2304
Views & Citations1304
Likes & Shares
Introduction: Diabetes mellitus is a chronic disease that
has been recognized by the Malaysian government as a major public health
problem with far reaching consequences not just for its adverse impact on the
health of Malaysians, but also for the economic burden it places on the health
care system.
Objective: To identify anti-diabetic
medication cost of type 2 diabetes mellitus treatment for outpatient visit in a
teaching hospital.
Methodology: Anti-diabetic medication cost was
determined by conducting a retrospective audit on 1077 patient medical records
at Universiti Sains Malaysia (HUSM) Teaching Hospital in Kelantan.
Results: Hospital
Universiti Sains Malaysia (HUSM) spent approximately RM1, 102,738 for anti-diabetics
medications for study population in 2008. The analysis show that average cost
of medication per patient per year was RM 1, 023.8.
Conclusion: The cost of anti-diabetic drugs is the
high. The most commonly prescribed anti-diabetic
treatment regimen for type 2 DM was gliclazide in combination with metformin. Much
attention and effort should be directed towards determining the burden of
diabetes in the HUSM in economic terms.
Keywords: Type 2 diabetes mellitus, Cost diabetic
medication treatment, Outpatient, HUSM
INTRODUCTION
Diabetes mellitus is a chronic disease that has been recognized by the
Malaysian government as a major public health problem with far reaching
consequences not just for its adverse impact on the health of Malaysians, but
also for the economic burden it places on the health care system. Diabetes
mellitus presents a high burden for individuals and society. This burden is not
only related to health care costs, but also to indirect costs caused by loss of
productivity from disability and premature mortality. Medical expenditures for
people with diabetes are 2-3 times higher than that for those not affected by
diabetes [1].
Effective disease management programmes that aim to prevent
complications could potentially lead to cost savings in managed care settings
[2]. Hayward et al. [3] found that patients taking insulin had 2.4 more
diabetic outpatient visits, used 300 more glucose test strips, and had slightly
higher laboratory costs per year than patients receiving sulphonyl ureas.
Johnson et al. [4] found that metformin, alone or in combination, was
the most frequently dispensed oral anti-diabetic medication. A longer duration
of diabetes was associated with increased use of oral medications and insulin
therapy. Insulin was used in approximately 12% of patients with type 2 DM and
was associated with approximately three times higher expenditure on diabetes
testing supplies compared with patients on oral anti-diabetic medications [4].
Objective of study to
identify anti-diabetic medication cost of type 2 diabetes mellitus treatment
for outpatient visit in a teaching hospital.
MATERIAL AND METHODS
Medications cost
This was the cost of anti-diabetic
medications used in treating diabetic patients either oral anti-diabetic
medications or insulin or combination of oral anti-diabetic medications and
insulin therapies.
Cost calculation for anti-diabetic medications among type 2 diabetes
mellitus patients
All costs were valued in year 2008 constant RM (RM3.21=1 USD).
Medications cost was the anti-diabetic medications cost used in treating type 2
DM. All the anti-diabetics medications used in type 2 DM treatments within one
year period (2008) were recorded in terms of their daily dose and frequency and
totaled-up for one year duration. Drugs cost was calculated multiplying by
their unit cost based on price taken from inventory units, HUSM pharmacy
department.
Data entry and Statistical analysis
Data entry and analysis were conducted using statistical packages for
social sciences (SPSS) version 12.0.1 (SPSS Inc., 2003).
Data were checked and explored. First, editing process was done, which
include preliminary data screening (observing missing values) and correcting
data points. The original data were reviewed again and the required changes if
any error were made during the editing phase. The data set was then explored
for the outliers by histogram, box plot and by statistical test. To confirm the
presence of all the outliers, the researcher checked for the possibility of
recording error and data entry process.
Distributions and frequencies of the independent variable were
examined. Data exploration was done including descriptive statistics. All
continuous variables were expressed as mean and standard deviation for normal
distribution and median and interquartile range for skewed data. Frequencies
and percentages for categorical variables were calculated. Meaningful
combination of categories was done when it was indicated.
In current study the cost of anti-diabetic medications were calculated
for one year. Descriptive analysis was used.
