
4691
Views & Citations3691
Likes & Shares
Bimalleolar fractures are a type of ankle fractures characterized by involvement of the medial and lateral malleoli into the fracture line. Ankle fractures are one of the commonest traumatic injuries, accounting for a tenth of all fractures. They are also found to be among the common traumatic injuries requiring hospitalization. With an observed trend of rising incidence across the world and the paucity of data available on the pathology in this area, ankle fractures require studies assessing the burden and management of the pathology in this region. Bimalleolar fractures account for approximately one-fourth of ankle fractures and are the focus of this study.
Falls, sports and road traffic accidents account for most cases of bimalleolar fracture [7-11]. Bimalleolar fractures have three classification systems; the Lauge-Hansen system which is mechanism-based, the Weber system and the AO/OTA system which is an expanded version of the Weber system. Weber Classification system of bimalleolar fractures approximates the severity of the fracture and plays a role in management [12]. Management of bimalleolar fractures can be non-operative and operative, ranging from immediate weight-bearing to surgery and 12 weeks non-weight-bearing, depending on the severity of the injury, rehabilitation and professional demands of each patient [13]. Ankle fracture severity can be defined and classified into three groups including unimalleolar, bimalleolar and trimalleolar. Bimalleolar and trimalleolar fractures have similar outcome patterns while unimalleolar fractures show a significantly different pattern [14]. Several studies have examined the differences between severity groups concerning functional outcomes and show conflicting results. Some concluded that a fracture severity classification is a consistent predictor of functional outcome following surgery [15-17]. However, recent work by Egol [18] concluded that the type of fracture did not influence functional recovery [18]. Concomitant comorbidities should be investigated as they could significantly alter the management as well as recovery profiles.
The purpose of this study is to elicit epidemiological data on bimalleolar fracture cases, clinical patterns and assess early post-operative outcome patterns.
RESEARCH OBJECTIVES
General Objective
To determine the epidemiological characteristics and clinical patterns of bimalleolar fractures and evaluate the short-term outcome patterns.
Specific Objectives
The specific objectives of this study are:
- To determine the epidemiological characteristics of bimalleolar fractures.
- To describe the clinical patterns of bimalleolar fractures.
- To determine the short-term outcome patterns.
Research Scope
This study included cases of bimalleolar fractures at the Limbe Regional Hospital, Buea Regional Hospital, and St. Luke Clinic Buea between January 2010 and December 2019. It excluded cases with inadequate patient information for the study.
METHODOLOGY
Study Design
This was a hospital-based retrospective observational study carried out in the surgical departments of the Limbe Regional Hospital, Buea Regional Hospital and St. Luke Clinic Buea on admission files of bimalleolar fractures between January 2010 and December 2019.
Study Duration
This study was carried out between February 2020 to May 2020.
Study Area
This study was carried out in the aforementioned centers, all located in the South West Region.
The study was carried out in the Limbe Regional, Buea Regional Mutengene Baptist Hospital and St Luke Medical Centre. These hospitals are located in the South West region of Cameroon in the towns of Limbe, Mutengene and Buea. The Limbe Regional Hospital (LRH) is located in the town of Limbe, head quarter of the Fako division. Limbe, former Victoria also known as the town of friendship, is a seaside city in the south west region of Cameroon with a population of about 200.000 inhabitants. The LRH is a secondary health care facility which has the four main departments which include Internal medicine, Pediatrics, Obstetrics and Gynecology and Surgery with each department having specialists, general practitioners and nurses. It also has some specialized units like Ophthalmology, Dentistry, Neonatology, orthopedic surgery, Medical imaging unit and an Intensive care unit. The hospital has one orthopedic surgeon. The Buea Regional Hospital is found in Buea in the Fako Division of the South West Region of Cameroon on the foot of the mount Cameroon. The hospital is made up of many units including the following: the medical unit (male and female), the surgical unit, the pediatrics unit, the maternity unit, the HIV/AIDS unit, the Laboratory unit, the X-ray unit, the hemodialysis unit, the Tuberculosis unit, the Diabetes unit, the theatre department and the Out-Patient department (OPD). Each of the Unit is headed by a specialist doctor. The Buea Regional Hospital (B.R.H) serves patients from all over Buea and its environs. It admits clients for as long as they can stay and get well and also carries out minor and major surgery such as orthopedic surgery. St. Luke Clinic Bokwai is a private health facility found in Buea that specializes in orthopedic surgery. The institution has been operational for 11 years, is adequately staffed and appropriately equipped to handle bone fracture cases. It is a reference center for orthopedic cases in Fako division. It is run by an orthopedic surgeon and his team. These are three of the main orthopedic centers in the South West region.
