1975
Views & Citations975
Likes & Shares
MATERIAL METHOD
This randomized, prospective study was started after receiving ethical approval. patients aged between 60-90 years, who were programmed for total hip replacement and femur fracture surgery under general anesthesia, had an ASA (American Society of Anesthesiologists) risk classification of I-III, were at least literate and offered written informed consent under the elective conditions. The patients were separated 2 groups with opaque sealed envelope technique (SNOSE) [Group 2 (rSO2 n=30), Group 1 (Control n=30). The same physician administered the Mini-Mental Test, functional Montreal Cognitive Assessment Scale (MoCA) to the patients before the anesthesia and the Mini-Mental Test and MOCA test were repeated at the postoperative 24th hour. All the patients were followed using standard anesthesia monitoring, radial artery invasive monitoring, BIS (Datex-Ohmeda S5, Finland) and cerebral oxygen saturation monitoring (INVOS 5100). For the patients in Group 1 (Control Group), the cerebral oximeter monitor was turned to the reverse direction from the sight of the investigator. Cerebral oximetry monitor was followed-up in Group 2 (Study Group), and NIRS (INVOS 5100) and rSO2 values were documented in the groups. The depth of anesthesia was checked using BIS Monitoring (BIS VISTA COVIDIEN REF 185-0151) that were maintained between 40 and 60. Vital parameters were recorded during the surgery. Induction was initiated after the patients were provided with 100% oxygen support for three minutes through a mask. Management of the anesthesia was completed by 1 mg/kg lidocaine (Armita 2%, Osel), 0.5-1 mcg/kg remifentanil (Ultiva 5 mg, GlaxoSmithKline) and 5 mg/kg thiopental (Pental Sodium, İ.E. Ulagay) and 0.6 mg/kg rocuronium. If there was an adequate muscle relaxation, the intubation was finished, and patients were ventilated using a Dräger (Lübeck, Germany) anesthesia device to save the tidal volume at 6-8 ml/ kg and frequency at 12/ min. To maintain anesthesia, we used 2% sevoflurane (Sevorane, Abbott Lab, UK) and an infusion of 0.25 μg/kg/min of remifentanil along with 40% O2 and 60% air. The doses of remifentanil infusion were continued in both groups to save the MAP above 65 mmHg. Heart rate was maintained at a maximum of 30% change from baseline. Hypotension is defined as a 30% decrease in MAP compared to basal blood pressure, a systolic blood pressure less than 90 mmHg, or a MAP less than 55 mmHg, and hypotension is defined as intravenous fluids or vasoconstrictor Corrected by administration of ephedrine. Arterial blood pressure values were measured and recorded preoperatively, at 60 minutes intraoperatively, and postoperatively. The algorithm described below was followed in the study group when rSPO2 dropped below 75% of the baseline value or stabilized for more than 15 sec below 50°C. The ventilator, anesthesia circuit and position of the patient’s head were checked.
- An attempt was complete to increase blood oxygenation by increasing Fİ O2.
- AttemptsweremadetomaintainETCO2atregularintervals. When ETCO2 dropped below 35, ventilation was reduced to increase the partial pressure of ETCO2.
- Ifmeanarterialpressurefellbelow20%ofbaseline,anattemptwasmadetoreturnarterialpressuretoWhenbrainrSO2levelswerepersistentlylow,intravenousfluidsandadministrationofavasoconstrictor(ephedrine)increasedmeanarterialpressureto20%abovebaseline.
- Erythrocyte transfusion was given when HTC dropped below 27%.
- In cases where the acceptable cerebral rSO2 values were not achieved despite all measures, 0.5 mg/kg propofol i.e. bolus was given to decrease brain metabolism. Ten minutes before the end of the procedure, anesthetic gas was stopped, and 100% oxygen was All patients received tramadol 1 mg/kg intravenously 30 minutes before completion of surgery. The duration of surgery, anesthesia and hospital stay was recorded. The patients were assessed using the Modified Aldrete’s Scoring System and transferred from the recovery room to inpatient wards when their Aldrete scores were 9 points.
