844
Views & Citations10
Likes & Shares
Background:
Hepatitis B virus (HBV) remains a major public health problem worldwide that
accounts for significant morbidity and mortality. About one third of the world
population have serological evidence of past or present hepatitis B virus
infection and more than 350 million people may be affected by chronic HBV
infection. The aim of this study was to detect the prevalence of hepatitis B
virus among febrile malaria and typhoid negative patients in Atbara city, River
Nile State, northern Sudan.
Material
and methods: A total of 89 blood samples were collected from
febrile malaria and typhoid negative patients including 44 females and 45
males. Sandwich Enzyme Linked Immunosorbent Assay (ELISA) was used to detect
Hepatitis B Surface Antigen (HBsAg) and competitive ELISA to detect Hepatitis B
Core Antibody (HBcAb) antibodies. Detection of HBV-DNA was carried out by Real
time-PCR and Conventional-PCR.
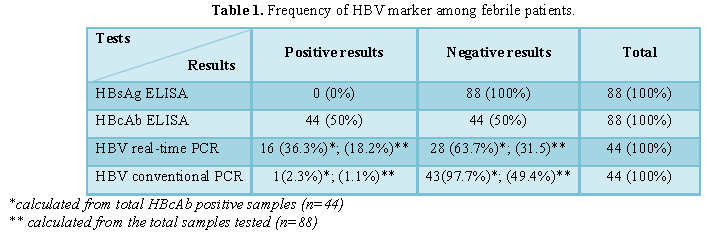
Results: Out of
88 samples, 44 (50%) samples were positive for HBcAb and all samples were
negative for HBsAg. HBV DNA was detected in 16 (18.2%) and 1 (1.1%) of the
samples using real time-PCR and conventional-PCR, respectively.
Conclusion: This
study had showed high prevalence of Occult Hepatitis B infection (OBI) among
febrile patients in Atbara town northern State where hepatitis B infection
seems to be endemic.
Keywords: Hepatitis B virus, Occult hepatitis B, Febrile patients, Atbara,
Sudan
INTRODUCTION
HBV is a double stranded DNA virus classified
in the virus family Hepadnaviridae.
HBV infection may result in subclinical or asymptomatic infection,
acute self-limited hepatitis, fulminant hepatitis or chronic hepatitis which
can lead to cirrhosis or hepatocellular carcinoma [1,2]. Signs and symptoms of
acute hepatitis include nausea, abdominal pain, vomiting, fever, jaundice and
dark urine, changes in stool color and hepatomegaly or splenomegaly [3].
Hepatitis B viral infection is endemic in the
developing countries of Africa [4]; the highest endemicity (>8%) is seen in
some sub-Saharan countries such as Nigeria, Namibia, Gabon, Cameroon, Burkina
Faso. Other countries like Kenya, Zambia, The Ivory Coast, Liberia, Sierra
Leone and Senegal are considered areas of intermediate endemicity (2%-8%),
while low endemicity level (<2%) was shown in Egypt, Tunisia, Algeria and
Morocco, located in the north of the continent. Sudan is classified among the
African countries with high HBV endemicity [5]. According to the most recent
World Health Organization estimate, two billion people worldwide have serologic
evidence of past or present HBV infection 360 million are chronically infected
and at risk for HBV-related liver disease. And approximately 600,000 die each
year [3].
HBV is transmitted by percutaneous or mucosal
exposure to infected blood or other
body fluids, it has been observed
The aim of this study was to detect the
prevalence of hepatitis B virus among febrile malaria and typhoid negative
patients in Atbara city, Sudan.
MATERIAL AND METHODS
Study area
This study was conducted in different health
centers in Atbara city, northern Sudan during the period of July to December
2018.
Study population and
sample size
A total of 88 blood samples were collected
from febrile malaria and typhoid negative patients including 44 females and 45
males. The age of the patients ranged between 15-60 years.
Most of the patients complained of fever and
other symptoms like headache and general body pain. All relevant information
including personal data such as name, gender were collected from each patient
after obtaining full consent.
