1820
Views & Citations820
Likes & Shares
This is a case study on cysta colli mediana. It is encircled on account of insufficiency in the focal point of the ductus thyreoglossus, while the proximal and distal parts of the ductus are destroyed. The removed injuries from inside are verified with epithelium, which is tube formed and with fine cell contradicts, while the fistulа has a splitted epithelium. From Inside the cystа colli mediana is stacked up with mucous fluid. When in doubt, in the dividers of the cist and besides in the dividers of the fistules, the disturbance of a substitute degree was all the time perceived. It is routinely arranged in the inside line, typically close to the os hyoideum. The cysta colli mediana is all the time pea measure, yet can moreover accomplish the range of a nut. It is all around constrained and has a smooth surface. In this study, a brief report of 5 year old male child is described.
INTRODUCTION
The cysta colli mediana is formed due to insufficiency in the middle part of the ductus thyreoglossus, while the proximal and distal parts of the ductus are obliterated. The extracted cysts from the inside are covered with epithelium, which is cylindrical and with fine cell resists, while the fistulа has a splitted epithelium. From Inside the cystа colli mediana is filled with mucous fluid. Usually, in the walls of the cist and also in the walls of the fistules, the inflammation of a different degree was very often detected. It is very often located in the middle line, usually close to the os hyoideum. The cysta colli mediana is very often pea size, but can also reach the size of a nut. It is well restrained and has a smooth surface. Ofen is bent to the os hyoideum, but rarely can be bent to the skin, especially when was infection in the skin. Along with this localization, the cysta colli mediana can be detected in intraoral position close to the foramen caecum [1].
Differential diagnosis
(1) Lymphadenitis submentalis is easily recognizable by the detection of the primary infection from the teeth, lips or chin. The enlarged lymph gland is often located in the front part of the in the submental region, while the rest of the ductus thyreoglossus, is often located backwards.
(2) Cystic branchiogenes (branhiogenic cyst) are located a little bite laterally and usually at the anterior edge of the sternocleidomastoideus [2].
(3) Lymphadenitis tuberculosa is located in the upper mediastinum and can penetrate through the skin over the sternum manubrium and under the thyroid gland isthmus. Therefore, radiographic examination of the lungs is mandatory.
(4) The Cystis dermoides and the Atheroma in the middle line are intimately fattened with the skin, while the cystic colli of the median is is related to deeper structures used of the skin.
(5) Lipoma on the neck, especially in the middle line and anterior part of the neck is very rare. Although it exists, it is clearly limited and lobulated and does not fluctuate. Also, the fistula colli mediana can be not recognised and by mistake diagnosed as a fissure colli mediana. The fissure colli mediana occurs due to irregular merging of the lateral mesenchymal, branhiogenic masses. It seems like vertical neck knitting wound with a red base, easily recessed, with a length from about 1cm to a few centimeters, and a width up to 5 mm. In the upper and lower part of this crest, openings can be seen, which stretched in depth.
Treatment of the medial cysts and fistulas
Some authors are supporters of the conservative treatment especially in cases of small cysts. If we take into account its frequent infection, it is best to get rid of operative treatment. If the cysta is infected, it needs to be subject to a process of incision and drainage, and after few weeks cysta have to be completely removed. Sclerotherapy with a variety of solutions does not yield satisfactory results. Operative treatment is not so simple, because special surgical technique was required. Surgical treatment can be done with endotracheal anesthesia.
After elliptical excision with a thick cut, the resection of the middle part of the os hyoideum is obligatory, because then the surgeon approaches to the base of the tongue. The surgeons have to be careful not to remove the ectopic tissue of the glandе thyroide. Recognition can be done by detection of ball mass upon the os hyoideum with a diameter from 1 to 2 cm and evidence that there is no glande thyroide in the normal place.
CASE REPORT
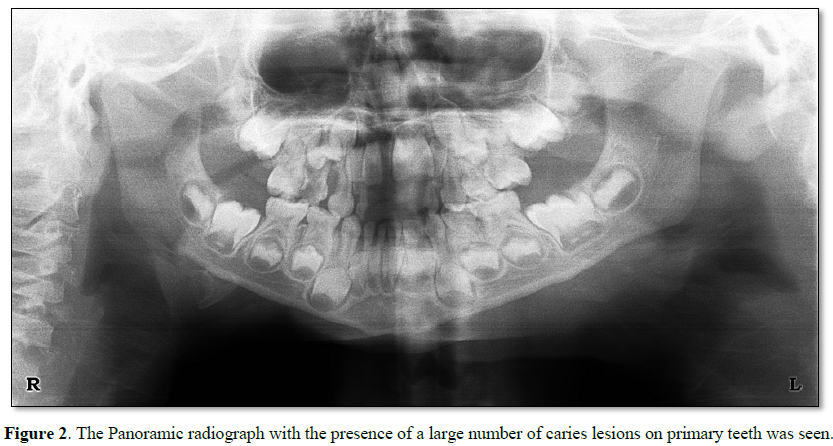
At the Department for Dental and Preventive Dentistry, a 5 year old male child (Figure 1) was referred by pediatric doctor for oral examination whether some carious teeth can be dental focus. The presence of a many carious teeth was largely confirmed on the orthopantomography (Figure 2). From an anamnesis that I took from the child's mother that the cyst was infected several time in the last six months. Also we received the information that the amoxicillin was prescribed by family doctor. During the first dental visit, extraction was carried out of the left primary incisor and the process of dental restoration started on all decay primary teeth. In the worst situation was the first right primary molar, with progressive caries lesion involving the pulp and periodontal space around the apex.
