1073
Views & Citations73
Likes & Shares
Introductıon: The aim of this study is to compare maternal
and perinatal outcomes in HELLP Syndrome (hemolysis, elevated liver enzymes and
low platelet count) and severe preeclampsia cases.
Materıals and methods: This study was conducted between January
2015 and January 2018 in the Gynecology and Obstetrics and Gynecology Clinics
of Zekai Tahir Burak Training and Research Hospital. The aim of this study was
to retrospectively examine the files of the maternal and perinatal outcomes.
Between these dates, 50.000 births (C/S: 10,000 patients, Normal spontaneous
birth: 40,000 patients) occurred in our hospital. Severe preeclampsia or HELLP total
incidence is 1.40% in our study period. The incidence of HELLP is 0.26% and
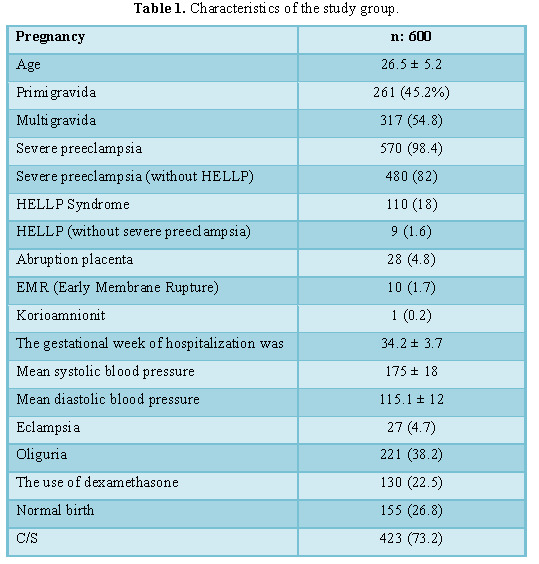
severe preeclampsia is 1.35%. The mean age of 600 patients was 26.5 ± 5.2. 45%
of the patients were primigravid, 90.2% were severe preeclampsia and 25% had
normal spontaneous delivery. Severe preeclampsia and HELLP 110 (18%) were seen
at the same time without HELLP, only severe preeclampsia was present in 480
(82%), and only HELLP was in 10 (1.8%). Statistical analyses were performed
using the Chi-square (X2) test with Yates’ correction, the Student’s
t test, logarithmic transformation, and the logistic regression method.
Conclusıon: HELLP syndrome caused more maternal complications
than severe preeclampsia.
INTRODUCTION
Atrial fibrillation (AF) is the most common
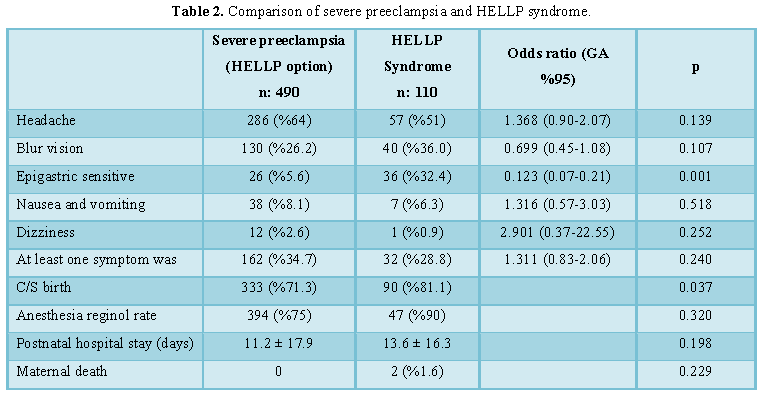
sustained While 60% of women with severe pre-eclampsia have a headache symptom,
this figure is 52.3% in patients with HELLP Syndrome. However, this difference
was not statistically significant (p=0.189) (p>0.05). Similarly, there was
no statistically significant difference between severe preeclampsia and HELLP groups
in terms of visual acuity, nausea and vomiting, dizziness and at least one
symptom (p>0.05) (Table 1). Epigastric sensitivity in patients with HELLP
Syndrome (Table 2). 32.4% were higher than the patients with severe
preeclampsia (5.6%) and this difference was statistically significantly higher
(p<0.001). The rate of birth with C/S patients with severe preeclampsia was
333 (71.3%) and in patients with HELLP Syndrome was 90 (81.1%), and this
difference was statistically significantly higher in the HELLP group than in
the Heavy preeclampsia group (p=0.037). The mean APGAR score of the patients
with severe preeclampsia was 8.3 ± 1.3 and the mean score was 7.0 ± 1.5 in the
patients with HELLP Syndrome and this difference was found to be significantly
higher in favor of the severe preeclampsia group (p=0.012). In patients with
severe preeclampsia, the need for intensive care was 53.2% and in patients with
HELLP Syndrome was 69.5% and this difference was significantly higher in favor
of the Hellp group (p=0.002) (Table 2).