5 ml blood samples were collected in EDTA
tubes from each patient and centrifuged at 3000 rpm for 5 min. Obtained plasma
was then stored at -20°C until used.
Serological testing
Commercial ELISA kits; Diagnostic Bioprobe
(Italy) and Diagnostic Automation/Cortez Diagnostics (USA) were used for
detection of HBsAg and HBcAb, respectively according to the manufacturers’
instructions. All positive samples for HBcAb were then tested for HBV DNA using
real time-PCR and conventional-PCR.
Heat treatment of
plasma samples
Substrate for HBV real-time and conventional
PCR was prepared by heat treatment of plasma without DNA extraction [9]. In
brief, 25 µL of specimens was diluted 2-fold with nuclease-free water. The
mixture was briefly vortexed and heated at 95°C for 5 min, then at 100°C for
approximately 5 min. The mixture was then centrifuged at 12 000 g for 3 min.
The supernatant was reserved and 5 µL were used in RT-PCR and conventional PCR
for detection of HBV DNA.
Real-time PCR
Detection of HBV DNA was performed using
real-time PCR on the Rotor 5 plex real-time PCR machine (Germany) according to
the protocol developed by Garson et al. [10]. Commercial kit (innuMIX Q PCR
MasterMi`x probe_analytic jena_Germany) was used according to manufactures
protocol. Amplification and detection was carried out under the following
cycling conditions: 1 cycle of 95°C for 15 min and 45 cycles of 95°C for 15 s
and 60°C for 60 s.
Conventional PCR
The PCR was performed using primers that are
specific for the HBsAg gene of HBV. The primers used consisted of forward
primer 5’TCGGAAATACACCTCCTTTCCATGG3’ (HBV genome 1353-1377) and reverse primer,
3’GCCTCAAGGTCGGTCGTTGACA-5’ (HBV genome 1702-1681). The reaction was performed
in 25 μl volume using (iNtRON, Korea) master mix. The volume included: 5 μl
master mix, 1 μl forward primer, 1 μl reverse primer, 5 μl extracted DNA and 13
μl distilled water.
The DNA was amplified in thermo cycling
conditions using PCR machine Heal force-classic (China) as follows: initial
denaturation at 94°C for 5 min, followed by 35 cycles of denaturation at 94°C
for 1 min, annealing at 62°C for 1 min and extension at 72°C for 1 min, with a
final extension step at 72°C for 7 min.
5 μl of the amplified product was then
subjected to direct analysis by gel electrophoresis in 2% Agarose gel, and
visualized by staining with Ethidium bromide using UV gel documentation system
INGeNius (Synoptics Limited, England). The expected size of the surface antigen
gene (HBsAg gene) amplicon was 350 bp.
RESULTS
DISCUSSION
Occult hepatitis B virus in Sudan had been
detected in different populations; it recorded 15.1% in HIV positive patients [11-15]
and among hemodialysis patients it was 0% in white Nile state and 3.3% in
Khartoum state [16,17], but much higher prevalence were observed in blood
donors, cancer patients, renal transplant patients and patients with
hematological disorders, recording 38%, 38.2%, 51.4% and 53.3% prevalence rates,
respectively [18-21] which is similar to our current finding (36.3%) when using
RT-PCR. In Africa similar studies were done regarding OBI revealed that a rate
of 7.4%, 8.7% and 7.3% in Libya, Nigeria and Burkina Faso, respectively [22-24].
The variation of OBI rates according to global studies may be affected by
populations of the study, demography and sensitivity of used assay [23,25].
The high prevalence of OBI recorded in the
present study indicates that HBV infection is endemic in Atbara town, northern
Sudan. In Africa more than 50% of the adult population may have serologic
evidence of past hepatitis B infection [7]. In this study, the prevalence rate
of HBsAg was 0% and HBcAb was 50%. Similar study in Tanzania found prevalence
rates of 4.3%, and 29.3% for HBsAg and HBcAb, respectively [11].
