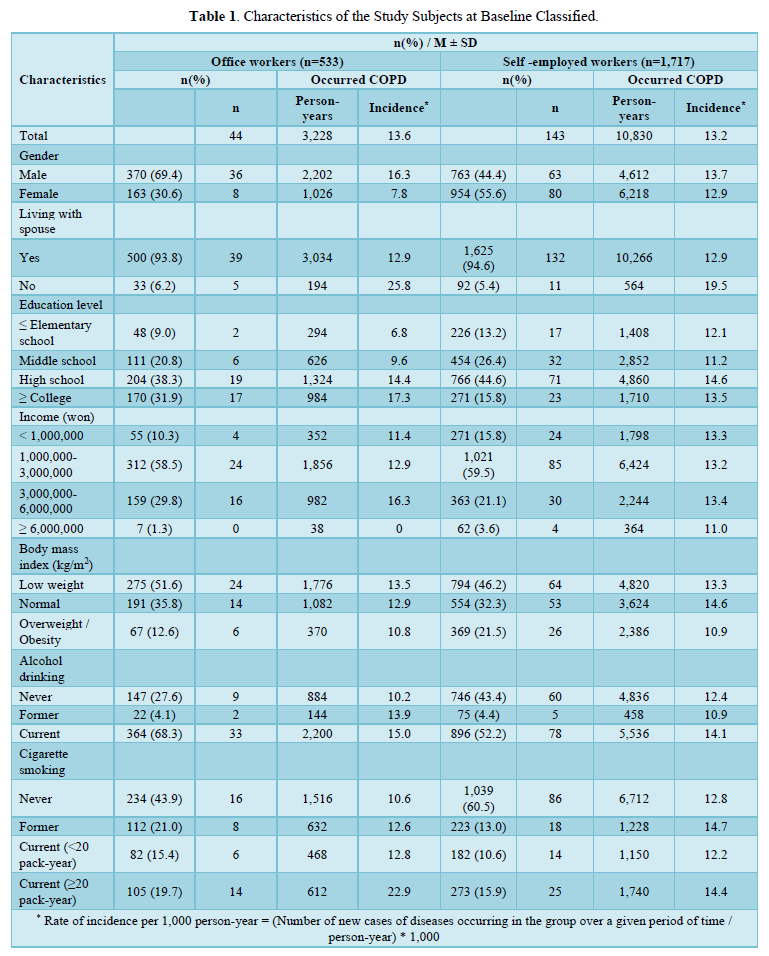
As a result of the data analysis, out of 2,250 adults in their 40s, 533 were office workers and 1,717 were self-employed. Among office workers and self-employed workers who had COPD were 44 and 143 respectively. As for office workers, 69.4% were men and 30.6% were women with 93.8% having a spouse. Education levels below elementary school, middle school and above high school were 9.0%, 20.8% and 38.3% respectively. Monthly income below 1 million won was 10.3%, 58.5% above 1 million won, 29.8% above 3 million won and 1.3% above 6 million won. The body mass index was 51.6% for those with low weight, 35.8% for those with normal weight and 12.6% for overweight and obesity. Non-drinking was 27.6% for non-drinking, 4.1% for past drinking, 68.3% for current drinking, 43.9% for non-smoking, 21.0% for past smoking, 15.4% for under 20 packs of current smoking, and 19.7% for over 20 packs of current smoking (Table 1).
For self-employed people, 44.4% were men and 55.6% were women, and 94.6% were people with spouses. The education level below elementary school was 13.2%, the education level of middle school was 26.4%, the education level of high school was 44.6%, and the education level above university was 15.8%, the monthly income was 15.8%, 59.5% from 1 million won to 3 million won, and 3.6% from 3 million won to 6 million won. The body mass index was 46.2% for those with low weight, 32.3% for those with normal weight, and 21.5% for overweight and obesity. Non-drinking was 43.4% for non-drinking, 4.4% for past drinking, 52.2% for current drinking, 60.5% for non-smoking, 13.0% for past smoking, 10.6% for under 20 packs of current smoking, and 15.9% for over 20 packs of current smoking (Table 2).
The cumulative incidence of chronic obstructive pulmonary disease according to the smoking status of adult office workers and self-employed people in their 40s
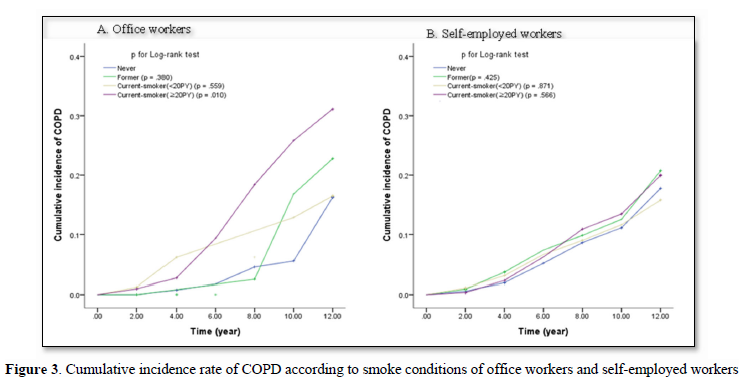
From the Kaplan-Meier curve, the incidence rate was calculated each time COPD occurred based on their smoking status with their cumulative incidence rate estimated and schematized (Figure 3).
