Image Article
Another face of Digoxin Toxicity
954
Views & Citations10
Likes & Shares
A 74-year-old man was referred from private clinic for evaluation of
dyspnea and abnormal electrocardiography (ECG) under suspicion of new onset
diabetes mellitus (DM). His medical history included benign prostate
hyperplasia, paroxysmal atrial fibrillation (PAF), and congestive heart failure
(CHF) on medications. His blood pressure was 134/62 mmHg and pulse rate was 75
bpm. He had a relatively healthy looking appearance and physical examination
was fine with regular heart beats without murmur. Initial chest X ray showed
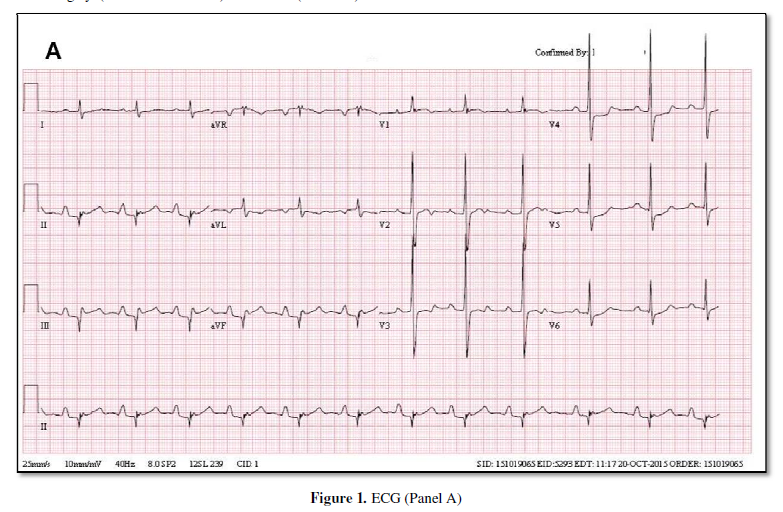
mild cardiomegaly (CT ratio was 0.60) and ECG (Panel A) showed sinus rhythm with PR interval prolongation and
ST-segment and T-wave forces opposite the direction of the major QRS forces
(scooped ST segment), suggesting digoxin toxicity. His current medications were
warfarin 3mg, digoxin 0.25 mg, furosemide 20 mg once a day. We checked serum
digoxin level, glucose, electrolyte, renal function studies and other routine
laboratory studies to check digoxin toxicity and DM. Serum digoxin level was
1.8 ng/mL and fasting serum glucose level was 134 mg/dL. Hemoglobin A1C level
was 5.8%. He had abdominal discomfort and dyspepsia
about a month ago, and he drank daily soda twice or three times a day since he felt dyspepsia. We suspected
hyperglycemia caused by soda containing lots of sugar (sprite in his case) to
facilitate digestion for folk remedy. We made him stop taking digoxin and
drinking soda and we prescribed beta blocker instead. He recovered completely
after one month, as restoration of T wave abnormality (Panel B) and normalized fasting serum glucose level (99 mg/dL).

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Chemotherapy Research Journal (ISSN:2642-0236)
- International Journal of Diabetes (ISSN: 2644-3031)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
")
")