Among the 44 (50%) HBcAb positive samples in
our study, HBV-DNA was detected in 16 (36.3%) of them. All HBV DNA positive
samples were found to be negative for HBsAg; this is consistent with the
definition of occult hepatitis B (OBI). Possible explanations for occult HBV
are: (1) mutations in ‘α’ epitope of the S gene could alter the
antigenicity of HBsAg, causing the failure of anti-HBs to neutralize HBsAg; (2)
or due to decline in HBV genome replication and expression; (3) also altering
HBx and/or overlapping core promoter function can reduce HBV replication due to
mutation in HBx ORF region [12].
The frequency of OBI (18.2%) in febrile
patients without any signs or symptoms of clinical hepatitis in our study is
higher than that found (12.5%) in a previous study conducted in West Kurdofan State, Sudan [13]. This rate is
also much higher in comparison with previous data (3%) from immigrants
with fever from sub-Saharan African countries to Australia [14].
The variation in our results regarding HBV
DNA detection by using real time PCR (36.3%) and conventional PCR (2.3%) may be
due the fact that we used heat treatment plasma without DNA extraction [9]. This
may indicate that heat treatment method is more suitable to use with RT-PCR
than conventional PCR but this also may be due to the higher sensitivity of
RT-PCR.
CONCLUSION
It is concluded from our study that there is
a need for HBV testing in individuals presenting with febrile illnesses in
areas where HBV are endemic using serological and molecular methods. Finally
and to the best of our knowledge the present study represents the first report
on HBV infection in River Nile State.
ACKNOWLEDGMENT
The authors would like to thank Atbara
teaching hospital and health centers for allowing us to collect samples from
their patients.
1.
McMahon BJ, Alward WL, Hall DB,
Heyward WL, Bender TR, et al. (1985) Acute hepatitis B virus infection:
Relation of age to clinical expression of disease and subsequent development of
the carrier state. J Infect Dis 151: 599-603.
2.
Kolawole OM, Kana SN (2018)
Hepatitis B virus and malaria co-infection causing significant changes in
hematological and liver function indices in a cohort of subjects in Ilorin,
Nigeria. Int J Infect.
3.
Shepard CW, Simard EP, Finelli
L, Fiore AE, Bell BP (2006) Hepatitis B virus infection: Epidemiology and
vaccination. Epidemiol Rev 28: 112-125.
4.
McCarthy MC, Hyams KC, El-Hag
AE, El-Dabi MA, El-Tayeb ME (1989) HIV-1 and hepatitis B transmission in Sudan.
Naval Medical Research Inst Bethesda MD.
5.
Kramvis A, Kew MC (2007)
Epidemiology of hepatitis B virus in Africa, its genotypes and clinical
associations of genotypes. Hepatol Res 37: S9-S19.
6.
Abou MA, Eltahir YM, Ali AS
(2009) Seroprevalence of hepatitis B virus and hepatitis C virus among blood
donors in Nyala, South Dar Fur, Sudan. Virol J 6: 146.
7.
Hyams KC, Al-Arabi MA,
Al-Tagani AA, Messiter JF, Al-Gaali AA, et al. (1989) Epidemiology of hepatitis
B in the Gezira region of Sudan. Am J Trop Med Hyg 40: 200-206.
8.
Elsheikh RM, Daak AA, Elsheikh
MA, Karsany MS, Adam I (2007) Hepatitis B virus and hepatitis C virus in pregnant
Sudanese women. Virol J 4: 104.
9.
Nyan DC, Ulitzky LE, Cehan N,
Williamson P, Winkelman V, et al. (2014) Rapid detection of hepatitis B virus
in blood plasma by a specific and sensitive loop-mediated isothermal
amplification assay. Clin Infect Dis 59: 16e23.
10.
Garson JA, Grant PR, Ayliffe U,
Ferns RB, Tedder RS (2005) Real-time PCR quantitation of hepatitis B virus DNA
using automated sample preparation and murine cytomegalovirus internal control.
J Virol Methods 126: 207-213.