RESULTS
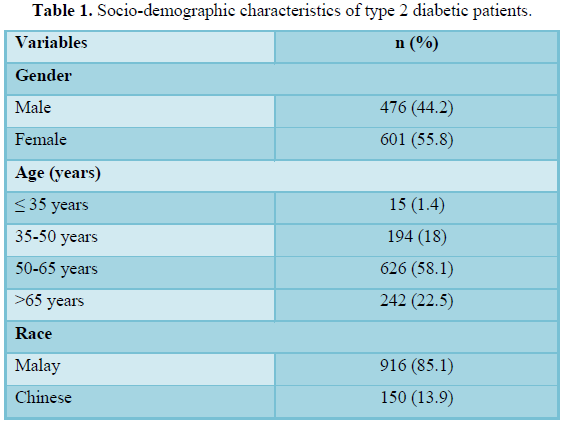
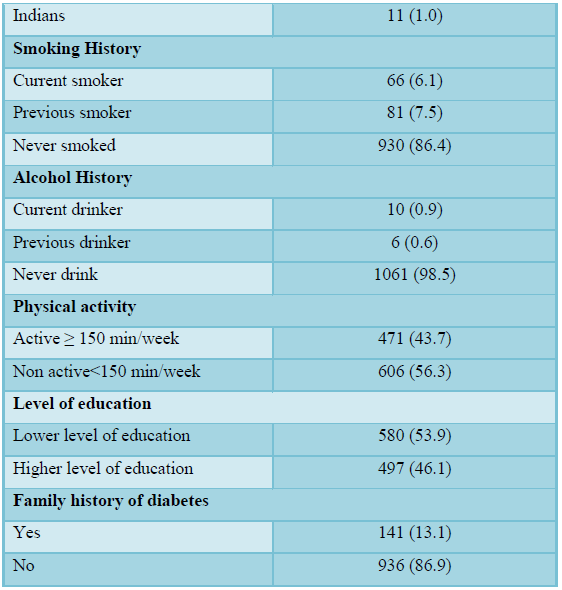
A total of 1077 type 2 diabetic patients were involved in this study.
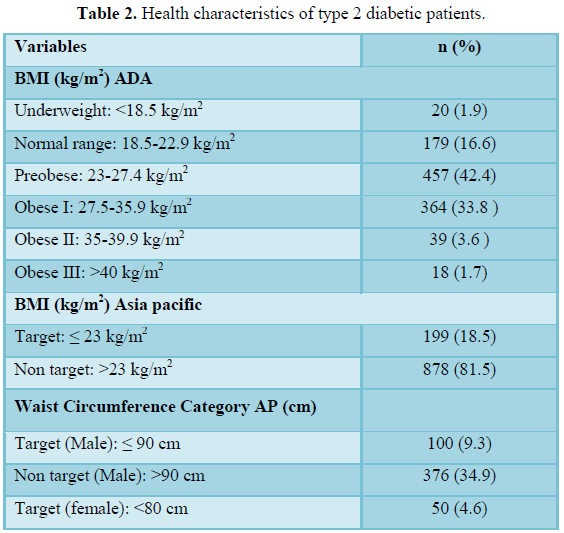
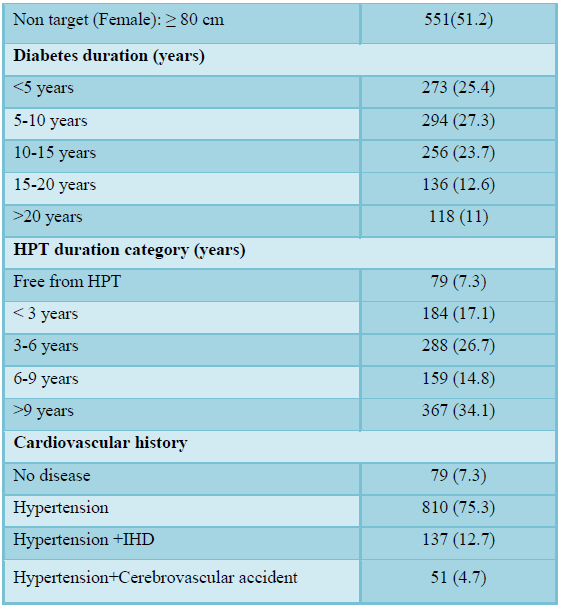
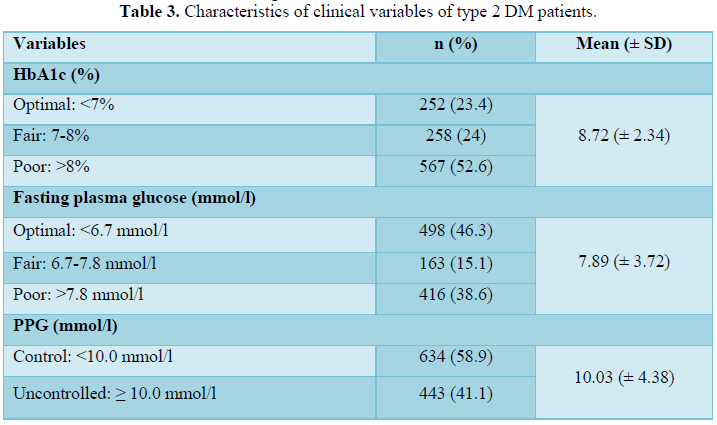
