3025
Views & Citations2025
Likes & Shares
Background: Fusion and disc replacement surgeries are
common surgical procedures to treat discogenic low back pain affecting one or
two lumbar levels, however there remains millions of patients with significant
degenerative pathologies at 3 or more levels. Surgery to repair 3 or more
degenerated levels is typically unsuccessful and virtually always avoided by
surgeons and insurance companies alike
Purpose/Hypothesis: Many animal studies, and limited
human trials have demonstrated the safety and efficacy of mesenchymal stem cell
(MSC) based treatments for discogenic low back pain. Providing a biologic intervention
for patients with 3 or more degenerated discs rather than typical palliative
(pain control, physical therapy) measures could change the way discogenic back
pain is treated.
Study Design: Prospective, non-randomized, open label
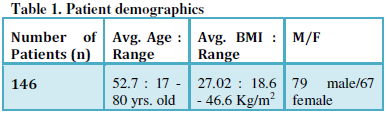
Methods: Patients included male and female
participants ranging in age from 17-80 years old (average 53), and BMI ranging
from 18.6 to 46.6 Kg/m2 (average 27). One hundred forty six patients
were studied based on having MRI documented disc degeneration at three or more
lumbar levels (modified Pfirmann grade of 5-7) and at least 6 months of
attempted conservative care. MSCs were harvested in the form of bone marrow
aspirate from the iliac crest to obtain bone marrow concentrate (BMC). The
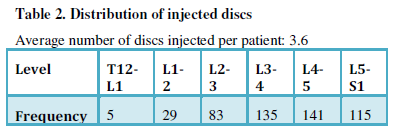
average patient had 3.6 levels treated. Outcomes were measured by Oswestry
Disability Index scores (ODI) and Visual Analog Scale pain scores (VAS)
pre-treatment, and at 3,6, and 12 months. Adverse events were monitored
throughout the study.
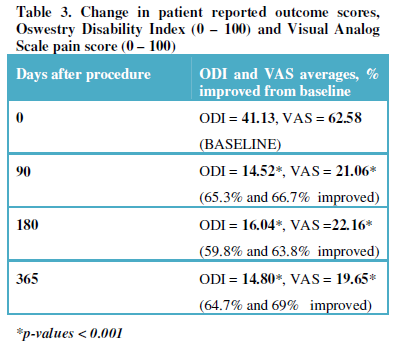
Results: There were no serious adverse events reported.
Patient average pre treatment scores (ODI / VAS) were 41.81 / 63.29, for 3
month patients 14.52/21.06, for 6 month patients 16.04/22.16 and 14.08/19.65 at
12 months. At 3 months the average patient improved by 65.3% / 66.7%
respectively, at 6 months by 59.8% /
63.8%, and at 12 months improved by 64.7% / 69% (all values p < 0.001).
There were no serious adverse events reported, and no patient had increased
pain or disability following the injections.. Two patients went on to have
surgery during the study, both for indications other than discogenic low back
pain (one had a foraminotomy, one a fusion for retrospondylolisthesis from a
new injury at a level adjacent to the treatment levels)
Conclusions: These results are superior to reported
results of one or two level surgical treatments (average improvement 35 to 40%)
and conservative measures (20 to 25%) for the same diagnosis. The BMC injection
patients had a higher percentage improvement and there were fewer complications
(revisions, infections etc.). Patient improvement was maintained from 3 months
through the twelve month follow up (from 3 to 12 months p = 0.76). Utilizing
MSCs derived from BMC, based on these preliminary results, may offer patients
with multi-level discogenic back pain a viable treatment option.
INTRODUCTION
Back pain is the second most common reason for physician visits in the United
States and the most common cause of missed work [1-3]. Costs for back pain
treatment in the U.S. are estimated to be at $100 billion annually [4].
