
30
Views & Citations10
Likes & Shares
Results: The actual movement obtained (0.639 mm) was consistently smaller than that planned (1.632 mm) across all brands. Angel Aligner® showed the lowest mean gross difference (0.842 mm) and the lowest standard deviation (0.656), whereas Spark® presented the highest relative predictability (58.42%). The lower arch reached a higher relative predictability (percentage of achieved movement), although with larger gross differences. A critical threshold was identified at around 2 mm, with smaller movements being more predictable.
Conclusions: Digitally planned intrusion shows significant discrepancies with the clinical outcome. Angel Aligner® offers greater overall consistency, Spark® greater movement potential with higher variability, and movements below 2 mm prove to be the most predictable across all brands.
Keywords: Clear aligners; Intrusion; Overbite; Predictability; Digital set-up; STL superimposition.
Historically, the concept of repositioning the teeth by means of sequential appliances dates back to Kesling’s positioners (1945) and to their subsequent refinement by Nahoum, who developed a vacuum-formed appliance [6]. The aligner era is officially considered to have begun in 1998, when the FDA approved the marketing of Align Technology’s Invisalign®, the first system manufactured using digital CAD/CAM technology [7,8].
In parallel, Angel Aligner® became established in China where it patented its technology in 2006 and launched the iOrtho platform in 2013 [9], while Ormco® introduced the Spark® system in 2017, expanding rapidly across different markets [10].
The plastic material is decisive in the behavior of the aligner: it must be flexible enough to allow its insertion and removal, yet rigid enough to apply continuous and controlled forces [2]. To achieve predictable movements, thermoplastics must combine elastic and plastic properties, the basis for force generation [5,11]. Among the materials described are PET, PET-G and polyurethane (PU) [12,13], and clinical performance also depends on thickness (between 0.5 and 1 mm) and on the manufacturing process, whether vacuum thermoforming over physical models or direct 3D printing [14]. Thermoforming itself can alter the molecular structure of the polymer and modify the applied force system [12].
Each manufacturer uses its own material solutions. Invisalign® evolved from the first polymers (PC30, EX30) to the current SmartTrack (LD30), a 0.75 mm multilayer thermoplastic polyurethane/copolyester that improves elasticity, activation and control over the tooth surface [15]. Angel Aligner® uses a dual system (MasterControl and MasterControl S) based on modified PET-G and TPU, with multilayer aligners that better distribute the load on the periodontal ligament and alveolar bone [4,6,9]. Spark®, for its part, introduced the TruGEN XR material free of BPA, mercury, latex and phthalates, intended for finishing and refinement [10].
The trimming line which defines how far the aligner extends over tooth and gingiva influences movement control, comfort, stability and esthetics [9,16]. Invisalign® usually employs a scalloped edge that follows the gingival contour; Angel Aligner® allows its height to be varied with three combinations (scalloped, straight at 2.5 mm or mixed) [9]; and Spark® opts for a straight edge that slightly covers the gingiva to improve retention [10]. These variations affect the stability of the aligner and its efficacy in specific movements such as intrusion [17,18].
Biomechanics is the core of treatment: only an adequate expression of force triggers the biological response of the periodontium and an efficient movement [19]. The behavior of the aligner depends on the direction and magnitude of the movement, the properties of the material, the thickness, the fit, the trimming design and the activation, and discrepancies persist between the planned virtual result and the clinical one [5,11,20]. The aligner generates the movement through millions of contact points between the plastic and the crown, according to a position programmed at each stage [11]. Within this framework, intrusion is one of the most demanding movements, highly dependent on the rigidity of the material and on auxiliary attachments [3]; relative intrusion (through proclination of the crown, more predictable) is distinguished from absolute intrusion (pure, along the long axis of the tooth) [5].
Each system approaches intrusion differently. With G5 and G8, Invisalign® incorporated pressure areas, optimized attachments and bite ramps that adjust the force according to the vertical position of each tooth, as well as sequences such as the “frog pattern” and conventional rectangular attachments to secure anchorage [21,22,23]. Spark® does not establish predefined protocols, leaving the biomechanical approach to the clinician’s judgment, and there is no specific literature on the matter. Angel Aligner® uses conventional and precision attachments, pressure areas and bite raisers, calculated by means of its masterforce artificial intelligence system [9].
Despite the broad clinical acceptance of aligners, doubts persist about their biomechanical predictability in complex movements such as incisor intrusion in increased overbites, and comparative studies that simultaneously evaluate different brands under a homogeneous methodology are scarce. Therefore, the general aim of this work was to determine the predictability of the amount of intrusion movement of the upper and lower incisors in patients with overbite, comparing the set-up planning with the results obtained through the superimposition of STL models in Nemotec® software, as well as to analyze the differences between arches and the relationship between the planned magnitude and the accuracy achieved.
MATERIAL AND METHOD
Study Design
A retrospective, observational and longitudinal study was carried out to evaluate the predictability of the intrusion movement of the upper and lower incisors (leveling of the curve of Spee) in 54 patients treated with aligners, distributed into three groups of 18 (Invisalign®, Spark® and Angel Aligner®). In each case, the initial STL model was superimposed on that of the first refinement, and the amount of planned intrusion movement was compared with the amount produced clinically.
Sample Selection
The search for patients was carried out in the database of the Invisalign Doctor Site platform of the Master’s Degree in Digital Advanced Orthodontics of the Universidad Europea de Madrid (coordinating center) and in the corresponding platforms of patients treated at the private practice of Dr. Romina Vignolo Lobato, in Majadahonda (Madrid). After selecting the patients on the platforms of each system (Invisalign®, Spark® and Angel Aligner®), the progress notes of the clinical records were exhaustively reviewed to confirm compliance with the criteria; patients who did not meet them were excluded.
