3008
Views & Citations2008
Likes & Shares
Background: Aspirin desensitization and daily aspirin therapy constitute an effective option in patients with aspirin-exacerbated respiratory disease (AERD) who has sub optimally controlled asthma or rhino sinusitis, or require multiple polypectomies.
Objective: Our objective was to evaluate the utility and safety of nasal/oral ketorolac/aspirin desensitization (NOKAD) in patients with AERD.
Methods: Fourteen patients with challenge-proved AERD underwent NOKAD and they were also treated with aspirin during at least the next 3 months. Three questionnaires and an olphatometric test were used to evaluate the clinical outcome to aspirin treatment.
Results: All AERD patients received a 300 mg aspirin per os after NOKAD. Eight patients (57.14%) did not present any reaction during the oral phase of the NOKAD. The remaining six patients (42.86%) developed lower respiratory tract symptoms, including easily treated mild bronchospasm and/or chest tightening when they took 25 mg (in 4 cases) and 50 mg doses (2 cases) of aspirin. All questionnaires scores showed a significant clinical improvement of asthma and Sino nasal symptoms within 30 days from the start of treatment.
Conclusion: NOKAD followed by aspirin therapy is a safe alternative treatment which improves patients very early, with special emphasis on the Sino nasal dimension of their symptoms.
Keywords:Aspirin-exacerbated respiratory disease, Aspirin desensitization, Aspirin therapy
Abbreviations: ACT: Asthma control test; AD:Aspirin desensitization; AERD:Aspirin-exacerbated respiratory disease; HrQOL:Health-related quality-of-life; miniRQLQ: Mini Rhino conjunctivitis Quality of Life Questionnaire; NKC:Nasal ketorolac challenge; NOKAD:Nasal/oral ketorolac/aspirin desensitization; SNOT-20: Sino Nasal Outcome Test
TO THE EDITOR
Aspirin desensitization (AD) is a safe and appropriate procedure for the management of some patients with aspirin-exacerbated respiratory disease (AERD). Long-term clinical outcomes of AD, followed by daily aspirin therapy, were mainly related with a lower number of additional sinus surgeries and have also been found to be helpful in improving airway disease (in upper and lower symptoms) and reducing outpatient and emergency department visits [1]. However, only a few studies have demonstrated a significative early impact (3 months or below) of this procedure in AERD patients on several markers of disease activity, such as nasal inspiratory peak flow and nasal nitric oxide [2] or non-standardized Likert-type nasal and asthma scores [3].
The aim of this study was to determine if the aspirin treatment could improve the severity and health-related quality-of-life (HrQOL) questionnaires evaluated in less than 3 months after AD.
The 14 adult subjects with AERD were identified performing a nasal ketorolac challenge (NKC) using an acoustic rhinomether as previously described [4]. Briefly, single-blind challenge was started with saline solutionspraying 2 puffs into each nostril.Then a graduated challenge with ketorolac solution was performed using an initial dose of 1 mg (1 puff). If no clinical response occurred and if Vol 2-8 declined less than 30 %, incremental doses of ketorolac were administered every 30 minutes, controlled with acoustic rhinometry and spirometrybefore each dose: 2 mg (1 spray for each nostrils), 4 mg (2 sprays for each nostrils) and finally 6 mg (3 sprays for each nostrils). Thus, the maximal cumulative doses in nasal challenge were 13 mg of ketorolac. If the patient showed any symptoms or signs during incremental ketorolac exposure, the challenge was interrupted and the reaction treated.A positive challenge was defined as an increase of 30% or greater of nasal symptoms recorded by a visual analog scale and a 30 % drop in the sum of both nasal cavities volume at the level of 2 to 8 cm. Single-blind placebo controlled oral challenges with 750 mg of aspirin (in cumulative doses) was carried out in those patients who showed a negative NKC. Drugs that could interfere with the results of NKC, such as H1 receptor antagonists and short acting bronchodilator agents, were stopped 1 week and 6 hours before the procedure, respectively. However, all other asthma treatment (including montelukast, long-acting bronchodilator agents and inhaled glucocorticoids) were not discontinued.