The identity of the estimated survival curve according to the smoking status was confirmed by the log-rank test. As a result we identified differences according to the smoking status of adult office workers in their 40s. The difference by group was (p=.010) with no difference in the identity of the survival curve according to the smoking status of the self-employed (p=.698).
Proportional risk of chronic obstructive pulmonary disease due to smoking status of adult office workers and self-employed people in their 40s
The total number of adult COPD outbreaks in their 40s with observation period for office workers and self-employed workers was 3,228 and 10,830 respectively. The COPD incidence rate was 13.6 for office workers and 13.2 for self-employed workers per 1,000 people. Two types of model fitness tests were used; firstly in the LML plot, this showed that the smoking status remained at a certain distance, satisfying the proportional risk assumption. Secondly, in the time-dependent cox regression model, the significance probability of smoking status was not statistically significant.
In order to correct the general characteristics in Cox's professional hazard regression, a proportional risk regression analysis was conducted with the multivariate model, including all independent variables, and the risk of COPD was statistically significant. In other words, current smokers had a 5.28 times higher risk of developing COPD than non-smokers (95% CI=1.49-18.70, p=.010).
DISCUSSION
Smoking is one of the most dangerous factors for COPD to occur and there is a difference in smoking status between office workers and self-employed workers. The fact that the smoking status varies depending on the job means that the risk of COPD from smoking may vary depending on the job. Currently, Korea's health examination system by life cycle recommends that checkups be conducted at regular intervals to prevent diseases that may be common to Koreans. In addition, prompting the entire nation to actively participate in health checkups. However, the prevalence of COPD in Koreans is currently high at about 19% but not included in the examination in order to prevent and diagnose it early. COPD is a disease that has relatively clear causes and can slow and prevent the progression of the disease due to early detection [21]. By preventing diseases through periodic lung function tests, the cost and effort effect can be great. Therefore, it is necessary to actively educate and promote the cycle of lung function tests by identifying the frequency of disease occurrence for the prevention and early diagnosis of CODP of office smokers.
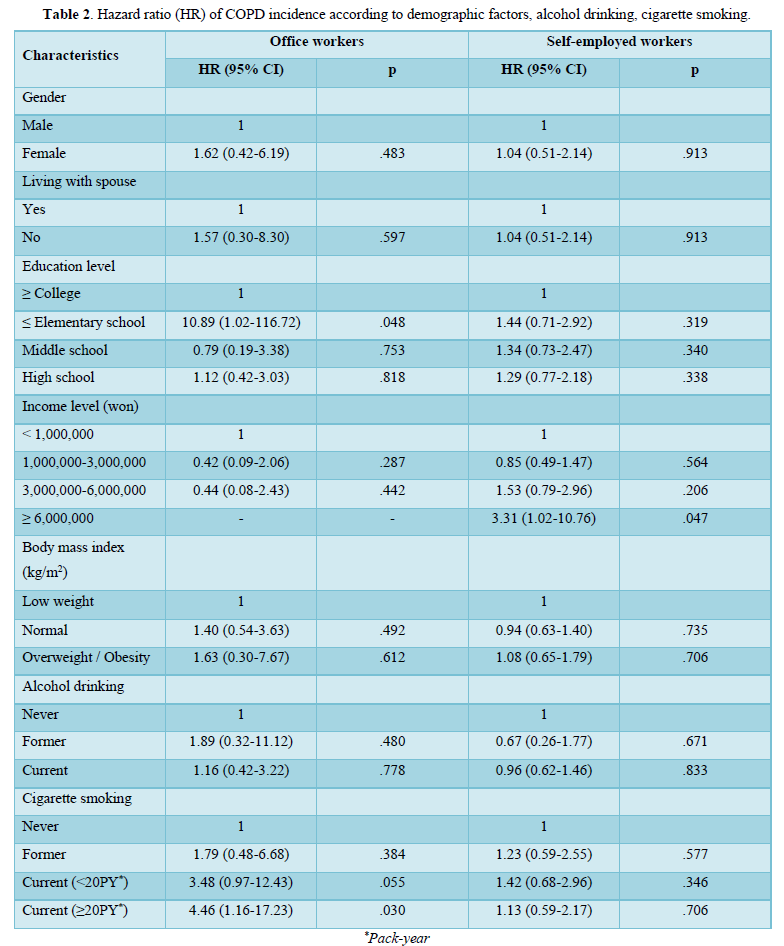
In the results of this study, the education levels and smoking status of office workers affected the occurrence of COPD. On the other hand, the income level of self-employed workers affected the occurrence of COPD and the smoking status did not. In other words, those below the elementary school education level among office workers had a 10.9 times higher risk of developing COPD than those above the university education level and those over 20 packs of smoking status had a 4.5 times higher risk of developing COPD than non-smoking status. Office workers are more likely to have a higher alcohol consumption rate and currently smoke more than self-employed workers. In a previous study that confirmed the smoking rate according to the education level of the adults using data from the National Health and Nutrition Examination Survey (NHANES), the education level was higher for the non-smoking group [22]. These preceding studies support the results of this study that the educational level of office workers is related to the occurrence of COPD, and that low education levels can lead to high smoking rates and high COPD incidence. In the results of this study, income levels seem to affect the occurrence of COPD for self-employed workers. Even COPD patients are aware of the harmfulness of smoking to COPD, but it is difficult to change smoking habits to smoking cessation due to stress such as working life [23]. In addition, if the income level is more than 6 million won per month among self-employed workers, the risk of COPD was about 3.3 times higher than that of less than 1 million won per month. In most previous studies, the lower the income, the more COPD occurred [24,25], but this study showed the opposite result. The reason why the results of this study are different from previous studies is that the age of the study subjects was limited to adults in their 40s.