Study Population and Sampling
The files studied were of patients diagnosed with bimalleolar fractures at the three centers included in this study from January 2010 to December 2019.
Inclusion Criteria:
- Files of patients with bimalleolar fractures.
Exclusion Criteria:
- Admission files lacking adequate data.
Sampling Method:
- Convenience sampling was used in this study by identifying cases of bimalleolar fracture admissions at the surgical departments of the centers included in this study.
Study Procedure
Administrative Procedure
Ethical clearance was obtained from the institutional review board of the Faculty of Health Sciences of the University of Buea. Ethical Approval was issued on February 4th 2020 with reference 2020/1127-1/UB/SG/IRB/FHS. Administrative Authorization from the Delegation of Public Health South West region was issued on March 26th 2020 with reference R11/MINSANTE/SWR/RDPH/PS/608/864 and from the Faculty of Health Sciences with reference 2020/664/UB/AA/VD/RC/FHS. Administrative clearance was obtained from the Buea Regional Hospital, Limbe Regional Hospital and St. Luke Clinic Buea to carry out this study, all seen in the Appendix.
Data Collection
It constituted admission file study at the surgical departments of the Buea Regional Hospital, Limbe Regional Hospital and St. Luke Clinic Buea. Admission files of patients with bimalleolar fractures were identified and retained for further study. The data on demographics, past history, bimalleolar fracture classification, management and early post-treatment outcome for each patient was obtained and recorded on a concise data collection sheet.
Data Management and Analysis
The data collection sheets were checked each time they were returned from the field for completeness and use of correct code. The sheets were coded with each question given nominal values for the number of options available, with the figure 9.00 attributed to unspecified data in the files. This coding sequence was then used to input data into the SPSS 23.0 software for analysis. Data was saved secretly in a computer with other backups as a precautionary measure. Analysis of each specific objective was done as follows:
Frequencies and proportions are used to describe categorical variables, while mean and standard deviation are used to describe quantitative variables. The inferential statistics used were the one sample T-test and Chi square test where appropriate. The alpha criterion for statistical significance was set at a p value of 0.05, confidence interval at 95%.
Ethical Considerations
The admission files were diligently processed such that patient confidentiality was preserved. Each form identified with a serial number and core ethical principles respected in the data collection, management and analysis process.
RESULTS
Epidemiological Data
The admission file study identified 178 cases of bimalleolar fracture. Of these, 11 files were excluded from analysis due to inadequate patient data. Hence, 167 admission files were included in this study (Figure 1).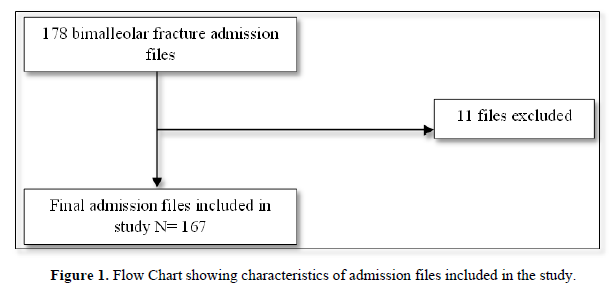
Demographic Profile
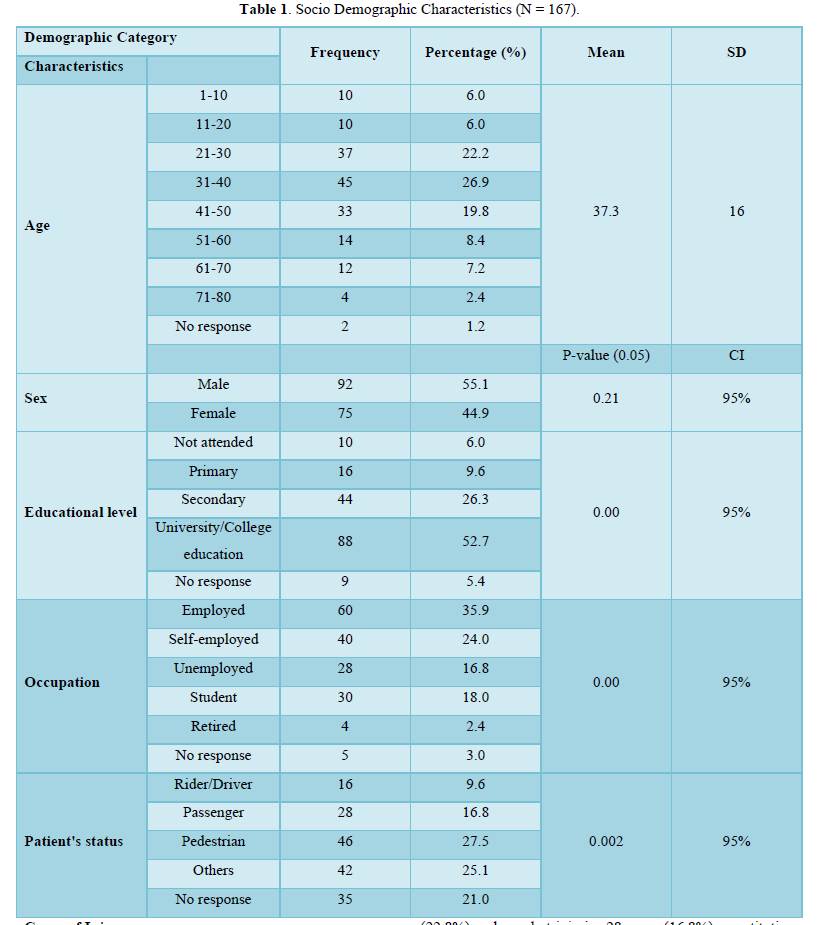
The patient files sampled had a sex distribution of 92 males (55.1%) and 75 females (44.9%) (p=0.21, 95% CI). In terms of patient age, the data indicates that bimalleolar fractures are most prevalent amongst patients between the ages 31-40 (45 cases, 26%), 21-30 (37 cases, 22.8%), and 41-50 (33 cases, 19.6%). The mean age stood at 37.3(±15.80), distribution demonstrated on Figure 2.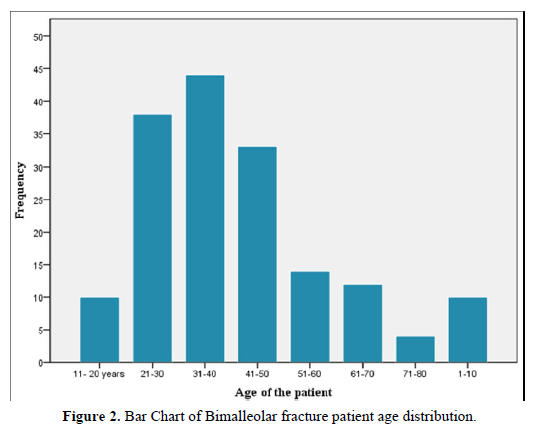
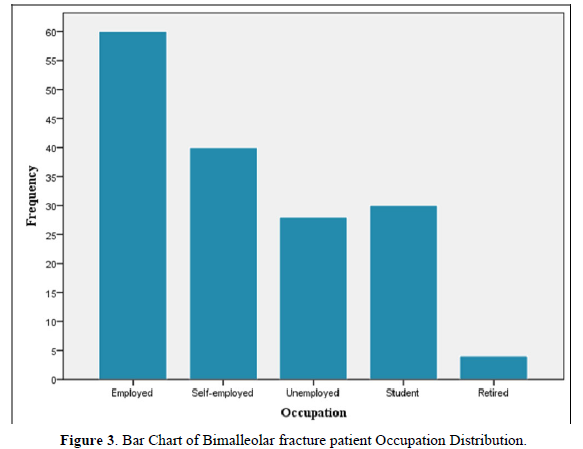
Bimalleolar fractures are more prevalent amongst the employed with 60 cases (35.9%), self-employed (40 cases, 24%) and students (30 cases, 18%) (p=0.00, 95% CI). It was lowest amongst the retired with 4 cases (2.4%) and unemployed with 28 cases (16.8%). Patients with university education recorded higher rates of bimalleolar fractures with 88 cases (52.7%) (p=0.00, 95% CI). The study found 27.5% of bimalleolar fractures were on pedestrians, making the set the most vulnerable group (p=0.002, 95% CI). Figure 3 shows the distribution of the cases according to occupation. Table 1 below shows the demographic characteristics of the patients in this study.