Statistical Analysis
Study data were uploaded to a computer and evaluated using “SPSS (Statistical Package for Social Sciences) for Windows 22.0 (SPSS Inc, Chicago, IL).” Descriptive statistics were expressed as mean ± standard deviation, frequency distribution, and percentage. Categorical variables were assessed using Pearson's chi-square test. The suitability of the variables to a normal distribution was examined using visual methods (histograms and probability plots) and analytical methods (Kolmogorov-Smirnov test). For variables found not to follow a normal distribution, the Wilcoxon signed rank test was used as a statistical method to check statistical significance between two dependent groups. When a significant difference was detected between the independent groups, Bonferroni correction was applied to find the source of the difference. For variables following a normal distribution, a paired samples t-test between two dependent groups was used. Two-way Repeated Measures Analysis of Variance was used to always examine the changes of variables between groups. The statistical significance level was accepted as p <0.05.
RESULTS
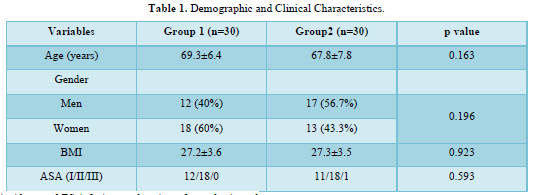
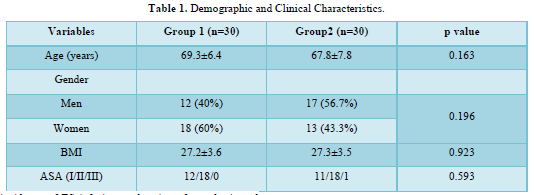
Of the 60 patients included in this study, 29 (48.3%) were male and 31 (51.6%) were female. The mean age, ASA risk score, gender distribution, and mean BMI are similar in the groups. (p>0.05) (Table 1).
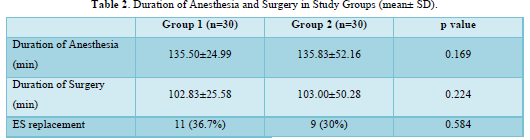
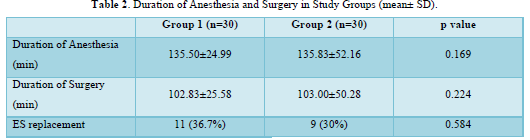
The incidence of ES infusion or duration of anesthesia and surgery was similar in both groups (p>0.05) (Table 2).
Compared to the first values, the SPO2 values significantly increased in both groups. In Group 2, the basal rSPO2 levels for both the right and the left hemispheres were found to be elevated at the 1st minute following intubation. No decrease was noted at later time points compared to the first values. Postoperatively, Hb, HTC, and albumin values were not similar between the two groups (p>0.05). A comparison of the mean arterial pressure levels between the study groups did not indicate any significant difference (p>0.05). ETCO2 values were similar in both groups (p>0.05). In both groups, BIS values were significantly lower at all time points compared to the first value.
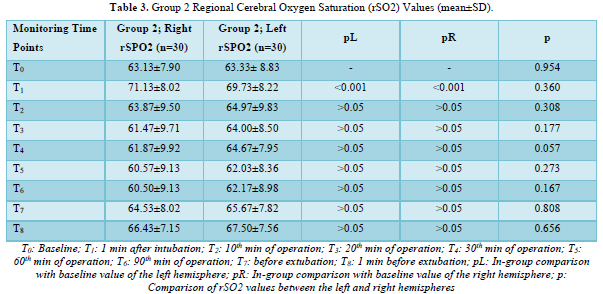
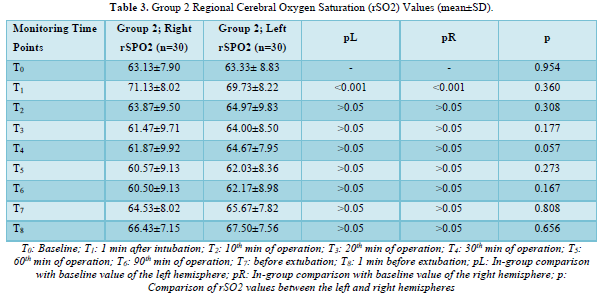
Baseline cerebral rSO2 values for both hemispheres were measured as 63.13±7.90 and 63.33± 8.83, respectively. There were no significant differences between the two hemispheres in baseline measurements or measurements recorded at subsequent time points (p>0.05). There was no correlation as for the patient’s age, ASA score and preoperative albumin levels with the cerebral rSO2 measurements of the left or right hemispheres.