Current non-operative treatments for chronic discogenic back pain
include activity modification, chiropractic care, exercise, physical therapy,
medications, and multiple steroid injections [2,5]. Surgical treatments for
severe chronic back pain are fusion or artificial disc replacement. The clinical results of one- or two-level
lumbar fusion for discogenic back pain are less than optimal compared to other
orthopedic procedures [6]. The consensus among spine surgeons is patients with
more than two segments of discogenic back pain have no surgical options and a poor
prognosis [6,7]. Millions of patients
have MRI scans which document abnormalities in three or more lumbar discs [2].
These patients are typically referred to chronic pain management clinics where
many end up on high-dose narcotic regimens and multiple steroid injections
[1-5,7,8]. Many of these patients are also unemployable [9]. The economic and
emotional impact of chronic low back pain on both society and the individual
patient is significant. Similar to other
chronic conditions, the treatment of multi-level discogenic back pain can cost
millions of dollars over a lifetime [2-4,7].
The lumbar disc is the largest avascular structure in your body. As a
result, cartilage cells in the nucleus and annulus of the intervertebral disc
have little capacity to heal annular tears or correct the degenerative process
of dehydration [10]. There is increasing literature to support the efficacy of
injecting discs with mesenchymal stem cells (MSCs) in an attempt to reverse or
slow down the degenerative process [11-20]. One previous study [21]
has demonstrated this procedure has the capacity to restore hydration to the
disc based on MRI evidence of modified Pfirrmann grade improvement in human
subjects. The purpose of this study is
to determine if MSCs in bone marrow concentrate (BMC) have safety and efficacy
to treat patients with three or more levels of discogenic low back pain.
MATERIALS
AND METHODS
This study is a prospective open-label
non-randomized evaluation of 146 patients having an injection of BMC into three
or more lumbar discs. Patients were enrolled as subjects in the study if they
presented with symptomatic moderate to severe discogenic low back pain as
defined by the following criteria:
centralized chronic low back pain increased by activity and lasting at
least six months; history of non-operative management for six months without
resolution; change in normal disc morphology as defined by MRI evaluation with
a modified Pfirrmann score of 5 to 7; modic grade-2 change or less; disc height
loss of less than 90% compared to an adjacent non-pathologic disc;
pre-treatment baseline oswestry disability index (ODI) of at least 30/100 and
pre-treatment baseline low back pain of at least 40mm/100mm visual analog scale
(VAS). An intact annulus was not required to be in the study. All patients underwent a pre-injection
medical history and physical including an ODI and VAS. These tests were repeated at three-, six-,
and 12-months post-injection of BMC. All
patients had a normal neurologic examination of the lower extremities,
demonstrated loss of lumbar range of motion, and had pain to deep palpation
over the symptomatic discs with associated muscle spasms. Standard exclusion
criteria included: an abnormal neurologic examination; symptomatic compressive
pathology due to stenosis or herniation; or any spondylolisthesis or
spondylolysis. Study patient
demographics are listed in Table 1.
The most common procedure based on discs injected were the 3 lower
lumbar discs ( L3 to S1), and the least likely disc to be injected were those
in the lower thoracic and at the thoracolumbar junction (T12-L1 and L1-2).
Bone marrow
collection and processing
Bone marrow aspirate (BMA, 55ml) was collected over Acid Citrate
Dextrose-anticoagulant (ACD-A, 5ml) from the patient’s posterior iliac
crest. The procedure was performed with
IV sedation consisting of Versed and Fentanyl.
Positioning of the Jamshidi needle in the iliac wing was confirmed by
fluoroscopy. BMA was collected in a 60ml
syringe in a series of discrete pulls on the plunger (targeting a collection of
5-10ml/pull), with repositioning of the needle tip between pulls based on the
reported enrichment of progenitor cells by Hernigou et al. [22] The
BMA was processed using the ART bone marrow concentration system (Selling
Biosciences, Austin, Texas) to produce a bone marrow concentrated cell
preparation. The 55 mL of BMA was centrifuged for 12 minutes to produce up to
10 mL of BMC>The BMC was drawn from the processing device, the glucose and
bicarbonate were added to the BMC. The BMC with the additives was immediately
transferred to the physician for injection [23]. Typically, a BMC volume was
drawn from the process device to allow 2ml to be injected into each degenerated
disc up to a maximum of 10ml of BMC.