Cause of Injury
Road traffic accidents account for as many as 78 cases (46.8%) of the bimalleolar fracture patients, falls 38 cases (22.8%) and gunshot injuries 28 cases (16.8%), constituting the major causes for ankle injury. Table 2 below details the distribution.
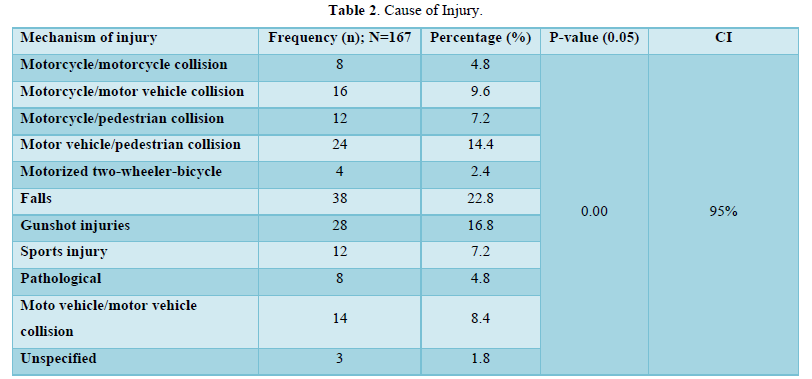
The study split road traffic accidents into the different likely scenarios to ascertain which vehicles are most culpable in causing bimalleolar fractures. Pedestrians (27.5%) were the most vulnerable group in the cases caused by road traffic accidents and the data shows motor vehicle accounted for the largest proportion of these crashes. Data on the speed of the vehicle on impact and the degree of energy involved in the collision was lacking however, the literature indicates bimalleolar fractures-ankle fractures in general-are low energy injuries. Gunshot injuries accounted for a significant proportion of the bimalleolar fractures in the study. In the literature on ankle fractures falls, sports and road traffic accidents account are the commonest causative scenarios [10,11].
Clinical Presentation
Every patient presented with pain on the affected ankle. Most patients also presented with limb deformity, inability to bear weight and swelling as seen in Table 3 below.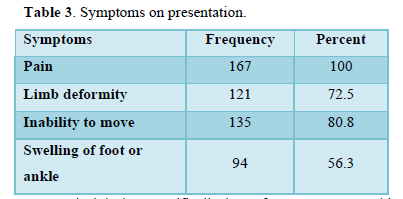
Traumatic injuries, specifically bone fractures, present this pattern of symptomatology however psychological response ranges from conservation withdrawal through the spectrum of denial, anxiety, anger and in some cases depression. Various causes of psychological disturbance in trauma patients have been elicited. These include pain, the acute and unexpected nature of the events, and these include in-hospital management like procedures and interventions necessary to resuscitate and stabilize the patients. Specific problems that concern the trauma patient psychologically include helplessness, humiliation, threat to body image and mental symptoms. In some cases, the patients suffer from depression, delirium and post-traumatic stress disorder. Some interventions which prevent and limit such conditions include adequate pain relief, prevention of sleep and sensory deprivation, providing familiar surroundings and careful explanations and reassurance of the patient about their condition. Psychotherapy and pharmacological management are necessary in some cases [19].