The total incidence of severe
preeclampsia or HELLP syndrome at 50.000 births in our hospital is 1.41%. The
incidence of HELLP syndrome is 0.27% and severe preeclampsia rate is 1.39%. In
our study, epigastric sensitivity (32.4%), birth rate 90% (81.1%) with C/S,
postpartum oliguria, blood products, platelets, erythrocytes and fresh frozen
plasma transfusion, and hematoma ratio (3.6%), postpartum BUN and creatinine
values, rate of ABY (8.1%), at least one complication rate (62.2%), maternal
intensive care needs and need for mechanical ventilation, NEC, intensive care
needs of babies (69.5%), mechanical ventilation requirement (31.4) and duration
of intensive care unit stay (13.1 ± 18.5 days) and neonatal mortality rate
(14.3%) were significantly higher than severe pre-eclamptic group. The
gestational week of hospitalization in HELLP syndrome (33.1 ± 3.6), gestational
week at birth (33.2 ± 3.6), hospitalization time (0.7 ± 1.1 days), birth weight
(1970.2 ± 740 g), hemoglobin and hematocrit values, APGAR 1.dk and APGAR 5.dk
scores are significantly lower and statistically significant than severe
pre-eclamptic group.
We found that laboratory
findings other than the diagnostic criteria of HELLP Syndrome were similar in
both groups and they were not statistically significant. We found only 10% less
postpartum complications in patients with severe preeclampsia. We found that
the simultaneous presence of HELLP Syndrome and severe preeclampsia increased
the postpartum complication rate by 8.4 fold, but there was no relationship
between the patients with HELLP Syndrome and postpartum complication. In our
study, we found that presence of acid in the abdomen, oliguria, C/S, AST ≥ 70
ü/l, Platelet count, serum creatinine ≥ 1.36 mg/dl increased, maternal
postpartum complication development. While 10.9% of women with severe
preeclampsia had a history of hypertension in their previous pregnancy, 6.5% of
women with HELLP Syndrome had a history of hypertension in previous pregnancies.
However, this difference was not statistically significant (p=0.146). While
8.6% of women with severe preeclampsia had a history of chronic hypertension,
8.1% of women with HELLP Syndrome had a history of chronic hypertension.
However, this difference was not statistically significant (p=0,876)
(p>0.05). In a study performed by Martin et al. it was found that laboratory
findings other than diagnostic criteria of HELLP Syndrome were similar in both
groups and +3, +4 proteinuria in both groups were similar [3,12].
DISCUSSION
Caritis et al. reported that
preeclampsia was observed more frequently in patients with pre-pregnancy
hypertension [9]. In other studies, pregnant women who had severe preeclampsia
and eclampsia in their previous pregnancy started that the risk of recurrence
pregnancies increased [1,6,11]. However, there is no adequate study comparing
severe preeclampsia and HELLP syndrome in terms of risk factors. When we
compared severe preeclampsia with HELLP Syndrome in our study, we found that
epigastric sensitivity was higher in patients with HELLP Syndrome (32.4%) than
in patients with severe preeclampsia (5.6%) and this difference was
statistically significant (p<0.05) (Table
2). In a study by Martin et al. found headache to be more common in
patients with severe preeclampsia than HELLP Syndrome; Epigastric sensitivity
was significant in both studies in favor of HELLP Syndrome. The most common
clinical symptoms of HELLP syndrome are fatigue, epigastric tenderness and pain
[6,10]. We can say that this symptom is more stimulating in terms of HELLP Syndrome.
In our study, we found that the
rate of birth with C/S was higher in 90 patients (81.1%) compared to 333
(71.3%) in severe preeclampsia group. Similarly, in different studies, C/S
ratio was reported to be higher in HELLP Syndrome compared to severe
preeclampsia [1,2,5]. We think that HELLP Syndrome is more risky in terms of
both maternal and perinatal mortality and morbidity compared to severe
preeclampsia and necessitates urgent delivery.
The mean postpartum hospital
stay was 11.2 days in the severe preeclampsia group and 13.6 days in HELLP
Syndrome but this was not statistically significant. In the study of Kumru et
al. there was no difference in the length of hospital stay between the two groups
[4]. However, in a study by Martin et al. in HELLP Syndrome, this time is
longer and this is due to the increased incidence of postpartum complications
in HELLP Syndrome and thus increased the need for hospitalization [3,12].