11.
Mudawi H, Hussein W, Mukhtar M,
Yousif M, Nemeri O, et al. (2014) Overt and occult hepatitis B virus infection
in adult Sudanese HIV patients. Int J Infect Dis 29: 65-70.
12.
Majed AA, El Hussein ARM, Ishag
AEH, Madni H, Enan KA, et al. (2018) Absence of occult hepatitis B virus
infection in hemodialysis patients in white Nile state, Sudan. Virol Immunol J
2.
13.
Abdalhafeez AM, Khalid AE,
Osama MK, Mohammed OH, Abdel RMEH, et al. (2015) Prevalence of occult hepatitis
B virus (HBV) infections in hemodialysis patients in Khartoum state, Sudan from
2012 to 2014. J Med Lab Diagn 6: 22-26.
14.
Abd El Kader Mahmoud O, Abd El
Rahim Ghazal A, El Sayed Metwally D, Elnour AM, Yousif GE (2013) Detection of
occult hepatitis B virus infection among blood donors in Sudan. J Egypt Public
Health Assoc 88: 14-18.
15.
Gasmelseed NEA, Elhaj EY, Saeed
OK, Elsir AA, Elbalal M (2014) Occult hepatitis B virus in Gezira state Sudan.
Sudan J Med Sci 9.
16.
El Sheredy AG, El Ghazzawy EF,
Helaly GF, El Naggar AA, Mahadi MM (2015) Occult hepatitis B virus infection in
patients with blood diseases. Int J Curr Microbiol Appl Sci 4: 1-10.
17.
Mustafa MO, Enan KA, Elkhidir
IM, El Hussein ARM (2019) Occult hepatitis B virus and hepatitis B genotypes
among renal transplant patients in Khartoum state, Sudan. J Emerg Dis Virol 5.
18.
Shambesh MK, Franka EA, Agila
AR, Ismail FF (2018) Frequency of hepatitis B core antibody and hepatitis B
virus DNA among apparently healthy male blood donors in Eastern Libya. Libyan J
Med Sci 2: 12.
19.
Akintule OA, Olusola BA, Odaibo
GN, Olaleye DO (2018) Occult HBV infection in Nigeria. Arch Basic Appl Med 6:
87-93.
20.
Diarra B, Yonli AT, Sorgho PA,
Compaore TR, Ouattara AK, et al. (2018) Occult hepatitis B virus infection and
associated genotypes among HBsAg-negative subjects in Burkina Faso. Mediterr J
Hematol Infect Dis 10.
21.
Meschi S, Schepisi MS, Nicastri
E, Bevilacqua N, Castilletti C, et al. (2010) The prevalence of antibodies to
human herpes virus 8 and hepatitis B virus in patients in two hospitals in
Tanzania. J Med Virol 82: 1569-1575.
22.
Brechot C, Thiers V, Kremsdorf
D, Nalpas B, Pol S, et al. (2001) Persistent hepatitis B virus infection in
subjects without hepatitis B surface antigen: Clinically significant or purely
‘occult’? Hepatology 34: 194-203.
23.
Ahmadu A, Ibrahim IT, Ahmad OY,
Mohammed AA, Ismail A, et al. (2016) Prevalence of occult hepatitis B virus
infection in febrile patients in west Kurdofan state, Sudan. EC Microbiol 4:
671-677.
24.
Gibney KB, Torresi J, Lemoh C,
Biggs BA (2008) Isolated core antibody hepatitis B in sub-Saharan African
immigrants. J Med Virol 80: 1565-1569.
25.
Saijo T, Joki N, Inishi Y, Muto
M, Saijo M, et al. (2015) Occult hepatitis B virus infection in hemodialysis
patients in Japan. Ther Apheresis Dialysis 19: 125-130.
-
 Table 1
Table 1
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Advance Research on Alzheimers and Parkinsons Disease
- Journal of Rheumatology Research (ISSN:2641-6999)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Chemotherapy Research Journal (ISSN:2642-0236)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)