Brain rSO2 values recorded 1 min after intubation were significantly higher compared to baseline values in both left and right hemispheres (p<0.001). For both hemispheres, there were no significant differences in rSPO2 compared to the baseline, except for the measurement obtained one minute after intubation (p>0.05) (Table 3).
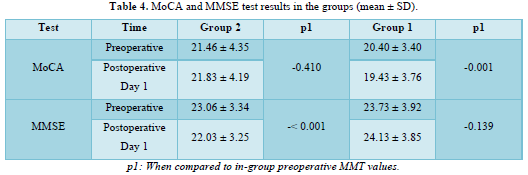
Preoperative MoCA scores were similar between the study groups (p>0.05) (Table 4). Postoperative 24 h MoCA values in group 1 were lower than preoperative values (p<0.001). 24th h MoCA scores in Group2 was significantly higher than the group1 scores (p<0.001) (Table 4). According to the MoCA scores in the control group POCD 63% and in monitored with NIRS group it was 40%.
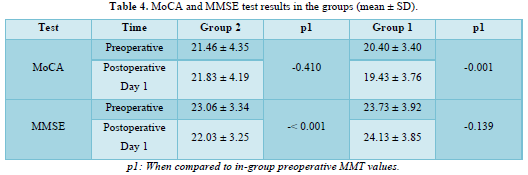
Preoperative MMSE scores did not change significantly between the two groups (p>0.05). In Group 1, the postoperative MMSE value was significantly lower than the preoperative MMSE (p<0.001). Preoperative and postoperative MMSE values were similar in Group 2 (p=0.139). In group 1 as a control group, POCD was determined 60% and in group 2 it was 30%.
DISCUSSION
NIRS monetarized patients’ preoperative and postoperative MMSE scores were not change after the surgery and MoCA scores in 5 patients were increased at postoperative 24th hour. On the other hand, the MMSE score of the control group was statistically significantly lower than the preoperative score. In group 1 POCD was seen %60-63, in group 2 %40-30. In this study, it was confirmed that cerebral oxygen saturation monitoring in geriatric patients had positive effects on neurocognitive test results in the early postoperative term. It must be emphasized that while there is agreement on which neuropsychological tests should be used to assess postoperative cognitive impairment, the validity and specificity of the tests already available are unknown [2]. In this study, we used MoCA and MMSE tests to detect early postoperative neurocognitive dysfunction. In a report by Gungen [9] a study conducted found that the threshold for analysis of mild dementia in Turkish elderly patients was 23/24. İn the literature there are studies that MoCA and MMSE used. A clinical trial that found the frequency of POCD was higher in sevoflurane group than propofol anesthesia. They observed the patients according to the MMSE and MoCA grades [11]. A study aimed to observe whether combined general and local anesthesia affects perioperative cognitive function compared to general anesthesia alone in elderly patients undergoing arthroplasty [12]. The combined anesthesia allowed the postoperative higher MMSE results. In another study showed that the dexmedetomidine has positive effect on the POCD and improved the MMSE score on the postoperative 24 h [13]. POCD is common neurologic problem occurring in geriatric patients [14]. In the literature that was showed that POD was not related with decreased survival. Endurance was a function of age, surgical duration, ASA score, and ICU length of stay [15]. In this study there weren’t any differences between groups in demographic data. We didn’t determine any correlation with cerebral rSO2 and demographic data. There are some strategies that improve the early recognition. The perioperative risk factors can be controlled to treat POCD [16]. When was the cerebral oxygenation added to the routine monitoring that could protect the patients from the POCD? [17]. The NIRS signal has correlation with measures of brain perfusion [18]. brain tissue oxygen tension [19] and CT perfusion [20], and in critical care this correlation was demonstrated [21]. NIRS provides continuous measurements of cerebral oxygen by measuring the relationship among the blood hemoglobin concentrations and neural activity [22]. In this study the correlation with hemoglobin and cerebral rSO2 was laid out. Yutaka Morimoto [23] showed that patient age and low preoperative brain rSO2 levels are risk factors for the development of postoperative