Intradiscal
injection
With the patient in a prone position, the injection sites were treated
with local anesthetic (1% buffered Lidocaine).
BMC was percutaneously injected into the symptomatic discs through a
standard posterolateral discogram approach with a two-needle technique. An 18
gauge needle was placed against the posterior right corner of the annulus with
the position verified utilizing fluoroscopy. A 22 gauge needle was then placed
into the center of the nucleus. The injection point of the 22-gauge needle was
verified by fluoroscopy. Approximately
2-3ml of BMC were used per symptomatic lumbar disc injection. The entire procedure averaged less than 45
minutes. Patients were prescribed pain
medication to use as needed for three days and put on restricted physical
activity for two weeks.
Clinical Outcomes
Determination and Statistical Analysis: ODI and VAS scores were collected from
patients by non-investigator personnel employed by the clinic. Univariable data
comparisons were analyzed by two-tailed Student t-test with a 95% confidence
intervat (@=0.05, Microsoft Excel). Multivariable date were determined with
analysis of variance (ANOVA) using JMP 9 statistical analysis software (SAS
Institute, Cary, NC).
Results
There were no complications from harvesting of
the BMC or the disc injections. Not
every patient improved statistically, but no patient reported increases in VAS
or ODI from pre-treatment scores. There
were four patients eliminated from the data: one was in an ATV accident, one
developed a cyst in a non-treated vertebra unrelated to the injection, and two
patients decided to proceed with surgical treatment for indications other than
discogenic back pain.
All the patients who had their injections greater than 12 months prior
to the writing of this paper were called for final follow-up, and were also
asked about the amount of epidural steroid injections (ESIs) and daily narcotics/NSAIDS they were taking before and after the stem
cell injection. No patient who responded reported having any ESIs after having
his/her disc injected with BMC. The average patient had decreased
narcotic/NSAID intake by ~50% following the BMC injection, and no patient
reported increased consumption of narcotic/NSAID pain medication.
DISCUSSION
Millions of patients have multiple levels of abnormal discs based on
MRI scanning [1]. Almost all causes of multi-level discogenic low back pain
patients are of unknown etiology. These
patients develop progressive degeneration of multiple discs likely due to a
genetic component [9,10,24,25]. Desiccated discs on MRI scanning can be seen in
patients as young as 16 [10,21]. Most every surgeon would agree performing a
three-, four-, or five-level fusion for discogenic back pain is not a
reasonable surgical option. Phillips et
al. [6] published an excellent systematic review on the treatment of
chronic discogenic low back pain. After
establishing strict quality and level of evidence requirements for the review
trials, they reported on 26 studies. All
patients had one or two abnormal discs with results of the review showing a
weighted average of 35.3% improvement in the surgical group (547 patients) and
a 20% improvement in the non-surgical group (372 patients). Twelve prospective randomized studies were
reviewed comparing various fusion techniques with a minimum two-year
follow-up. These patients again were
restricted to one or two levels. The
results were 43.3% improvement in back pain (1,420 patients) with a
re-operation rate of 15.3%. These
results along with other meta-analysis of fusion surgeries versus non-operative
care demonstrate that even within the context of one or two degenerated discs,
fusion surgery provides less than optimal outcomes, and in an appreciable
amount of cases, actually makes things worse [26,27]. The minimal data
available on three or more level fusions in the context of degenerative disc
disease is inconsistent and typically shows poor outcomes. This is the prime
reason most surgeons will not attempt the procedure. The lack of clinical data
showing surgical efficacy makes insurance coverage for multi-level fusion for
discogenic back pain very difficult [9,24].