Medical History
The study investigated the presence of relevant past history in the cases of bimalleolar fracture identified. Medical information likely to affect patient outcomes were investigated, and most patients did not have any relevant comorbidities as shown in Table 4 below.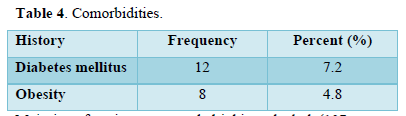
Majority of patients reported drinking alcohol (107 cases, 64.1%). However, just 14 cases (8.4%) reported smoking cigarettes. Majority (57, 76.6%) of female patients were not menopausal. Diabetes Mellitus has been shown to have a deleterious effect on wound healing which is in line with the pathophysiology of the disease [20]. Adequate blood glucose control is important in gaining optimal recovery in cases managed operatively with a past history of Diabetes. In this study, 12 cases (7.2%) had a past history of Diabetes. Obesity was tracked in this study as the condition has been shown to predispose individuals to greater severity of ankle fractures [21]. Studies also found the condition to have no impact on recovery patterns following management [22,23]. Obesity was seen in 8 cases (4.8%).
Smoking is an important risk factor for the occurrence of postoperative complications in ankle fracture patients [24]. Alcohol abusers were shown to suffer ankle fractures as the most common fracture in a study by Marley [25].
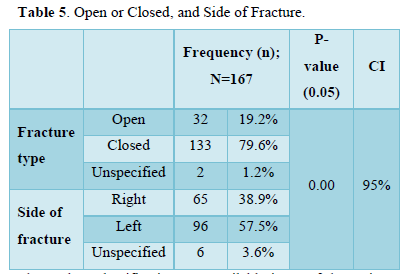
Clinical Pattern
The data revealed 133 cases were closed fractures (79.6%), while 96(57.5%) of the fractures were on the left ankle as shown in Table 5 below.
The Weber Classification was available in 54 of the patient files studied. Of these, 46.4% were found to be Type B, while Type C was the least common bimalleolar fracture type in this study. The data distribution is shown in Table 6 below.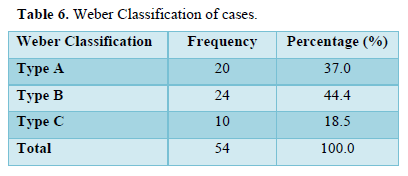
Road traffic accidents account for 28 (51%) of the Weber classified fractures, as well as most cases of Type A and B fractures. Falls account for an equal proportion of Type C fractures as road traffic accidents. X2 test revealed a significance of 0.133, meaning the relationship between the variables is not statistically significant at p value 0.05. There were 4 cases of obese patients with classification available, with 2 suffering Type B fracture and the other 2 Type C fracture. The association was statistically significant at a p value of 0.00(95% CI).
Management and Early Postoperative Outcome
Management
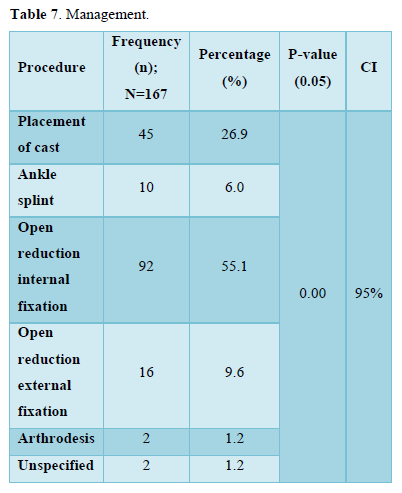
Definitive management was mostly open reduction internal fixation as it was used in 92 cases (55.1%). Other definitive procedures were placement of cast (45 cases, 26.9%), Open reduction external fixation (9.6%), ankle sprint (6%) and arthrodesis (1.2%). The distribution was statistically significant as seen in Table 7.
Arthrodesis in this study was carried out in cases of neglected bimalleolar fracture presenting with chronic intractable pain due to malunion arthritis. ORIF was the treatment of choice, particularly with the more severe fractures while placement of cast was most utilized in the less severe bimalleolar fractures. Correlation of management modality and fracture classification (54 classified cases) is shown below in Table 8.