delirium. Papadopoulos [5], the preoperative and postoperative cognitive dysfunction observed in geriatric patients with femur fracture were originated to be correlated with low cerebral oximetry values. The mean MMSE score of that patient population, which was 26.23±2.77 preoperatively, decreased to 25.94±2.52 after the operation and patients with an MMSE grade lower than 23 were considered to have cerebral dysfunction. In another study performed by Slater [24], cerebral desaturation during cardiac surgeries reduced postoperative cognitive functions and elongated the lengths of hospital stay [24]. However, NIRS management is limited in global brain ischemia damage and may omit micro-embolisms or hypoperfusion at sites distant to the frontal region. In their study, Reents [25] did not locate any connection between cerebral desaturation and neurological impairment [25]. The review included 1822 adult evaluating cerebral NIRS monitoring, no significant differences were defined between the groups for mortality postoperative stroke, postoperative delirium and cognitive dysfunction [26]. If there isn’t a chance to monitor the cerebral oxygenation, by the achieving hemodynamic stability may not be enough to reduction postoperative cognitive function impairments. The aim of keeping cerebral rSO2 level higher than 75% of baseline in patients who were followed via cerebral oxygen monitoring gave us the opportunity to perform interventions to increase cerebral oxygenation. In this study, a lower incidence of postoperative neurocognitive dysfunction was observed in the cerebral oximetry group, highlighting the importance of perioperative brain monitoring.
CONCLUSION
In conclusion, monitoring, and follow-up level of the cerebral oxygen, in geriatric patients who are taken into hip surgeries under general anesthesia are beneficial by reducing the potential for development of postoperative cognitive function impairments.
- Davis FM, Woolner DF, Framton C, Wilkinson A, Grant A, et al. (1987) Prospective, multi-center trial of mortality following general or spinal anesthesia for hip fracture surgery in the elderly. Br J Anaesth 59(9): 1080-1087.
- Monk TG, Weldon BC, Garvan CW, Dede DE, van der Aa MT, et al. (2008) Predictors of cognitive dysfunction after major noncardiac surgery. Anesthesiology 108(1): 18-30.
- Li YC, Xi CH, An YF, Dong WH, Zhou M (2012) Perioperative inflammatory response and protein S-100b concentrations-relationship with post-operative cognitive dysfunction in elderly patients. Acta Anaesthesiol Scand 56(5): 595-600.
- Rohan D, Buggy DJ, Crowley S, Ling FKH, Gallagher H, et al. (2005) Increased incidence of postoperative cognitive dysfunction 24 h after minor surgery in the elderly. Can J Anaesth 52(2): 137-142.
- Papadopoulos G, Karanikolas M, Liarmakopoulou A, Papathanakos G, Korre M, et al. (2012) Cerebral oximetry and cognitive dysfunction in elderly patients undergoing surgery for hip fractures: A prospective observational study. Open Orthop J 6: 400-405.
- Tobias JD, Johnson GA, Rehman S, Fisher R, Caron N (2008) Cerebral oxygenation monitoring using near infrared spectroscopy during one- lung ventilation in adults. J Minim Access Surg 4(4): 104-107.
- Edmonds Jr HL, Ganzel BL, Austin 3rd EH (2004) Cerebral oximetry for cardiac and vascular surgery. Semin Cardiothorac Vasc Anesth 8(2): 147-166.
- Arrowsmith JE, Harrison MJ, Newman SP, Stygall J, Timberlake N, et al. (1998) Neuroprotection of the brain during cardiopulmonary bypass: A randomized trial of remacemide during coronary artery bypass in 171 patients. Stroke 29(11): 2357-2362.
- Güngen C, Ertan T, Eker E, Yaşar R, Engin F (2002) Reliability and validity of the standardized Mini Mental State Examination in the diagnosis of mild dementia in Turkish population. Turk Psikiyatri Derg 13(4): 273-281.
- Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, et al. (2005) The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J Am Geriatr Soc 53(4): 695-699.