In this study and in previous studies, there was a difference in smoking status between office workers and self-employed workers. There was also a difference in the proportional risk of COPD according to the smoking status of office workers. There were more cases where office workers were currently smoking than self-employed workers, and there were differences in COPD incidence by smoking status. Unlike non-smoking and past smoking status, COPD incidence continued to increase from the start of observation. This was similar to the results of previous studies that lung function decreased as the smoking period increased [26]. In addition, when the current smoking status was divided into less than 20 packs and more than 20 packs, the incidence of COPD in smokers increased significantly for more than 20 packs after 6 years of observation, which was statistically significantly different from that of non-smokers. In other words, the longer the smoking period and the greater the amount, the higher the risk of COPD than those who do not smoke. This study tracked the same subjects every two years and confirmed whether COPD occurred every two years. In the case of smokers, the incidence of COPD increases rapidly every follow-up cycle compared to non-smokers, so it should be recommended that smokers conduct pulmonary function tests during medical checkups for COPD prevention and early diagnosis. Currently, pulmonary function tests are not included in the mandatory items of national health examination in Korea, which may causes an economic burden on the examinee. Therefore, there is a need for institutional changes that can actively conduct checkups for smokers.
CONCLUSIONS
COPD is a disease with a high mortality rate worldwide, and if symptoms appear and are diagnosed, the disease is in progress. In addition, even if coughing and shortness of breath appear, it is difficult to diagnose early because it is thought that it is because of smoking or aging. Therefore, lung function tests used to diagnose COPD should be regularly performed to recommend COPD prevention and early diagnosis of people with risk factors for COPD development. In addition, factors that cause COPD, such as smoking, should be removed and regular hospital visits should be recommended to observe the incidence and progress of the disease.
However, there is no research on the lung function test cycle of smokers and the focus is on treatment rather than prevention with smoking cessation recommended after diagnosis in COPD. In addition, the general public's awareness of COPD is relatively low and resource information on diseases is insufficient. Therefore, it is necessary to inform people about the risk of COPD and educate them that PFT should be regularly performed for the prevention and early diagnosis of people with risk factors.
Therefore, the results of this study can be used to encourage the general public's awareness of the risk of COPD and induce long-term smokers to quit smoking. In addition, based on the results of this study, nurses should educate smokers about the need to periodically perform PFT in clinical, community settings and the cycle of performing PFT leading to COPD prevention and early diagnosis. The role of these nurses may contribute to lowering the mortality and incidence of COPD. This study has a limitation that data analysis before COVID-19 does not reflect the pandemic and it is necessary to study by adding a flow-up period by reflecting changes in smoking status after COVID-19.
- Donald PT, Thomas G, Alyssa B, Barry P, Ayca O-G, et al. (2019) Effect of smoking status on ling function, patient-reported outcomes, and safety among COPD patients treated with glycopyrrolate inhalation powder: Pooled analysis of GEM1 and GEM2 studies. Respir Med 20(1): 135-145.
- Kim HK, Lee SD (2005) Pathophysiology of chronic obstructive pulmonary disease. Tuberc Respir Dis 59(1): 5-13.