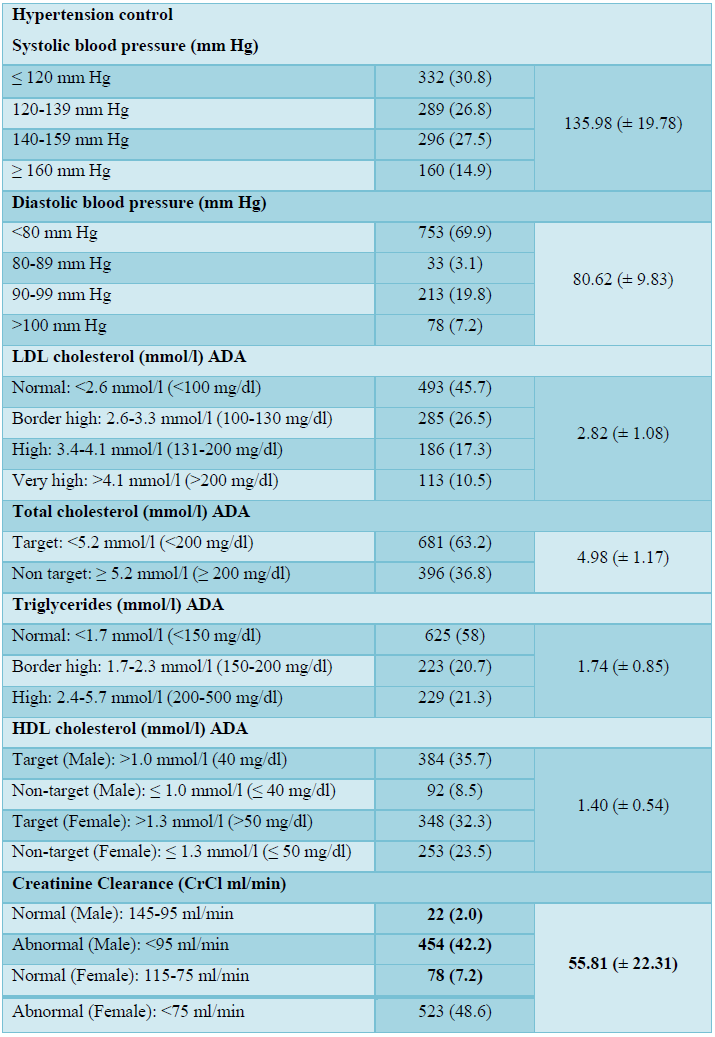
Descriptive statistics were used to describe the sociodemographic characteristics of patients as shown in Table 1. The health and clinical
characteristics of the patients are shown in Tables 2 and 3, respectively.