Inclusion Criteria
- Patients treated with Invisalign® (Align Technology), Spark® and Angel Aligner® clear aligner therapy.
- Patients in permanent dentition.
- Patients treated in both arches.
- Patients with an intraoral scan at the start of treatment and at refinement that includes the palate with good definition of the palatal rugae.
- No restriction regarding Angle classification.
- Patient with a pre-treatment overbite of at least 4 mm.
- Completion of the first series of aligners without mid-treatment correction.
- Good compliance with constant aligner wear.
Exclusion Criteria
- Failure to complete the initial series of aligners.
- Poor compliance with aligner wear.
- Patient with primary or mixed dentition.
- Previous and active periodontal disease.
- Use of temporary anchorage devices.
Working Methodology
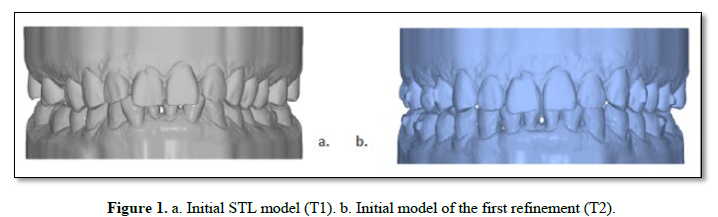
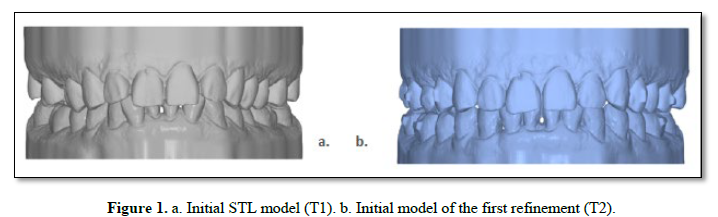
The study material was obtained from stereolithography (STL) files acquired with the iTero® and 3Shape® intraoral scanners. The superimposed models were labeled as T1 (initial STL of the first phase of the ClinCheck®/Spark Approver™/iOrtho™) and T2 (initial STL of the refinement phase) (Figure 1). Before starting the study, the overbite was evaluated on the T1 models to confirm the inclusion criterion of ≥4 mm [21].
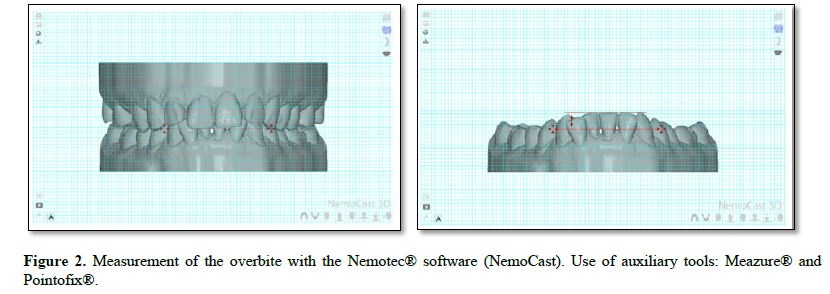
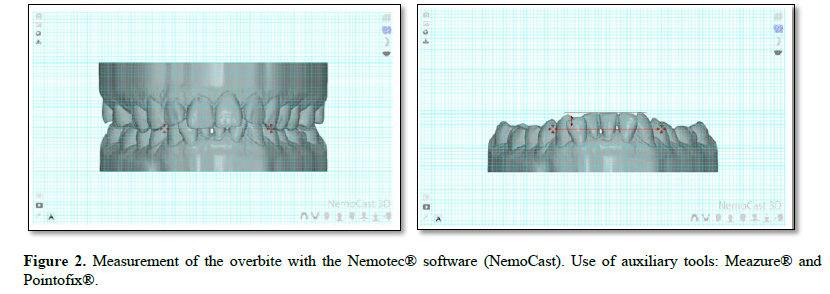
The models were imported into the NemoCast® tool from NEMOTEC S.L. and placed in the frontal plane. The overbite was measured between two antagonist teeth (central or lateral incisors) with the greatest vertical overlap, according to the American Board of Orthodontics classification system, by marking the incisal edge of the maxillary incisor and measuring in millimeters on the grid. As support for the software, the Meazure® and Pointofix® tools were used, which allow linear tracings and measurements on a tenth-of-a-millimeter scale outside the study models (Figure 2) [21].