- Qiao Y, Feng H, Zhao T, Yan H, Zhang H, et al. (2015) Postoperative cognitive dysfunction after inhalational anesthesia in elderly patients undergoing major surgery: The influence of anesthetic technique, cerebral injury and systemic inflammation. BMC Anesthesiol 15: 154.
- Chen C, Li M, Wang K, Shen J, Yang L, et al. (2017) Protective effect of combined general and regional anesthesia on postoperative cognitive function in older arthroplasty patients. Int J Clin Exp Med 10: 15453-15458.
- Zhou C, Zhu Y, Liu Z, Ruan L (2016) Effect of dexmedetomidine on postoperative cognitive dysfunction in elderly patients after general anesthesia: A meta-analysis. J Int Med Res 44: 1182-1190.
- Tang N, Ou C, Liu Y, Zuo Y, Bai Y (2014) Effect of inhalational anesthetic on postoperative cognitive dysfunction following radical rectal resection in elderly patients with mild cognitive impairment. J Int Med Res 42: 1252-1261.
- Gottschalk A, Hubbs J, Vikani AR, Gottschalk LB, Sieber FE (2015) The impact of incident postoperative delirium on survival of elderly patients after surgery for hip fracture repair. Anesth Analg 121: 1336-1343.
- Kotekar N, Shenkar A, Nagaraj R (2018) Postoperative cognitive dysfunction - current preventive strategies. Clin Interv Aging 13: 2267-2273.
- Wood MD, Jacobson JA, Maslove DM, Muscedere JG, Boyd JG (2019) The physiological determinants of near-infrared spectroscopy-derived regional cerebral oxygenation in critically ill adults. Intensive Care Med Exp 7(1): 23.
- Kim MB, Ward DS, Cartwright CR, Kolano J, Chlebowski S, et al. (2000) Estimation of jugular venous O2 saturation from cerebral oximetry or arterial O2 saturation during isocapnic hypoxia. J Clin Monit Comput 16: 191-199.
- McLeod AD, Igielman F, Elwell C, Cope M, Smith M, et al. (2003) Measuring cerebral oxygenation during normobaric hyperoxia: A comparison of tissue microprobes, near-infrared spectroscopy, and jugular venous oximetry in head injury. Anesth Analg 97: 851-856.
- Taussky P, O’Neal B, Daugherty WP, Luke S, Thorpe D, et al. (2012) Validation of frontal near-infrared spectroscopy as noninvasive bedside monitoring for regional cerebral blood flow in brain-injured patients. Neurosurg Focus 32: E2.
- Wood MD, Song A, Maslove D, Ferri C, Howes D, et al. (2016) Brain tissue oxygenation in patients with septic shock: A feasibility study. Can J Neurol Sci 43(1): 65-73.
- Monk TG, Weldon JE (2002) Cerebral oxygen desaturations are associated with postoperative cognitive dysfunction in elderly patients. Anesthesiology 96: A40.
- Morimoto Y, Yoshimura M, Utada K, Setoyama K, Matsumoto M, et al. (2009) Prediction of postoperative delirium after abdominal surgery in the elderly. J Anesth 23(1): 51-56.
- Slater JP, Guarino T, Stack J, Vinod K, Bustami RT, et al. (2009) Cerebral oxygen desaturation predicts cognitive decline and longer hospital stay after cardiac surgery. Ann Thorac Surg 87(1): 36-44.
- Reents W, Muellges W, Franke D, Babin-Ebell J, Elert O (2002) Cerebral oxygen saturation assessed by near-infrared spectroscopy during coronary artery bypass grafting and early postoperative cognitive function. Ann Thorac Surg 74(1): 109-114.
- Yu Y, Zhang L, Zong H, Meng L, Han R (2018) NIRS for perioperative monitoring of brain oxygenation in children and adults. Cochrane Database Syst Rev 2018: CD01947.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Stem Cell Research and Therapeutics (ISSN:2474-4646)
- Journal of Spine Diseases
- Ophthalmology Clinics and Research (ISSN:2638-115X)
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- Journal of Renal Transplantation Science (ISSN:2640-0847)
- Oncology Clinics and Research (ISSN: 2643-055X)
- Dermatology Clinics and Research (ISSN:2380-5609)