A total of 476 (44.2%) of patients in this
study were males and 601 (55.8%) were females. According to racial
distribution, 916 (85.1%) were Malay, 150 (13.9%) were Chinese and 11 (1.0%)
were Indians. This proportion of ethnic group is generally representative of
the Kelantan population. The age of patients recruited in this study range was
from 18 to 88 years and was categorized into four groups. Majority 626 (58.1%)
of patients in this study were in age group more than 50-65 years. This was
followed by the age group of >65 years and 35-50 years which consisted of
242 (22.5%) and 194 (18%), respectively. Furthermore, the least affected group
was ≤ 35 years 15 (1.4%).
Concerning the level of education, the literacy level of the patients was
moderate. More than half of the patients 580 (53.9%) in this study had a lower
level of education, whereas 497 (46.1%) patients had a higher level of
education.
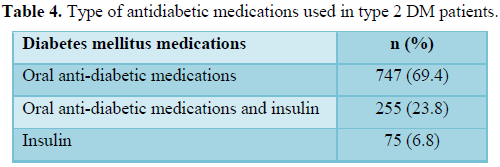
Type of anti-diabetic
medications used in type 2 diabetes mellitus patients
In this study most of the patients, a total
of 747 (69.4%) were on oral anti-diabetic medications for management of
diabetes mellitus, while 255 (23.8%) were on combination of oral anti-diabetic
medications and insulin and only 75 (6.8%) were on insulin injection alone (Table
4).
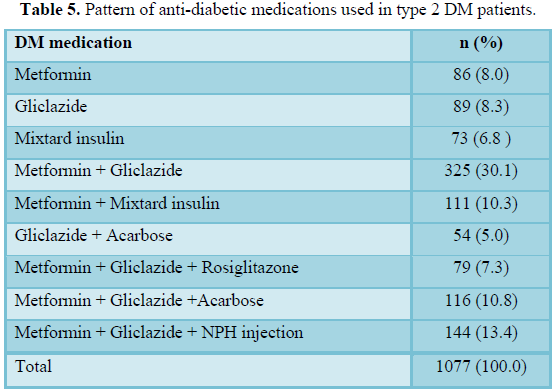
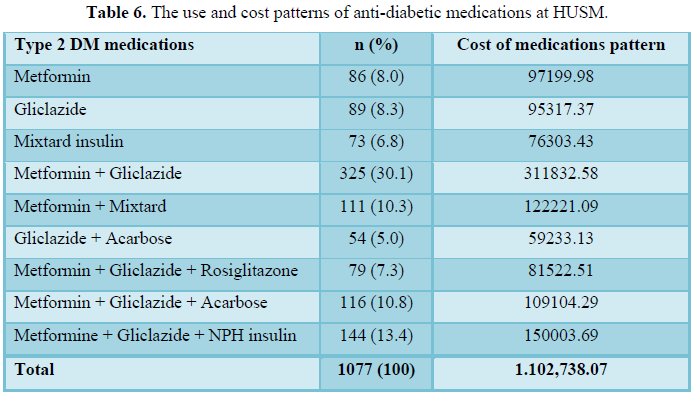
Pattern of anti-diabetic
medications used in type 2 DM patients
Out of 1077 type 2 diabetic patients, 325
(30.2%) were on combination of metformin and gliclazide, 144 (13.4%) were
taking metformin, gliclazide and NPH insulin, 116 (10.8%) were taking
combination of metformin, gliclazide and acarbose, 111 (10.3%) were taking
metformin and mixtard insulin injection, while 89 (8.3%) were taking gliclazide
alone and 86 (8.0%) were taking metformin only (Table 5).
The use of anti-diabetic
medications among type 2 diabetes mellitus patients
Out of 1077 type 2 DM patients, most of patients
747 (69.4%) were on oral anti-diabetes medications for managements of diabetes
mellitus, while 255 (23.8%) were on combination of oral anti-diabetic
medication and insulin, and only 73 (6.8%) were on insulin injection. The 248
(23.1%) were prescribed with single anti-diabetic agents; 490 (45.5%) were
prescribed two drugs-class anti-diabetic agents and 339 (31.5%) were prescribed
three combination of anti-diabetic medications.
Metformin was the main anti-diabetes drug
class used, either as a single agent or in combination with gliclazide or
insulin. Metformin was prescribed to 861 patients out of the 1077 subjects
studied, which was about 80%. On the other hand, gliclazide was prescribed to
804 (75%) patients and emerged as the second main anti-diabetes drug class used
in the present study. The use of anti-diabetic agents in HUSM was shown in Table
6.