Mesenchymal stem cells (MSCs) have many positive attributes and have
mounting evidence of safety in human use [28-30]. BMC is a source of MSCs. MSCs are anti-inflammatory, secrete numerous
growth factors, stimulate blood vessel formation, modulate your immune system
to enhance healing, fight bacteria, and turn into cartilage cells to potentially
heal damaged discs in the lumbar area [11-20,28,31,32]. Circumventing
the circulation limitations of articular structures like the intervertebral
disc by local injection of BMC is hypothesized to expose these areas to the
body’s potential regenerative healing mechanisms where MSCs would normally be
occluded. MSC’s through paracrine cellular communication modulate the
regenerative environment via anti-inflammatory and immunomodulatory mechanisms.
In response to inflammatory molecules such as interlukin-1 (IL-1), IL-2, IL-12,
tumor necrosis factor-alpha, and interferon-gamma, MSC’s secrete an array of
growth factors and anti-inflammatory proteins to modulate many types of immune
cells. These paracrine mechanisms may explain some of the MSC’s efficacy in
treating disc pathology [28].
There is research published primarily in animals documenting the safety
and efficacy of MSCs to treat damaged discs and many other orthopedic
conditions. MSC based treatments have
become standard of practice in veterinary medicine [11-20,33-40]. We have
published our one-year and two-year minimum follow-up results from treating
patients with BMC having only one or two degenerated discs with symptomatic low
back pain. These studies show treating
patients with one or two levels of discogenic low back pain results in
improvement of VAS and ODI similar to the current study on treating patients
with three or more levels [21,41].
Limitations of this study include: no randomized control, no follow up
MRI scan data and no cell count data. The author has published MRI follow up
data and cell count data in a similar group of patients with the same
pathology. [21,41].
CONCLUSION
Patients with more than two levels of symptomatic discogenic low back
pain have limited treatment options.
There is minimal literature reporting the long-term efficacy of any
non-operative treatment (chronic narcotics and multiple steroid injections),
and these patients basically have no surgical options. One-year follow-up in treating multi-level
discogenic low back pain with BMC showed an average 65% improvement in ODI
(p-value<0.001) and 70% improvement in VAS (p-value<0.001) No patient was made worse from the procedure,
and there were no complications from the percutaneous injection of BMC into the
discs. Utilizing MSCs derived from bone
marrow concentrate, based on these preliminary results, may offer patients with
multi-level discogenic low-back pain a viable treatment option.
- Andersson
GB (1999) Epidemiological features of chronic low-back pain. Lancet 354:
581-585.
- Freburger
JK, Holmes GM, Agans RP, Jackman AM, Darter JD, et al. (2009) The rising
prevalence of chronic low back pain. Arch Intern Med 169: 251-258.
- Deyo
RA, Weinstein JN (2001) Low back pain. N Engl J Med 344: 363-370.
- Katz
JN (2006) Lumbar disc disorders and low-back pain: socioeconomic factors
and consequences. J Bone Joint Surg Am 88: 21-24.
- Dagenais
S, Caro J, Haldeman S (2008) A systematic review of low back pain cost of
illness studies in the United States and internationally. Spine J 8: 8-20.
- Phillips
FM, Slosar PJ, Youssef JA, et al. (2013) Lumbar spine fusion for chronic
low back pain due to degenerative disc disease. Spine 38: E409-22.
- van
Tulder MW, Koes BW, Bouter LM (1995) A cost-of-illness study of back pain
in The Netherlands. Pain 62: 233-240.
- White
AP, Arnold PM, Norvell DC, Ecker E, Fehlings MG (2011) Pharmacologic
management of chronic low back pain: synthesis of the evidence. Spine
(Phila Pa 1976) 36: S131-143.
- Chou
R, Carragee JB, Eugene J, Resnick DK, Shaffer WO, et al. (2009) Surgery
for Low Back Pain: A Review of the Evidence for an American Pain Society
Clinical Practice Guideline Spine (Phila PA 1976) 34: 1094-1109.
- Vergroesen
P, Kingma I, manuel KS, Hoogendoorn RJ, Welting TJ, et el. (2015)
Mechanics and biology in inintervertebral disc degeneration: A vicious
circle. Osteoarthritis and Cartilage.