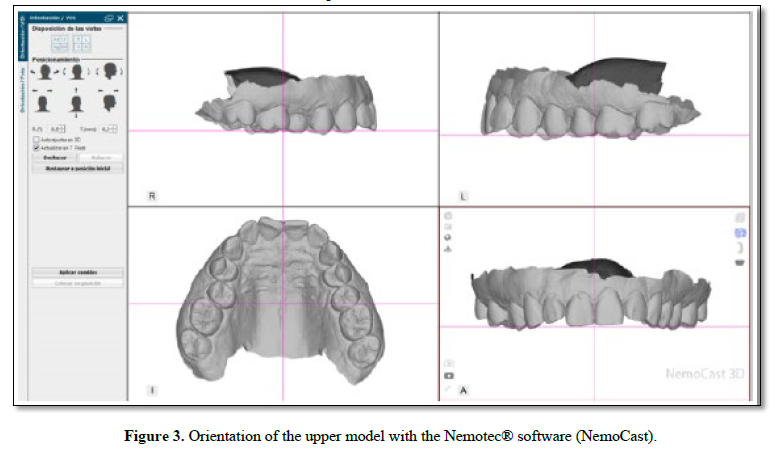
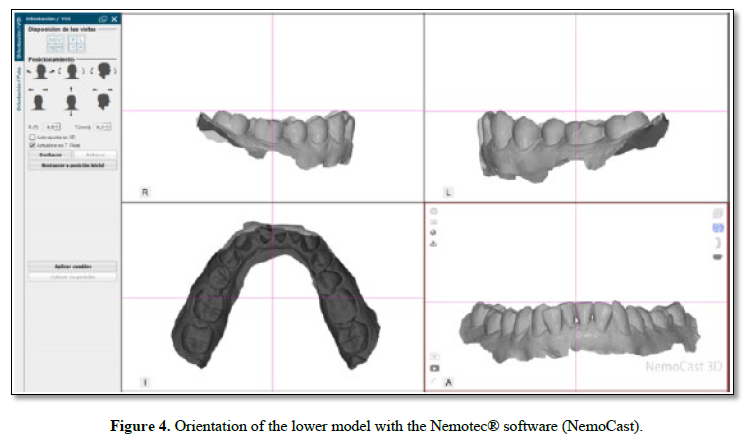
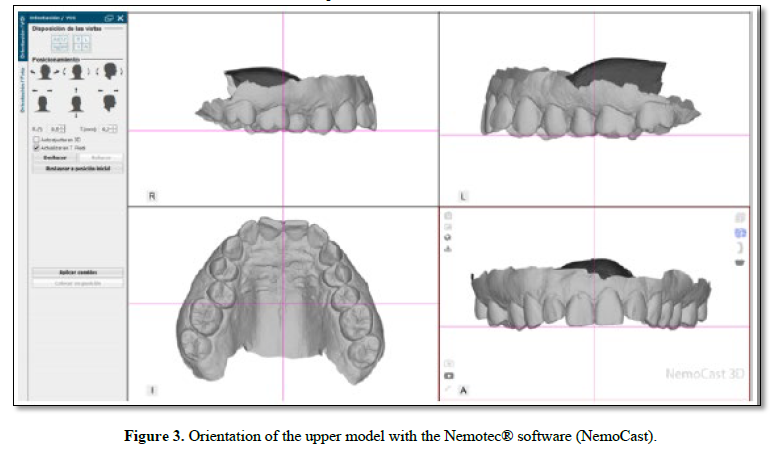
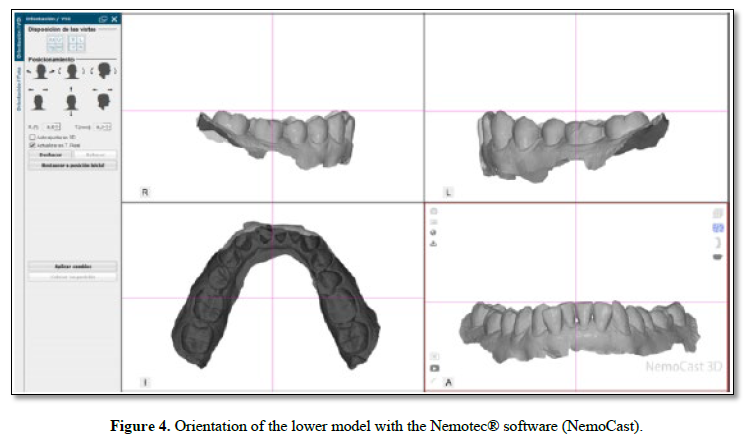
 To analyze the individual movements, the models were imported into the NEMOSTUDIO® software and each model was oriented in the three planes of space. In the upper jaw, the occlusal plane was defined as a straight line passing through the midpoint of the right and left incisal edges and the cusp tips of the bilateral first molars (Figure 3) [24,25]. In the lower model, the occlusal plane was established according to Braun’s technique, by means of a straight line joining the midpoint between the incisal edges of the mandibular central incisors and the distobuccal cusp of the second molar on each side (Figure 4) [26].
To analyze the individual movements, the models were imported into the NEMOSTUDIO® software and each model was oriented in the three planes of space. In the upper jaw, the occlusal plane was defined as a straight line passing through the midpoint of the right and left incisal edges and the cusp tips of the bilateral first molars (Figure 3) [24,25]. In the lower model, the occlusal plane was established according to Braun’s technique, by means of a straight line joining the midpoint between the incisal edges of the mandibular central incisors and the distobuccal cusp of the second molar on each side (Figure 4) [26].