Cost analysis of
anti-diabetic medications for type 2 diabetes mellitus
Hospital Universiti Sains Malaysia (HUSM)
spent approximately RM1, 102,738 for anti-diabetics medications for study
population in 2007. The analysis show that average cost of medication per
patient per year was RM 1, 023.8 (Table 7).
Type 2 DM is considered as one of the most
prevalent and costly chronic conditions in the world. The costs and prevalence
of this disease are increasing. The burden of diabetes on patients and the
health care system is enormous and it is predicted that the incidence,
prevalence, and costs associated with treating diabetes will rise [5-7]. The
present study evaluated the annual direct medical costs for patients with type
2 DM during a follow-up period of one year. The current study provides valuable
information to our health care providers and policy makers regarding the
planning of health care programmes, particularly in the public sector.
Furthermore, this is the first study in Malaysia to evaluate the annual direct
medical costs in the HUSM. Diabetes causes
a significant health burden for patients, and the care of this population is a
substantial economic burden on society. A study by Al-Sadat [8] showed that
medical expenditures for people with diabetes are two to three times higher
than for those not affected by diabetes. In another study, Suhaiza et al. [9]
reported that the annual costs of providing care were 2.4 times greater for
diabetic members than for the non-diabetic group of the same age and sex.
DISCUSSION
The mean age of all of the patients was 58.3 years (± 9.8). This
finding agreed with the study by King et al. [10], who found that most of the
type 2 diabetic patients were older than 50 years. The onset of type 2 DM occurs at maturity, which is normally after age of 45 years. The major population in
Malaysia consists of Malay people and the percentage of Malay diabetic patients
was the highest in this study, located in the Malay populated state of
Kelantan.
The use and cost of anti-diabetic medications
patterns at HUSM
In this study, the most frequently used anti-diabetic medication
was metformin (80%), which was used alone or in combination with other anti-diabetic
medications, followed by gliclazide. The low cost of metformin might be the
reason for the wide use of this drug. Gliclazide was prescribed to 75% of the
patients and emerged as the second main anti-diabetes drug class used in the
present study. Although the unit cost of gliclazide is expensive compared to
other anti-diabetic medications, such as sulfonylureas and metformin,
gliclazide was widely used either as a single agent or in combination therapy,
probably because it was shown to increase insulin secretion, to be more
protective against β-cell failure and to have anticytokine properties, and a
study by Mamputu et al. [11] reported that gliclazide has anti-oxidative
properties which might decrease vascular smooth muscle cell dysfunction and
prevent cardiovascular diseases in type 2 DM patients.
For oral anti-diabetic combination therapy, the combination of metformin
and gliclazide was used the most frequently. Out of all of the patients, 93% were on metformin or gliclazide alone
or in combination and more than 61% were on combination therapy with gliclazide
and metformin. The most commonly used
combination therapy for type 2 diabetic patients in a study by DeFronzo et al.
[12] was biguanide plus sulfonylurea. A found that the combination of
gliclazide and metformin had the advantages of lipid lowering properties over
the glibenclamide and metformin combination and that it was better in
controlling the blood glucose level and reduced the risk of hypoglycaemia in
comparison to glyburide. These might be the reasons why this combination
therapy is used more frequently.
The cost of anti-diabetic
medications
The anti-diabetic medication cost was as the dominant cost factor in the
annual total treatment costs because it contributed to about 59.2% of the total
treatment costs. The type of anti-diabetes agent used was the major factor
affecting the annual treatment cost per patient. The use of expensive drugs
such as mixtard insulin, acarbose and rosiglitazone caused the high annual
treatment costs. Thus, the use of the treatment regimen depends on many other
factors including the availability of the drugs, patient compliance, and the
preference of the physician.
The results showed that insulin users incurred higher outpatient
treatment costs per year per patient. This finding is similar to the findings
of a previous study [13]. The use of insulin in patients in this study was
limited. There were 6.8% who used insulin alone, and only 23.8% used insulin
combined with oral anti-diabetic medications. It was found that the cost of
anti-diabetic treatment in the present study was RM 1,102,738 and the cost of
anti-diabetic medications per patient in 2008 was estimated to be RM 1023.9.