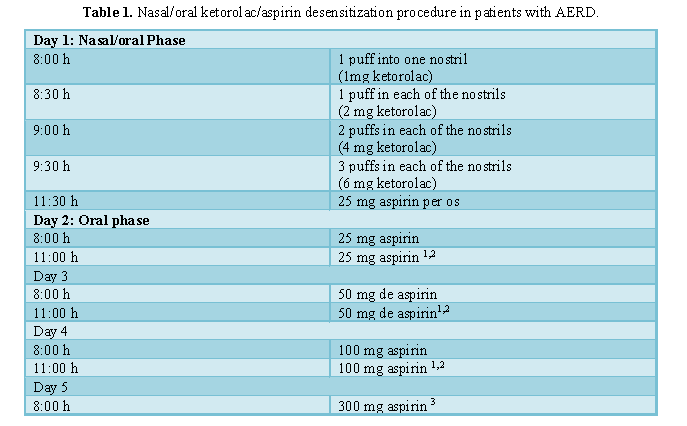
These patients underwent a nasal/oral desensitization procedure with ketorolac/aspirin (NOKAD) according to a modified method proposed by Lee [5] within 24 h after the diagnostic procedure was made (Table 1) and then they were also treated with aspirin during 3 months. Three HrQOL questionnaires: Mini Rhino conjunctivitis Quality of Life Questionnaire (miniRQLQ) [6], Sino Nasal Outcome Test (SNOT-20) [7] and asthma control test (ACT) [8] and the Connecticut olphatometric test [9] were used to evaluate the clinical outcome to aspirin treatment at 1 and 3 months.
· If any reaction was noted, the provoking ketorolac or aspirin doses were administered again when the reaction ceased.
· If no reaction, the next nasal or oral dose was administered.
· Patients were desensitized when they tolerated 300 mg aspirin without any reaction.
All AERD patients received a 300 mg aspirin per os after NOKAD. Eight patients (57.14%) did not present any reaction during the oral phase of the NOKAD. The remaining six patients (42.86%) developed lower respiratory tract symptoms, including mild bronchospam and/or chest tightening when they took 25 mg (in 4 cases) and 50 mg doses (2 cases) of aspirin, respectively.
Figure 1 summarizes the overall values of the different clinical questionnaires used in the study collected before the NOKAD, at 30 days and 90 days after treatment with aspirin. The medians of these three measurements were: 57 (43.25 - 59.75), 14.5 (6.5 - 44.25) and 8.5 (1.75 - 29.25), respectively. The differences between the baseline values and those at 30 days were significant (p = 0.016), while there were no significant differences between the values at 30 and 90 days.
The medians of these three measurements of mini RQLQ were: 40 (24 - 57), 7 (4 -30) and 4 (2 - 19), respectively. The ocular symptom dimension did not show significant changes when compared at baseline and after 90 days of treatment. The rhinosinusal symptoms dimension only showed a significant difference between the baseline and 90 days of treatment (p = 0.009).
The medians of these three ACT measurements were: 17 (10-21), 23 (20-25) and 24 (23-25), respectively. The differences between the baseline values and those at 30 days were significant (p = 0.012), while no differences were observed between the values at 30 and 90 days.
The medians of these three measurements of mini RQLQ were: 40 (24 - 57), 7 (4 -30) and 4 (2 - 19), respectively. The ocular symptom dimension did not show significant changes when compared at baseline and after 90 days of treatment. The rhinosinusal symptoms dimension only showed a significant difference between the baseline and 90 days of treatment (p = 0.009).
The medians of these three ACT measurements were: 17 (10-21), 23 (20-25) and 24 (23-25), respectively. The differences between the baseline values and those at 30 days were significant (p = 0.012), while no differences were observed between the values at 30 and 90 days.