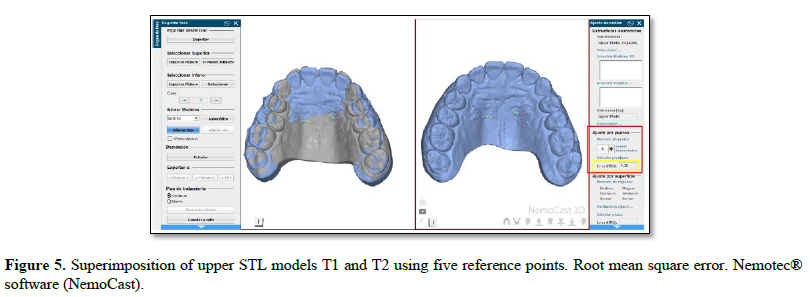
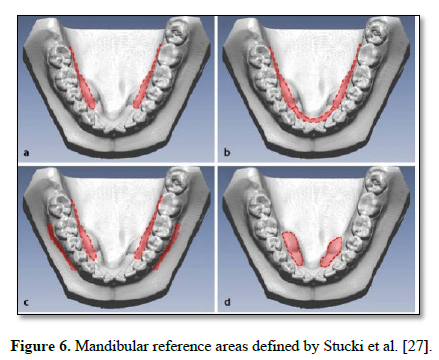
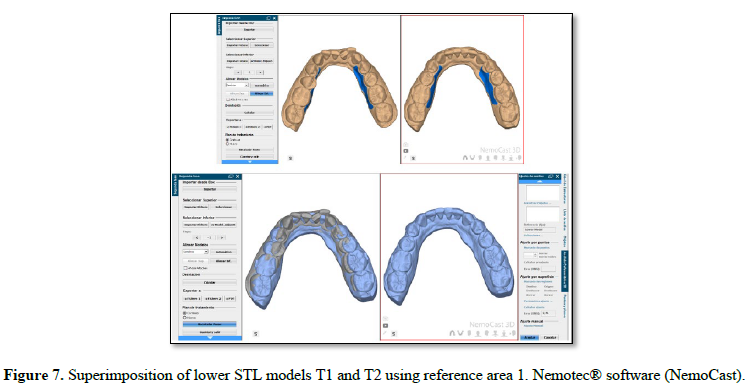
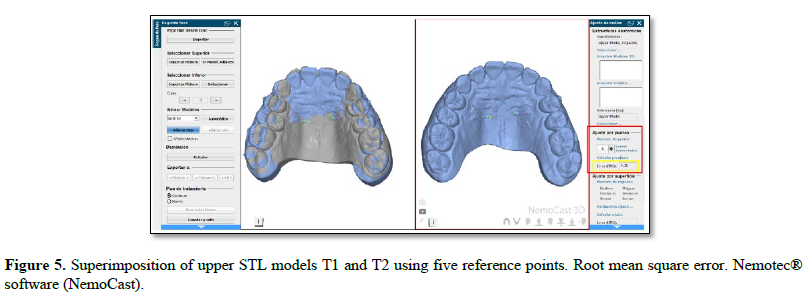
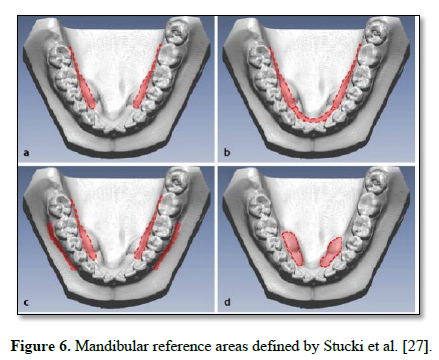
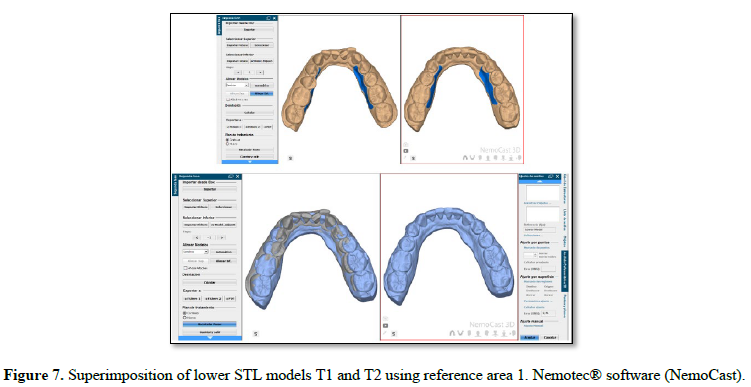
 Once oriented, the initial set-up model (T1, reference) was superimposed on the final achieved model (T2, from the first refinement set-up). In the upper jaw, the reference zone was the palatal rugae, defining at least five points in the medial two thirds of the third ruga of both hemiarches (Figure 5). In the mandible, the best-fit method was used over the four reference areas described by Stucki et al., choosing the one whose root mean square (RMS) error was closest to 0.3 mm or, ideally, lower (Figures 6 and 7) [27].
Once oriented, the initial set-up model (T1, reference) was superimposed on the final achieved model (T2, from the first refinement set-up). In the upper jaw, the reference zone was the palatal rugae, defining at least five points in the medial two thirds of the third ruga of both hemiarches (Figure 5). In the mandible, the best-fit method was used over the four reference areas described by Stucki et al., choosing the one whose root mean square (RMS) error was closest to 0.3 mm or, ideally, lower (Figures 6 and 7) [27].
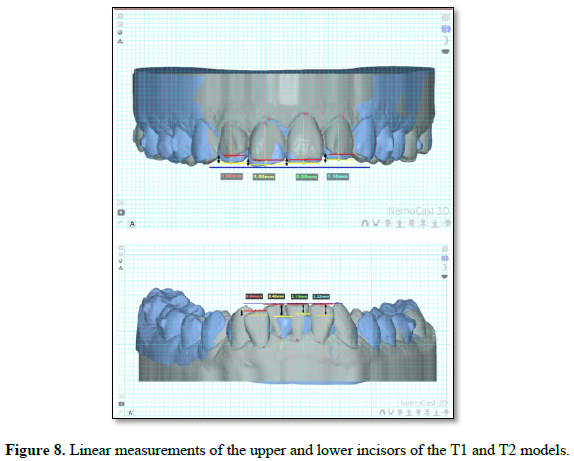
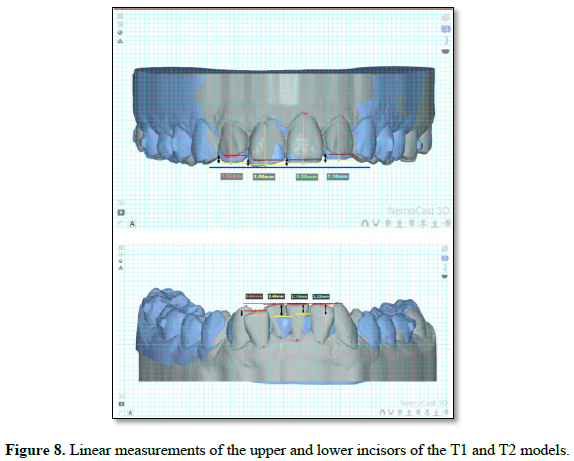
 The amount of intrusion was quantified with the program’s millimeter grid in frontal view: a horizontal line (from mesial to distal) was drawn on the incisal edges of each incisor as a fixed reference point, and the distance between the parallel lines passing through the midpoints of the incisal margin of T1 and T2 corresponded to the intrusion of each tooth (Figure 8) [2,21]. Finally, predictability was analyzed by comparing the digital planning set-up with the measurements of the T1 and T2 models; predictability was calculated as the actual movement obtained × 100 divided by the movement proposed in the set-up table (ClinCheck®/Spark Approver™/iOrtho™), obtaining the mean difference between what was planned and what was actually achieved. The statistical analysis was performed with JASP software (2023) - JASP (version 0.17.1), applying a two-way ANOVA, Tukey post-hoc contrasts and the intraclass correlation coefficient; a value of p < 0.05 was considered significant.