CONCLUSION
The cost of anti-diabetic drugs constitutes the highest proportion of the
costs. The most commonly prescribed anti-diabetic treatment regimen for type 2
DM was gliclazide in combination with metformin. Thus, it is impossible to
avoid the costs incurred in maintaining blood glucose control. Much attention
and effort should be directed towards determining the burden of diabetes in the
HUSM in economic terms. The present study recommends that more time, money and
attention must be given to the treatment of diabetic patients.
ACKNOWLEDGMENT
The authors would like to thank Universiti Sains Malaysia (USM) for the financial support provided for this research.
1.
Rubin RJ, Altman WM, Mendelson DN (1992) Health care
expenditures for people with diabetes mellitus. J Clin Endocrinol Metab 78:
809A-809F.
2.
Selby JV, Ray GT, Zhang D, Colby CJ (1997) Excess
costs of medical care for patients with diabetes in a managed care population.
Diabetes Care 20: 1396-1402.
3.
Hayward R, Manning W, Kaplan S, Wagner E, Greenfield
S (1997) Starting insulin therapy in patients with Type 2 DM: Effectiveness,
complications and resource utilization. Am Med Assoc 278: 1663-1669.
4.
Johnson JA, Pohar SL, Secnik K, Yurgin N, Hirji Z
(2006) Utilization of diabetes medication and cost of testing supplies in
Saskatchewan. BMC Health Serv Res 6: 159.
5.
Boyle JP, Honeycutt AA, Narayan KM, Hoerger TJ,
Geiss LS, et al. (2001) Projection of diabetes burden through 2050: Impact of
changing demography and disease prevalence in the U.S. Diabetes Care 24:
1936-1940.
6.
Ohinmaa A, Jacobs P, Simpson S, Johnson J (2004) The
projection of prevalence and cost of diabetes in Canada: 2000 to 2016. Can J
Diabetes 28: 116-123.
7.
Wild S, Roglic G, Green A, Sicree R, King H (2004)
Global prevalence of diabetes: Estimates for the year 2000 and projections for
2030. Diabetes Care 27: 1047-1053.
8.
Al-Sadat N (2003) Direct costs of diabetes in an
outpatient setting in Malaysia. NCD Malay 2: 19-27.
9.
Suhaiza S, Ahmad NS, Jeriah I, Aziz AS, Wan Mohamad
WB, et al. (2004) Glycemic control among type 2 diabetic patients in Kelantan. NCD
Malaysia the Bulletin of Epidemiology and Public Health on Non-Communicable Disease
in Malaysia 3: 2-5.
10.
Setter S, White R, Campbell R (2000) Diabetes. In: Herfindal
ET, Gourley RD (eds.), Textbook of Therapeutic Drug and Disease Management.
Lippincott: Williams & Wilkins.
11.
Mamputu J, Renier G (2001) Gliclazide decrease
vascular smooth muscle cell dysfunction induced by cell-mediated oxidized
low-density lipoprotein. Metab Clin Exp 50: 688-695.
12.
DeFronzo RA (1999) Pharmacologic therapy for type 2
diabetes mellitus. Ann Intern Med 131: 281-303.
13.
Chale SS, Swai AB, Mujinja PG, McLarty DG (1992)
Must diabetes be a fatal disease in Africa? Study of costs of treatment. BMJ
304: 1215-1218.
14.
Zaini A (2000) Where is Malaysia in the midst of the
Asian epidemic of diabetes mellitus? Diabetes Res Clin Pract 50: S23-28.
15.
Selby J, Ettinger B, Swain B, Brown J (1999) First
20 months’ experience with use of metformin for type 2 DM in a large health
maintenance organization. Diabetes Care 22: 38-44.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6
-
Table 7
-
Table 8
-
Table 9
-
Table 10

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Rheumatology Research (ISSN:2641-6999)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Chemotherapy Research Journal (ISSN:2642-0236)
- BioMed Research Journal (ISSN:2578-8892)