- Sakai
D, Andersson GB (2015) Stem cell therapy for intervertebral disc
regeneration: obstacles and solutions. Nat Rev Rheumatol 11: 243-256.
- Yim
R, Lee J, Bow C, Meij B, Leung V, et al. (2014) A systematic review of the
safety and efficacy of mesenchymal stem cells for disc degeneration:
Insights and future directions for regenerative therapeutics. Stem Cells
Dev 23: 2553-2567.
- Acosta
F, Metz L, Adkisson H, Liu J, Liebenberg EC, et al. (2011) Porcine intervertebral
disc repair using allogeneic juvenile articular chondrocytes or
mesenchymal stem cells. Tissue Eng Part A 17: 3045-3055.
- Allon
AA, Aurouer N, Yoo BB, Liebenberg EC, Buser Z, et al. (2010) Structured
coculture of stem cells and disc cells prevent disc degeneration in a rat
model. Spine J 10: 1089-1097.
- Bendtsen
M, Bunger C, Zhou X, Foldager C, Jorgensen HS (2011) Autologous stem cell
therapy maintains vertebral blood flow and contrast diffusion through the
endplate in experimental intervertebral disc degeneration. Spine (Phila PA
1976) 36: E373-E379.
- Feng
G, Zhao X, Liu H, Zhang H, Chen X, et al. (2011)
Transplantation of mesenchymal stem cells and nucleus pulposus cells in a
degenerative disc model in rabbits: a comparison of 2 cell types as
potential candidates for disc regeneration. J Neurosurgery Spine 14:
322-329.
- Ghosh
P, Moore R, Vernon-Roberts B, Goldschlager T, Pascoe D, et al. (2012)
Immunoselected STRO-3+ mesenchymal precursor cells and restoration of the
extracellular matrix of degenerate intervertebral discs. J Neurosurgery
Spine 16: 479-488.
- Hee
HT, Ismail HD, Lim CT, Goh JC, Wong HK (2010) Effects of implantation of
bone marrow mesenchymal stem cells, disc distraction and combined therapy
on reversing degeneration of the intervertebral disc. J Bone Joint Surg Br
92: 726-736.
- Hiyama
A, Mochida J, Iwashina T, Omi H, Watanabe T, et al. (2008) Transplantation
of mesenchymal stem cells in a canine disc degeneration model. J Orthop
Res 26: 589-600.
- Sakai
D, Mochida J, Iwashina T, Watanabe T, Nakai T, et al. (2005)
Differentiation of mesenchymal stem cells transplanted to a rabbit
degenerative disc model: potential and limitations for stem cell therapy
in disc degeneration. Spine (Phila PA 1976) 30: 2379-2387.
- Pettine
K, Murphy M, Suzuki R, Sand T (2015) Percutaneous injection of autologous
bone marrow concentrate cells significantly reduces lumbar discogenic pain
through 12 months. Stem Cells 33: 146-156.
- Hernigou
P, Mathieu G, Poignard A, Manicom O, Beaujean F, et al. (2006) Percutaneous
autologous bone-marrow grafting for nonunions. Surgical technique. J Bone
Joint Surg Am 88: 322-327.
- Pettine
K (2013) Regenerative Autologous Bone Marrow Cell Therapies and Methods
for their use in the treatment of joint pain.
- Röllinghoff
M, Schlüter-Brust K, Groos D, Sobottke R, Michael JW, et al. (2010)
Mid-range outcomes in 64 consecutive cases of multilevel fusion for
degenerative diseases of the lumbar spine. Orthop Rev (Pavia) 2: e3.
- Vora
RN, Barron BA, Almudevar A, Utell MJ (2012) Work-related chronic low back
pain-return-to-work outcomes after referral to interventional pain and
spine clinics. Spine (Phila Pa 1976) 37: E1282-1289.
- Bydon
M, De la Garza-Ramos R, Macki M, Baker A, Gokaslan AK, et al. (2014)
Lumbar fusion vs. non-operative management for treatment of discogenic low
backk pain: a systematic review and meta-analysis of randomized controlled
trials. J Spinal Discord Tech.