No significant changes were detected between the baseline test and the measurements at 30 and 90 days in the overall smell score. The medians of these three measurements were: 1 (0-2.5), 1.5 (0-6) and 2 (0.5-7), respectively. However, 4 patients (28.5%) who previously had severe anosmia recovered completely their sense of smell during 300 mg aspirin therapy.
Twenty-five years and more than 1500 patients support the experience in oral desensitization with aspirin [1]. In 2010, a new procedure combining the nasal and oral route was designed to shorten desensitization, although with an unacceptable rate of severe, laryngeal and systemic reactions which were clustered in the oral phase [5]. This study aimed to modify this protocol to obtain greater clinical safety and this has been fully achieved.
All reactions observed were nasoocular or asthmatic reactions, mild and easily controllable with inhaled salbutamol.Previous experience in desensitization of patients with AERD has shown solid successful clinical evidence in the improvement of polyposis, asthma and rhino sinusitis; However, quantitative and quality of life studies have been scarce, and, in any case, they have focused on evaluating the long-term clinical results of desensitization [1]. The aim of this study was to generate quantifiable and short-term data about 1 month and 3 months after treatment with aspirin. Interestingly, most of the improvement in the different dimensions is obtained in the first month of treatment, although the statistical significance is even greater when comparing the baseline values and 90 days after treatment. Desensitization, therefore, is an alternative treatment, possibly due to the failure of conventional options, which improves patients very early, with special emphasis on the Sino nasal dimension of their symptoms.
1. Walters KM, Waldram JD, Woessner KM, White AA (2018) Long-term clinical outcomes of aspirin desensitization with continuous daily aspirin therapy in aspirin-exacerbated respiratory disease. Am J Rhinol Allergy 32: 280-286.
2. Cooper T, Greig SR, Zhang H, Seemann R, Wright ED, et al. (2019) Objective and subjective Sino nasal and pulmonary outcomes in aspirin desensitization therapy: A prospective cohort study. Auris Nasus Larynx 46: 526-532.
3. Berges-Gimeno MP, Simon RA & Stevenson DD (2003) Early effects of aspirin desensitization treatment in asthmatic patients with aspirin-exacerbated respiratory disease. Ann Allergy Asthma Immunol 90: 338-341.
4. Quiralte-Castillo J, Ávila-Castellano MR, Cimbollek S, Benaixa P, Leguisamo S, et al. (2017) Nasal ketorolac challenge using acoustic rhinometry in patients with aspirin-exacerbated respiratory disease. J InvestigAllergol Clin Immunol 27: 169-174.
5. Lee RU, White AA, Ding D, Dursun AB, Woessner KM, et al. (2010) Use of intranasal ketorolac and modified oral aspirin challenge for desensitization of aspirin-exacerbated respiratory disease. Ann Allergy Asthma Immunol 105: 130-135.
6. Calderón MA, Casale TB &Demoly P (2019) Validation of patient-reported outcomes for clinical trials in allergic rhinitis: A systematic review. J Allergy Clin Immunol Pract 7: 1450-1461.
7. Piccirillo JF, Merritt MG Jr, Richards ML (2002) Psychometric and clinimetric validity of the 20-Item Sino-Nasal Outcome Test (SNOT-20). Otolaryngol Head Neck Surg 126: 41-47.
8. Vega JM, Badia X, Badiola C, López-Viña A, Olaguíbel JM, et al. (2007) Validation of the Spanish version of the asthma control test (ACT). J Asthma 44: 867-872.
9. Toledano A, Ruiz C, Navas C, Herráiz C, González E, et al. (2009) Development of a short olfactory test based on the Connecticut Test (CCCRC). Rhinology 47: 465-469.
-
 Table 1
Table 1

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Diabetes (ISSN: 2644-3031)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- BioMed Research Journal (ISSN:2578-8892)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)