The amount of intrusion was quantified with the program’s millimeter grid in frontal view: a horizontal line (from mesial to distal) was drawn on the incisal edges of each incisor as a fixed reference point, and the distance between the parallel lines passing through the midpoints of the incisal margin of T1 and T2 corresponded to the intrusion of each tooth (Figure 8) [2,21]. Finally, predictability was analyzed by comparing the digital planning set-up with the measurements of the T1 and T2 models; predictability was calculated as the actual movement obtained × 100 divided by the movement proposed in the set-up table (ClinCheck®/Spark Approver™/iOrtho™), obtaining the mean difference between what was planned and what was actually achieved. The statistical analysis was performed with JASP software (2023) - JASP (version 0.17.1), applying a two-way ANOVA, Tukey post-hoc contrasts and the intraclass correlation coefficient; a value of p < 0.05 was considered significant.
RESULTS
Descriptive Statistics
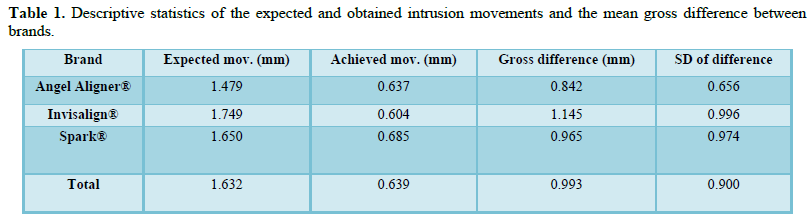
The final sample comprised 54 patients (18 per system) and the 8 incisors of each patient (12, 11, 21 and 22 in the upper arch; 32, 31, 41 and 42 in the lower arch), for a total of 432 incisors. The teeth whose planned movement was not intrusion (but extrusion) were removed from the analysis, leaving 364 teeth. The mean expected movement for the whole sample (1.632 mm) was consistently greater than the actual movement obtained (0.639 mm), evidencing a clear discrepancy between the software prediction and the clinical result, a trend common to the three brands (Table 1).
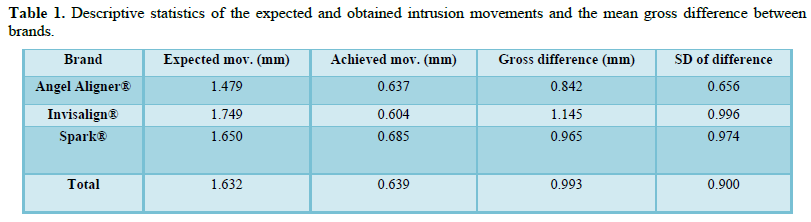
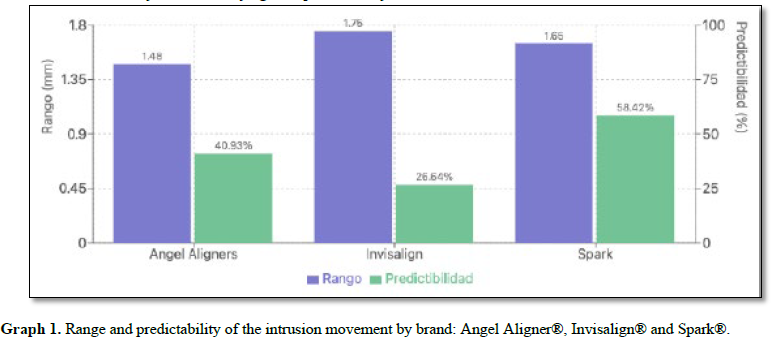
Angel Aligner® stood out for the lowest mean gross difference (0.842 mm) and the lowest standard deviation (0.656), suggesting greater consistency. Invisalign®, by contrast, presented the highest mean gross difference (1.145 mm) and the highest standard deviation (0.996), indicating considerable variability. When studying the predictability ratio (obtained / expected movement × 100), Spark® was the brand with the highest relative predictability (58.42%), although with a very high standard deviation, followed by Angel Aligner® (40.93%) and Invisalign® (26.64%) (Graph 1).
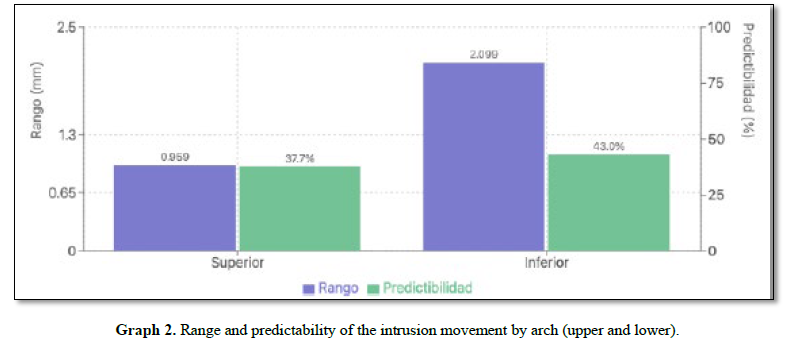
 The analysis by arch showed a consistent pattern of greater discrepancies in the lower arch across all brands, due to larger planned magnitudes, but with a higher percentage predictability. Spark® exhibited the most marked contrast: the lowest mean gross difference of all the groups in the upper arch (0.155 mm) versus a notable increase in the lower arch (1.392 mm). In terms of ratio, the lower arch reached a higher relative predictability (43.0%) than the upper arch (37.7%), although it should be borne in mind that a higher predictability percentage does not imply lower variability (Graph 2). For treatments of the upper arch, Spark® could be preferable, whereas Angel Aligner® would be the safest option when high predictability is required in both arches.