In our study, Systolic blood
pressure was ≥ 160 mm Hg, diastolic blood pressure ≥ 110 mm Hg, headache,
blurred vision, epigastric tenderness, nausea-vomiting, dizziness, gestational
age at birth (p>0.05). In the study of Philippe et al. unlike our study,
postpartum complication development was 2.55 times the systolic blood pressure
≥ 160 mm Hg and C/S 2.11 fold increased especially after the delivery was
performed. Perinatal mortality rate has been reported to very between 7.7% and
60% in patients with HELLP Syndrome [5,6-8]. In our study, we found this rate
to be 14.3%. We attributed the relatively low rate to a tertiary center and the
availability of our intensive care conditions.
CONCLUSION
Severe preeclampsia and HELLP
syndrome increase maternal-perinatal morbidity and mortality rates especially
in developing countries. In our study, we found that especially HELLP syndrome
caused more maternal complications than severe preeclampsia. However, although
neonatal morbidity and mortality can be explained by the small gestational age,
we could not reach a clear conclusion about the reason of poor neonatal
outcomes in HELLP Syndrome because the gestational age is smaller than the
severe preeclampsia.
1.
Chesley LC, Cooper DW (1986)
Genetics of hypertension in pregnancy: Possible single gene control of
preeclampsia and eclampsia in the descendants of eclamptic women. Br J Obstet
Gynecol 93: 898-908.
2.
Abramovici D, Friedman SA,
Mercer BM, Audibert F, Kao L, et al. (1999) Neonatal outcome in severe
preeclampsia at 24 to 36 weeks’ gestation: Does the HELLP (hemolysis, elevated
liver enzymes and low platelet count) syndrome matter? Am J Obstet Gynecol 180:
221-225.
3.
Martin JN Jr, Rinehart BK, May
WL, Magann EF, Terrone DA, et al. (1999) The spectrum of severe preeclampsia:
Comparative analysis by HELLP (hemolysis, elevated liver enzyme levels and low
platelet count) syndrome classification. Am J Obstet Gynecol 180: 1373-1384.
4.
Kumru S, Fiimflek M, Güratefl
B, Sapmaz E, Özcan Z, et al. (2005) Comparison of maternal and perinatal
outcomes of HELLP syndrome and severe preeclampsia cases. Perinatal J 13.
5.
Harms K, Rath W, Herting E, Kuhn
W (1995) Maternal hemolysis, elevated liver enzymes, low platelet count and
neonatal outcome. Am J Perinatol 1: 1-6.
6.
Sibai BM, Taslimi MM, El-Nazer
A, Amon E, Mabie CB, et al. (1986) Maternal perinatal outcome associated with
the syndrome of hemolysis, elevated liver enzymes and low platelets in severe
preeclampsia-eclampsia. Am J Obstet Gynecol 155: 501-509.
7.
Eeltink CM, van Lingen RA,
Aarnoudse JG, Derks JB, Okken A, et al. (1993) Maternal haemolysis, elevated
liver enzymes and low platelets syndrome: Specific problems in the newborn. Eur
J Pediatr 152: 160-163.
8.
Killam AP, Dillard SH Jr,
Patton RC, Pederson PR (1975) Pregnancy-induced hypertension complicated by
acute liver disease and disseminated intravascular coagulation: Five case
reports. Am J Obstet Gynecol 123: 823-828.
9.
Caritis S, Sibai B, Hauth J
(1998) Low-dose aspirin to prevent preeclampsia in women at high risk. National
Instutute of Child Health and Human Development Network of Maternal-Fetal
Units. N Engl J Med 338: 701.
10.
Steegers EAP, van der Post J
(1998) Hypertension in pregnancy. Textbook of Perinatal Medicine. Kurjak A
(ED). Bath, UK, the Parthenon Publishing Group, pp: 1889-1899.
11.
Delmis J (2006) Hypertension in
pregnancy. Croatian 128: 357-368.
12.
Kuyumcuoglu U, Celik Y (2011)
Are maternal and fetal parameters related to perinatal mortality in HELLP
syndrome? Arch Gynecol Obstet 283: 1227-1232.
-
 Table 1
Table 1 -
Table 2
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- Journal of Alcoholism Clinical Research
- International Journal of AIDS (ISSN: 2644-3023)
- Journal of Cell Signaling & Damage-Associated Molecular Patterns
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- Ophthalmology Clinics and Research (ISSN:2638-115X)
- Journal of Clinical Trials and Research (ISSN:2637-7373)