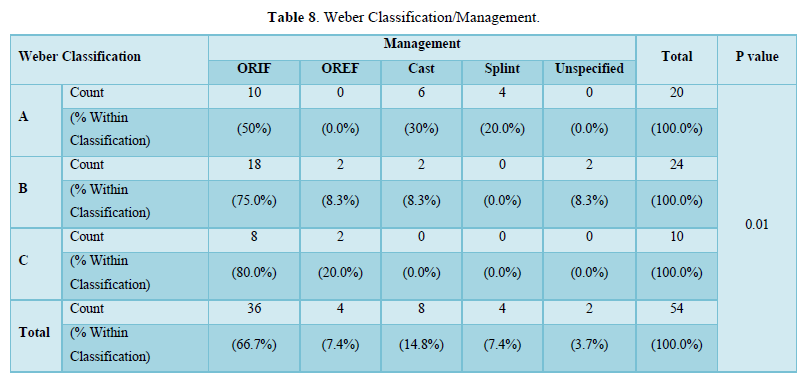
The correlation of fracture type to management shows Type A fractures have a 50% distribution between operative and non-operative management. This ratio falls greatly for Type B fractures with 83.3% managed operatively, while Type C fractures are entirely managed operatively. The Chi Square tests are all less than 0.05 meaning there is a positive statistically significant relationship between these two variables, with management modality dependent on the fracture type.
Outcome
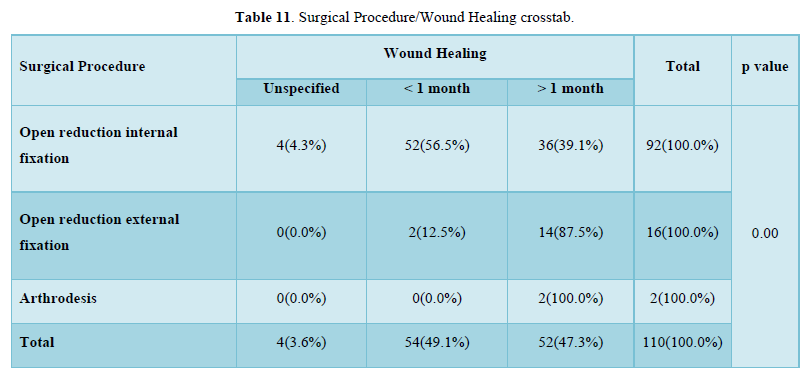
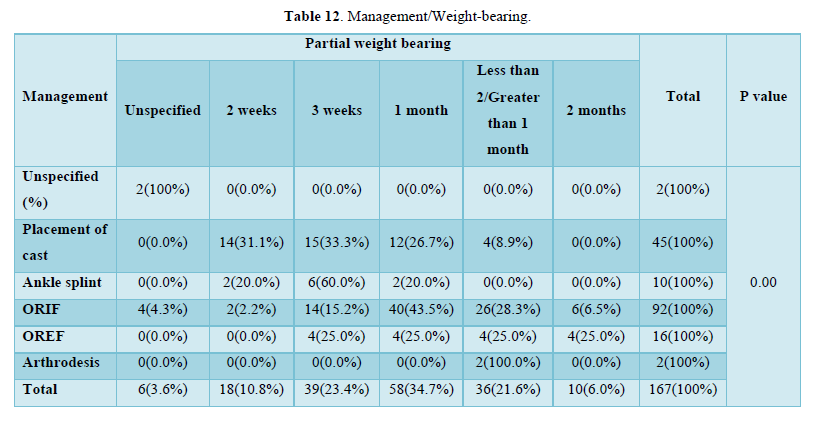
The early post-stabilization outcomes were investigated. SSI, wound healing and onset of partial weight-bearing used as markers of progress. Among the patients that underwent surgery [26], 6(5.5%) had an SSI postoperatively, 54(49.1%) wounds healed within a month while 52(47.3%) healed after a month. Most patients started partial weight-bearing at 1 month (58 cases, 34.7%) and three weeks (39 cases, 23.4%). Complete distribution is shown in Table 9 below & Correlation of surgical procedure to surgical site infection is shown in Table 10 below.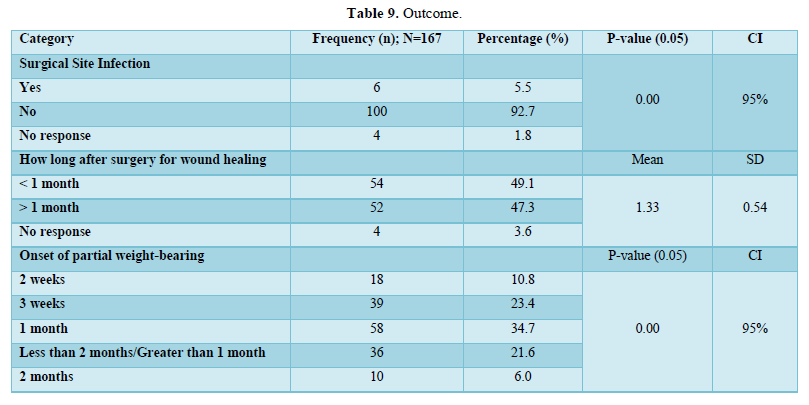
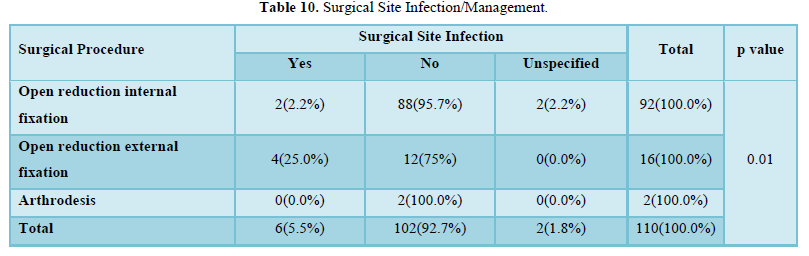
SSI is uncommon in this study. Cases of OREF show the highest postoperative SSI rate (25%). The p value for this correlation was 0.01, indicative of the statistical significance of the observed relationship between these 2 variables.
Diabetic patients that underwent surgery did not suffer from SSIs postoperatively; however the relationship between the variables was not statistically significant. Table 11 below shows the correlation between surgical management and wound healing time. Wound healing occurred within a month in 52(56.5%) of the ORIF cases, while the OREF and Arthrodesis cases needed over a month for wound to heal. The relationship of these variables is statistically significant (0.00) at a significance level of 0.05. Only 4 patients with a past history of Diabetes were managed operatively, ORIF for 2 and OREF for the other 2. All these cases the wound took longer than a month to heal however no statistical significance was found in this multivariate analysis. The obese patients