- Korea Centers for Disease Control and Prevention (2017) Ministry of Health and Welfare. 2016 Health behavior and chronic disease statistics. Report No. : 11-1352159-000313-01.
- Statistics Korea (2018) Rate of smoking [Internet]. Daejeon: Statistics Korea. Accessed on: July 05, 2020. Available online at: http://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_2KAAC04_OECD&conn_path=I2
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) (2019) Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2020 report). GOLD. Report No. : 979-8607447106.
- Committee for Amendment of COPD diagnostic Guidelines (2018) Guidelines for COPD diagnosis. The Korean Academy of Tuberculosis and Respiratory Disease. Report No. : 979-11-953666-9-9 93510.
- Moon JY (2016) Screening test for early diagnosis of COPD. Obstruct Lung Dis Res Foundation 4(2): 65-70.
- Kim JW (2018) Affecting factors to healthcare utilization depending enrollment type. Korean J Public Health 55(1): 33-41.
- Jung BM, Lim SS, Kim ES (2002) A survey on health management and life habits for the urban salaried workers. J Korean Soc Food Sci Nutr 31(3): 482-491.
- Kwon MJ, Kim SA (2019) Convergence factors affecting quality of life of wage worker and self-employed. J Korea Convergence Soc 10(9): 333-342.
- Holmers EA, O'Connor RC, Perry VH, Tracey I, Wessely S, et al. (2020) Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 7(6): 547-560.
- Nam JH, Lee RH (2020) Is the COVID-29's impact equal to all in South Korea? Korean J Soc Welfare 72(4): 215-241.
- Kwon MY, Cho MS (2022) Factors associating to the increased smoking time among South Korean male workers during COVID-19 pandemic. Korean J Health Educ Promot 39(2): 53-64.
- Statistics Korea (2019) Whether to try to quit smoking and a smoking cessation plan [Internet]. Daejeon: Statistics Korea. Accessed on: July 05, 2020. Available online at: http://kosis.kr/statHtml/statHtml.do?orgId=605&tblId=DT_60502_150307&conn_path=I2
- Hans P, Akshay S, Paula M, Xian S, Yan C, et al. (2014) Rapid lung function decline in smokers is a risk factor for COPD and is attenuated by angiotensin-converting enzyme inhibitor use. Chest 145(4): 695-703.
- Jordi O, Sergio J, Viviana P, Elizabeth CC, Gonzalo V, et al. (2018) Comparative analysis of COPD associated with tobacco smoking, biomass smoke exposure or both. Cell Physiol Biochem 50(3): 1140-1153.
- Nizet TAC, van den Elshout FJJ, Heijdra YF, van de Ven MJT, Mulder PGH, et al. (2005) Survival of chronic hypercapnic COPD patients is predicted by smoking habits, comorbidity, and hypoxemia. Chest 127(6): 1904-1910.
- Godtfredsen NS, Lam TH, Hansel TT, Leon ME, Gray N, et al. (2008) COPD-related morbidity and mortality after smoking cessation: status of the evidence. Eur Respir J 32(4): 844-853.
- Lee KH (2009) Diagnosis of chronic obstruction pulmonary disease. Korean J Med 77(4): 401-406.
- Yoo KY (2013) Understanding medical statistics. (1st ed), Korea: Hannarae Publishing Coperation. pp: 235-251.
- Kim IA, Park YB, Yoo KH (2018) Pharmacotherapy for chronic obstructive pulmonary disease. J Korea Med Assoc 61(9): 545-551.
- Jeong DH, Park SH (2020) The smoking rate of the elderly according to the level of education and income: Using the 2018 National Health and Nutrition Survey Data. J Soc Occup Ther Aged Dementia 14(2): 117-123.
- Noh HJ, Kim SH, Joung WJ (2020) Disease awareness and treatment experience of patients with chronic obstructive pulmonary disease. J Korean Acad Fund Nurs 27(2): 188-197.
- Jung YM, Lee H (2011) Chronic Obstructive Pulmonary Disease in Korea: Prevalence, risk factors, and quality of life. J Korean Soc Nurs Sci 41(2): 149-156.
- Aizhamal T, John RH, Soriano JB, William C, Erick W-CH, et al. (2021) Gaps in COPD guidelines of low-and middle-income countries: A systematic scoping review. Chest 159(2): 575-584.
- Hwang YH, Oh JH (2018) Effect of smoking duration, smoked cigarettes per day and cessation period on pulmonary function in ex-smokers: Based on the 6th Korea National Health and Nutrition Examination Survey Data (KNHANES, 2016). J Korean Biol Nurs Sci 20(4): 214-220.
-
 Table 1
Table 1 -
Table 2





QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- International Journal of Diabetes (ISSN: 2644-3031)