The analysis by arch showed a consistent pattern of greater discrepancies in the lower arch across all brands, due to larger planned magnitudes, but with a higher percentage predictability. Spark® exhibited the most marked contrast: the lowest mean gross difference of all the groups in the upper arch (0.155 mm) versus a notable increase in the lower arch (1.392 mm). In terms of ratio, the lower arch reached a higher relative predictability (43.0%) than the upper arch (37.7%), although it should be borne in mind that a higher predictability percentage does not imply lower variability (Graph 2). For treatments of the upper arch, Spark® could be preferable, whereas Angel Aligner® would be the safest option when high predictability is required in both arches.
When analyzing the planned movement range, the gross difference increased progressively with magnitude in the three brands. In movements smaller than 2 mm, Spark® presented the lowest mean difference (0.482 mm); in the 2-4 mm range the discrepancies grew markedly (up to 1.893 mm in Spark®), and in the few cases above 4 mm the largest differences were observed. This increase suggests a direct relationship between the planned magnitude and the loss of accuracy.
Inferential Statistics
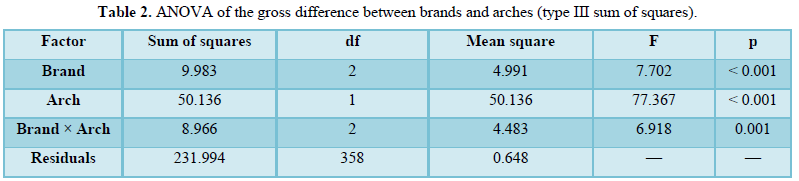
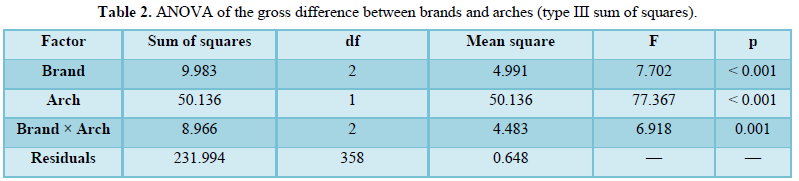
An analysis of variance (ANOVA) was applied to examine the differences in means by brand and by expected movement range. The two-way ANOVA identified statistically significant effects for both the aligner brand (F = 7.702; p < 0.001) and the arch (F = 77.367; p < 0.001), as well as a significant interaction between the two (F = 6.918; p = 0.001), which led to rejecting the null hypothesis and confirming significant differences in predictability between brands and arches (Table 2).
Levene’s test indicated heteroscedasticity (F = 9.498; p < 0.001), which advises some caution, although the ANOVA is robust to this violation given the large sample sizes; the Q-Q plot showed a satisfactory fit to the normality of the residuals, especially in the central region. The Tukey post-hoc analysis revealed significant differences between Angel Aligner® and Invisalign® (p = 0.003) and between Invisalign® and Spark® (p = 0.002) Invisalign® being the brand with the greatest differences, with no differences between Angel Aligner® and Spark® (p = 0.985).
Regarding the expected movement range, the ANOVA showed a significant effect on the obtained movement (F(2,361) = 29.230; p < 0.001). The Tukey contrast identified a highly significant difference between the group of movements smaller than 2 mm and the 2-4 mm group (mean difference −0.504
mm; p < 0.001), with no significant differences between the remaining groups. These results indicate a turning point around 2 mm, beyond which increases in the planned movement do not translate into proportional increases in the actual movement.
Finally, to assess reliability, the intraclass correlation coefficient was calculated one month after the initial measurements, remeasuring 10% of the randomly selected patients. The ICC3,1 coefficient (Shrout & Fleiss, 1979) was 0.989 (95% CI: 0.979-0.994), indicating an almost perfect concordance between the initial and repeated measurements and lending robustness to the results.
DISCUSSION
The most relevant finding of this study was the consistent difference between the digitally planned intrusion movement (1.632 mm) and the one obtained clinically (0.639 mm) in the three systems. This discrepancy is in agreement with what was described by Shahabuddin et al., who observed corrections of approximately 49% of the planned value, and by Castroflorio et al., with predictabilities of upper incisor intrusion with Invisalign® between 41.8% and 50.3% [21,25]; along the same lines, Kravitz et al. reported a mean intrusion accuracy of 41.3% [28]. From a biomechanical standpoint, the initial intrusion force decays after 24-48 hours [3] and the forces generated by PET-G for incisor intrusion are less efficient than for other movements [20], to which the loss of material rigidity after intraoral use is added
[15,18].
The differences between brands Angel Aligner® with the greatest consistency and Spark® with the highest relative predictability may be attributed to the composition and thickness of the materials and to the specific design of each system [6,12,14,35]. Previous studies indicate that the biomechanical response pattern of each system in the initial phase tends to be maintained throughout the refinements, so these findings have predictive value for anticipating behavior in subsequent phases [36,37]. The identification of a critical threshold at 2 mm is consistent with the inverse relationship between planned magnitude and predictability described by several authors and supports the planning of incremental movements through successive refinements [2,23,24,38].