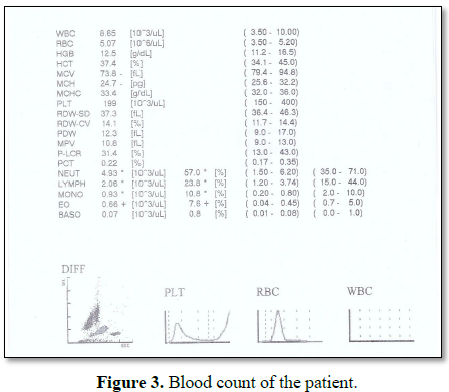
The child with his parents is redirected to the hematologic ambulance at the clinic hospital for children and the blood has been taken. The blood analysis was done at the biochemical hematologic laboratory at the University Clinic Hospital for Children and shows that all values were at normal limits, with the exception of insignificant higher values of monocytes and eosinophils (Figure 3).
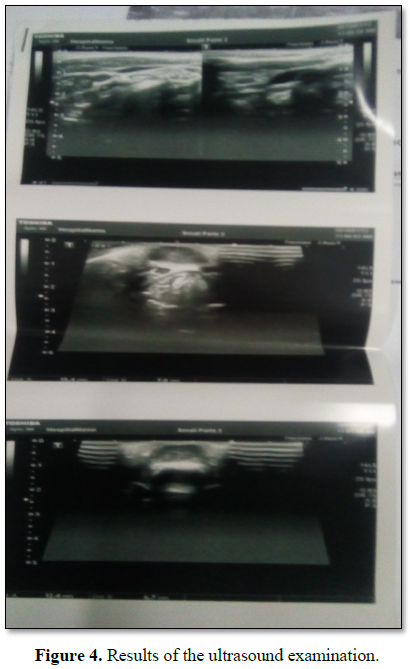
On the first echo examination at the University clinic of radiology in the neck region, the oval heteroehogenic changes were measured with a dimension of 15.4 × 7 mm on the medial line of the neck, while signs of enlarged lymph glands are not detected bilaterally (Figure 4).
On the clinical examination by children surgeon a cystic formation in the anterior part of the cervical region was detected. At the moment of the examination the cyst was inflamed and movable in relation to the background. After two-weeks check-up in the ambulance with new ultrasound examination was recommended by children surgeon. The children surgeon in the ambulance makes a diagnosis of Cysta colli mediana.
The report of the ultrasound examination after two weeks shows that in the medial line of the cervical region, subcutaneous oval heterogenic changes were detected with a dimension of 12 × 7 mm (Figure 5). No signs of elevated lymph nodes were detected.
DISCUSSION
Cysta colli mediana is rare congenital lesion. They are usually asymptomatic, but if the cyst is large and present in cervical area [3].
Focal infections are associated with a number of changes in the blood vessels, due to the decrease of the total number of blood elements (due to the cytotoxic effect on pathological agents of the focus), with a percentage change in white blood vessels, also due to the allergic and toxic effects of pathological agents of the focus. The neutrophilia (an increased number of neutrophil granulocytes) may occur, but the picture may be changed depending on the stage of development of the disease. The fractured sedimentation on erythrocytes which was seen in the blood is not a specific moment for focus, but every time when focal infections are present fractured sedimentation of erythrocytes was noticed.
Very occasionally, secondary infection may occur which results in sinus tract formation and external drainage of purulent material, if the cyst is super facial as was in our case.
CONCLUSION
Definitive diagnosis is not always possible preoperatively and because of the risk of malignant transformation, we recommend the complete surgical excision of the cysta colli mediana.
1. Panovski J (1988) Special surgery. University Ss. Cyril & Methodius, Skopje.
2. Singla SL, Chauhan TS, Bhoriwal S, Singla S, Tarar V, Sharma S (2013) Unusual presentation of a congenital bronchogenic cyst in a young child. Int J Pediatr Neonatol 16.
3. Puscas L (2015) Midline cervical cleft: Review of an uncommon entity. Int J Pediatr 2015: 1-10.


QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Chemotherapy Research Journal (ISSN:2642-0236)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Allergy Research (ISSN:2642-326X)