in this study showed a wound healing pattern of 75% within a month, and 25% after a month and this association was statistically significant at 0.006(95% CI). These obese patients also did not suffer any SSIs postoperatively (p value 0.00).Partial weight-bearing was started most often at 1 month (58 cases, 34.7%), 03 weeks (39 cases, 23.4%) and between 1 month and 2 months (36 cases, 21.6%) following management, with mean of 4.8 weeks (SD 1.8). A cross-tabulation of definitive management and time to partial weight-bearing is shown in Table 12. The non-operative management options mostly began weight-bearing within a month of management, while cases managed operatively took longer to start weight-bearing. The relationship between these two variables is significant.
DISCUSSION
The study aimed to determine epidemiological characteristics, clinical and early postoperative outcome patterns of bimalleolar fracture patients at three centers in the Fako Division over 10 years spanning from 2010 to 2019.
Epidemiological Characteristics
The epidemiological data in this study showed a higher occurrence in males (92 cases, 55.1%) which is in line with the findings of several earlier studies done in Europe and the US [10,11], as well as the studies on the African continent [3,27]. However, the data is not in line with the trend of greater female predominance in the more recent studies by Thur [7] and Juto [9] in Europe. This could be explained by the higher incidence of road traffic accidents in Cameroon as well as the greater mobility of men relative to women compared to Europe [28,29]. The study showed the highest incidence in the 3rd and 4th decades, which mirrors the study by Ngunde [3], as well as a mean age of 37.3 years (±15.80) which is similar to the mean age of 33.3 years(16.04) seen in Ngunde [3] The age distribution and mean age is similar to the data by other studies on ankle fractures quoted.[4,7,11,12] Employment also proved to be a significant risk factor in the incidence of bimalleolar fractures, making up 60% of the cases in this study. This is expected as the active population engages in higher-risk circumstances than the dependent population, exposing themselves to such injuries more regularly.