Regarding the arches, the higher percentage predictability of the lower arch, despite its larger gross differences, could be explained by anatomical factors and by a more favorable force distribution, although with greater variability of the results [3,5,26,33]. As for the methodology, superimposition on the palatal rugae is considered highly reproducible as it is not affected by treatment [31,32], and intraobserver reliability was very high [33]. Limitations worth noting are the retrospective nature, the small sample size in movements greater than 4 mm considered exaggerated deep bite according to Nanda and the scarcity of previous studies on Spark® and Angel Aligner® [28,29,30,34]. Likewise, the analysis treated each incisor as an independent unit when the eight incisors come from the same patient and share common factors (compliance, supporting bone and planning); this clustering violates the independence assumption of the ANOVA, so in future work a linear mixed model with the patient as a random factor would be preferable. Finally, auxiliary elements such as bite ramps and skeletal anchorage with miniscrews could improve the predictability of intrusion, although the available evidence is still heterogeneous [22,37,39,40].
CONCLUSIONS
- There is a consistent discrepancy between the digitally planned intrusion movements and the clinical results obtained, generally smaller than expected in the three brands; the digital set-up, although valuable, does not guarantee absolute predictability.
- Angel Aligner® offers the most consistent results (lowest mean gross difference and lowest standard deviation), Spark® presents the highest relative predictability but with notable variability, and Invisalign® shows the greatest overall variability.
- A critical threshold is identified at around 2 mm: smaller movements are significantly more predictable, regardless of the brand, and increases above that threshold do not translate into proportional increases in the actual movement.
- The two-way ANOVA confirms significant differences between brands and between arches, as well as a significant interaction; the Tukey post-hoc analysis reveals particularly notable differences between Angel Aligner® and Invisalign®, as well as between Invisalign® and Spark®. The large sample size supports the robustness of the findings despite the detected heteroscedasticity.
- From a clinical perspective, the choice of system can be optimized according to the the specific objectives of the treatment: Angel Aligner® when predictability and consistency are the priority, Spark® when the aim is to maximize movement (especially in the upper arch), and the three brands with comparable performance in the lower arch.
DECLARATIONS
Ethics approval and consent: This retrospective study was carried out through the analysis of STL files previously obtained during routine clinical practice. No additional intervention was performed on the patients, nor were the care procedures modified for research purposes. Before their use in the study, all records underwent an anonymization process that ensured the removal of any identifying data and the protection of patient confidentiality. The analysis was conducted exclusively on pre-existing digital information, without access to personal data or the possibility of individual identification. Given the retrospective nature of the study and the exclusive use of anonymized data, obtaining individual informed consent was not necessary. The research was conducted in accordance with the ethical principles set out in the Declaration of Helsinki and its subsequent revisions, respecting at all times the privacy, confidentiality and protection of patient data.
FUNDING
The authors declare that they received no specific funding for this work.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest. The study received no support or sponsorship from Align Technology, Ormco (Spark) or Angel Aligner, the manufacturers of the systems evaluated.
AUTHOR CONTRIBUTIONS
AHL: methodological development of the study, literature search, data collection and analysis, interpretation of the results and writing of the original draft. RVL: study conception, access to the clinical records, supervision and critical revision of the manuscript. Both authors approved the final version of the article.
- Schupp W, Haubrich J. Aligner orthodontics and orofacial orthopedics. Quintessence Publishing; 2023. 648 p.
- Yan X, Zhang X, Ren L, Yang Y, Wang Q, Gao Y, et al. Effectiveness of clear aligners in achieving proclination and intrusion of incisors among Class II division 2 patients: a multivariate analysis. Prog Orthod. 2023;24(1).
- Liu Y, Hu W. Force changes associated with different intrusion strategies for deep-bite correction by clear aligners. Angle Orthod. 2018;88(6):771-8.
- Tartaglia GM, Mapelli A, Maspero C, Santaniello T, Serafin M, Farronato M, et al. Direct 3D printing of clear orthodontic aligners: current state and future possibilities. Materials. MDPI AG; 2021;14.
- Rivero Lesmes JC, Yeste Ojeda F, Nogal Coloma A, et al. Biomecánica en ortodoncia transparente. Revista Española de Ortodoncia. [complete year;volume(issue):pages].
- Bichu YM, Alwafi A, Liu X, Andrews J, Ludwig B, Bichu AY, et al. Advances in orthodontic clear aligner materials. Bioact Mater. 2023;22:384-403.
- Wajekar N, Pathak S, Mani S. Rise & review of Invisalign clear aligner system. IP Indian J Orthod Dentofacial Res. 2022;8(1):7-11.
- Weir T. Clear aligners in orthodontic treatment. Aust Dent J. 2017;62:58-62.
- Zamora G, Lobato V, Reátegui P, Alonso F, Rivera C. Innovaciones en el tratamiento con alineadores transparentes. 2023.
- Spark Clear Aligner system: the latest in clear aligner technology. 2023.
- Elshazly TM, Bourauel C, Ismail A, Ghoraba O, Aldesoki M, Salvatori D, et al. Effect of material composition and thickness of orthodontic aligners on the transmission and distribution of forces: an in vitro study. Clin Oral Investig. 2024;28(5).
- Kaur H, Khurelbaatar T, Mah J, Heo G, Major PW, Romanyk DL. Investigating the role of aligner material and tooth position on orthodontic aligner biomechanics. J Biomed Mater Res B Appl Biomater. 2023;111(1):194-202.
- Tamburrino F, D'Antò V, Bucci R, Alessandri-Bonetti G, Barone S, Razionale AV. Mechanical properties of thermoplastic polymers for aligner manufacturing: in vitro study. Dent J (Basel). 2020;8(2).