- Saltychev
M, Eskola M, Laimi K (2014) Lumbar fusion compared with conservative
treatment in patients with chronic low back pain: a meta-analysis. Int J
Rehabil Res 37: 2-8.
- Murphy
MB, Moncivais K, Caplan AI (2013) Mesenchymal Stem Cells: environmentally
responsive therapeutics for regenerative medicine. Exp Mol Med.
- Lalu
MM, McIntyre L, Pugliese C, Fergusson D, Winston BW, et al. (2012) Safety
of cell therapy with mesenchymal stromal cells (SafeCell): a systematic
review and meta-analysis of clinical trials. PLoS One 7: e47559.
- Peeters
CM, Leijs MJ, Reijman M, van Osch GJ, Bos PK (2013) Safety of
intra-articular cell-therapy with culture-expanded stem cells in humans: a
systematic literature review. Osteoarthritis Cartilage 21: 1465-1473.
- Counsel
PD, Bates D, Boyd R, Connell DA (2015) Cell therapy in joint disorders.
Sports Health 7: 27-37.
- Kristjánsson
B, Honsawek S (2014) Current perspectives in mesenchymal stem cell
therapies for osteoarthritis. Stem Cells Int 2014: 194318.
- Black
LL, Gaynor J, Adams C, Dhupa S, Sams AE, et al. (2008)
Effect of intraarticular injection of autologous adipose-derived
mesenchymal stem and regenerative cells on clinical signs of chronic
osteoarthritis of the elbow joint in dogs. Vet Ther 9: 192-200.
- Chang
CH, Kuo TF, Lin FH, Wang JH, Hsu YM, et al. (2011) Tissue
engineering-based cartilage repair with mesenchymal stem cells in a porcine
model. J Orthop Res 29: 1874-1880.
- Guercio
A, Di Marco P, Casella S, Cannella V, Russotto L, et al. (2012) Production
of canine mesenchymal stem cells from adipose tissue and their application
in dogs with chronic osteoarthritis of the humeroradial joints. Cell Biol
Int 36: 189-194.
- Lee
KB, Hui JH, Song IC, Ardany L, Lee EH (2007) Injectable mesenchymal stem
cell therapy for large cartilage defects--a porcine model. Stem Cells 25:
2964-2971.
- Sato
M, Uchida K, Nakajima H, Miyazaki T, Guerrero AR, et al. (2012) Direct
transplantation of mesenchymal stem cells into the knee joints of Hartley
strain guinea pigs with spontaneous osteoarthritis. Arthritis Res Ther 14:
R31.
- Murphy
JM, Fink DJ, Hunziker EB, Barry FP (2003) Stem cell therapy in a caprine
model of osteoarthritis. Arthritis Rheum 48: 3464-3474.
- Mokbel
A, El-Tookhy O, Shamaa AA, Sabry D, Rashed L, et al. (2011) Homing and
efficacy of intra-articular injection of autologous mesenchymal stem cells
in experimental chondral defects in dogs. Clin Exp Rheumatol 29: 275-84.
- Mokbel
AN, El Tookhy OS, Shamaa AA, Rashed LA, Sabry D, et al. (2011) Homing and
reparative effect of intra-articular injection of autologous mesenchymal
stem cells in osteoarthritis animal model.BMC Musculoskelet Disord 12:
259.
- Pettine
K, Suzuki R, Sand T, Murphy M (2016) Treatment of discogenic back pain
with autologous bone marrow concentrate injection with minimum two year
follow-up. Int Orthop 40: 135-140.
-
 Table 1
Table 1 -
Table 2
-
Table 3

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- Journal of Renal Transplantation Science (ISSN:2640-0847)
- Journal of Cardiology and Diagnostics Research (ISSN:2639-4634)
- Ophthalmology Clinics and Research (ISSN:2638-115X)
- Journal of Alcoholism Clinical Research
- Oncology Clinics and Research (ISSN: 2643-055X)