- Gold BP, Siva S, Duraisamy S, Idaayath A, Kannan R. Properties of orthodontic clear aligner materials - a review. J Evol Med Dent Sci. 2021;10(37):3288-94.
- Condò R, Pazzini L, Cerroni L, Pasquantonio G, Laganà G, Pecora A, et al. Mechanical properties of “two generations” of teeth aligners: change analysis during oral permanence. Dent Mater J. 2018;37(5):835-42.
- Elshazly TM, Salvatori D, Elattar H, Bourauel C, Keilig L. Effect of trimming line design and edge extension of orthodontic aligners on force transmission: a 3D finite element study. J Mech Behav Biomed Mater. 2023;140.
- Hertan E, McCray J, Bankhead B, Kim KB. Force profile assessment of direct-printed aligners versus thermoformed aligners and the effects of non-engaged surface patterns. Prog Orthod. 2022;23(1).
- Šimunović L, Jurela A, Sudarević K, Bačić I, Meštrović S. Differential stability of one-layer and three-layer orthodontic aligner blends under thermocycling: implications for clinical durability. Acta Stomatol Croat. 2023;57(4):286-99.
- Lyu X, Cao X, Yan J, Zeng R, Tan J. Biomechanical effects of clear aligners with different thicknesses and gingival-margin morphology for appliance design optimization. Am J Orthod Dentofacial Orthop. 2023;164(2):239-52.
- Gao L, Wichelhaus A. Forces and moments delivered by the PET-G aligner to a maxillary central incisor for palatal tipping and intrusion. Angle Orthod. 2017;87(4):534-41.
- Shahabuddin N, Kang J, Jeon HH. Predictability of the deep overbite correction using clear aligners. Am J Orthod Dentofacial Orthop. 2023;163(6):793-801.
- Moshiri M, Kravitz ND, Nicozisis J, Miller S. Invisalign eighth-generation features for deep-bite correction and posterior arch expansion. Semin Orthod. 2021;27(3):175-8.
- Pasciuti E, Coloccia G, Inchingolo AD, Patano A, Ceci S, Bordea IR, et al. Deep bite treatment with aligners: a new protocol. Appl Sci. 2022;12(13).
- Khosravi R, Cohanim B, Hujoel P, Daher S, Neal M, Liu W, et al. Management of overbite with the Invisalign appliance. Am J Orthod Dentofacial Orthop. 2017;151(4):691-699.e2.
- Castroflorio T, Sedran A, Parrini S, Garino F, Reverdito M, Capuozzo R, et al. Predictability of orthodontic tooth movement with aligners: effect of treatment design. Prog Orthod. 2023;24(1).
- Goh S, Dreyer C, Weir T. The predictability of the mandibular curve of Spee leveling with the Invisalign appliance. Am J Orthod Dentofacial Orthop. 2022;162(2):193-200.
- Stucki S, Gkantidis N. Assessment of techniques used for superimposition of maxillary and mandibular 3D surface models to evaluate tooth movement: a systematic review. Eur J Orthod. Oxford University Press; 2020;42:559-70.
- Kravitz ND, Kusnoto B, BeGole E, Obrez A, Agran B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop. 2009;135(1):27-35.
- Takeda LF, Risemberg RICS, Di Francesco ERS, Jorge FGC, Rodriguez MLA, Maltarollo TFH, et al. Tratamiento de mordida profunda. Research, Society and Development. 2022;11(4):e48111427249.
- Gonçalves A, Collard A, Monteiro F, Matos D, Carvalho Ó, Azevedo R, et al. Accuracy of Invisalign® on upper incisors: a systematic review. Turk J Orthod. Galenos Publishing House; 2023;36.
- Chen G, Chen S, Zhang XY, Jiang RP, Liu Y, Shi FH, et al. Stable region for maxillary dental cast superimposition in adults, studied with the aid of stable miniscrews. Orthod Craniofac Res. 2011;14(2):70-9.
- Lanteri V, Cossellu G, Farronato M, Ugolini A, Leonardi R, Rusconi F, et al. Assessment of the stability of the palatal rugae in a 3D-3D superimposition technique following slow maxillary expansion (SME). Sci Rep. 2020;10(1).
- Charalampakis O, Iliadi A, Ueno H, Oliver DR, Kim KB. Accuracy of clear aligners: a retrospective study of patients who needed refinement. Am J Orthod Dentofacial Orthop. 2018;154(1):47-54.
- Gonzalez Zamora D, Vignolo Lobato R. Proposal of a new attachment design for the optimization of tip movement with clear aligners. J Oral Med Dent Res. 2025;6(1).
- Elshazly TM, Keilig L, Nang D, Golkhani B, Weber A, Elattar H, et al. Effect of thermomechanical aging on force system of orthodontic aligners made of different thermoformed materials: an in vitro study. J Orofac Orthop. 2024.
- Houle JP, Piedade L, Todescan R, Pinheiro FHSL. The predictability of transverse changes with Invisalign. Angle Orthod. 2017;87(1):19-24.
- Greco M, Rombolà A. Precision bite ramps and aligners: an elective choice for deep bite treatment. J Orthod. 2022;49(2):213-20.
- Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL. Efficacy of clear aligners in controlling orthodontic tooth movement: a systematic review. Angle Orthod. Allen Press Inc.; 2015;85:881-9.
- Rodríguez-Vilaboa C, et al. Efectos de las rampas de mordida en alineadores. Revista de la Sociedad Española de Ortodoncia y Ortopedia Dentofacial. 2024;62(4):17-25.
- Henick D, Dayan W, Dunford R, Warunek S, Al-Jewair T. Effects of Invisalign (G5) with virtual bite ramps for skeletal deep overbite malocclusion correction in adults. Angle Orthod. 2021;91(2):164-70.
-
 Table 1
Table 1 -
Table 2
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Pathology and Toxicology Research