Cause of Injury
The most common cause of injury was road traffic accidents in this study (78 cases, 46.8%), followed by falls and gunshot injuries. Studies by Sobgny [29] and Chichom [28] outline the high rate of RTAs in Cameroon relative to other parts of the world, while Ngunde [3] found pedestrians (26.52%) to be the most vulnerable to lower limb injuries as was seen in this study with pedestrians accounting for 27.5% of victims of bimalleolar fractures following a RTA [3]. The study by Kuubiere [27] in Tamale, Ghana found similar causes however RTAs accounted for a greater proportion of the ankle fractures (88.6%) than seen in this study. Ngunde [3] also found ankle fractures to account for almost a tenth of all lower limb fractures caused by road traffic accidents [3]. The studies in other parts of the world find falls the most incriminating, followed by road traffic accidents and sports, which was dissimilar to the causation distribution seen in this study [7-11].
Clinical Pattern
Symptoms of bimalleolar fractures are well documented and mirrored by the findings in this study. Most of the cases were closed fractures (133, 79.6%) which is the distribution seen in all ankle fracture studies, however the incidence of open fractures was significantly higher than the 1 to 3% incidence seen in the literature [7,9,11]. This is explained by the high impact cause of injury in this study, RTAs, compared to these studies in the West. The left-sided predominance is accounted for by the left side of vehicles being most vulnerable in road traffic accidents, which was the observed distribution in the study by Ngunde [3], as well as the study by Sakaki [30]. However, a right-sided predominance is more common in the literature [4,7,9,11].
Comorbidities investigated in this study were uncommon among the cases, however some statistically significant relationships were observed. The obese patients were found to have Type B and C bimalleolar fractures, which is similar to the study by Strauss [22] who found a higher severity of bimalleolar fractures in the obese compared to the non-obese patients. Obese patients were also not found to have worse early postoperative outcomes, which mirrors the study by Matson [33] which found a similar pattern. Diabetic patient correlations to outcome factors were not found to be statistically significant, indicating a need for more focused research as the literature shows Diabetes to be a significant risk factor for postoperative wound complications [19,20,31-46] The Weber Classification of these cases was available in 54 of the admission files. Transsyndesmotic (Type B) fractures made up 24 of the cases (44%), followed by infrasyndesmotic (Type A) 37.0% and lastly suprasyndesmotic fractures (Type C) 18.5%. Similar distribution was seen in the study by Court-Brown et al. with Type B making 52% of the cases in their study; Type A 38% and Type C 10% [11]. The analysis of dependence of type of fracture on mechanism of injury found no relationship between the two variables of statistical significance. While Type A fractures were mostly female (60%), Type C mostly male (80%) and Type B evenly distributed, the data was not statistically significant. Comparatively, the study by Juto [9] found a Weber Type A bimalleolar fractures to be mostly female (60.2%), Type B mostly female (60.1%) and Type C was more evenly distributed (48.7%).
Management
Management of bimalleolar fractures can either be operative or non-operative, with stability and displacement of the bony fragments being the main factors influencing the choice of management. In this study, 110 cases (65.9%) cases were managed operatively with Open Reduction Internal Fixation making up 55.1% of all management options undertaken. Open Reduction External Fixation (9.6%) was most often used in open fracture management while Arthrodesis was employed in 2 cases presenting with intractable ankle pain. Surgical management is most widely used in fracture management with a low threshold to choosing this option as studies have found better functional outcome following surgery relative to conservative management [47,48]. While operative management was employed most frequently, the data revealed a more conservative approach in this sub region as surgery rates are higher in other ankle fracture studies [4,7,48]. This could be explained by the paucity in orthopedic surgeons in the region and the middle to low-class socioeconomic status of these communities.
The Weber Classification system of bimalleolar fractures is based on the location of fracture relative to the ankle syndesmosis. The higher the level of the fracture, the more unstable the joint and hence a need for invasive reduction of the bony fragments. As such, Type B and C fractures were almost all managed operatively. Type A bimalleolar fractures were mainly managed non-operatively, bone fragment displacement a likely reason for the proportion managed operatively which radiographic material would have helped investigate but was unavailable in the files. This correlation between the classification and management employed is in line with the literature on bimalleolar fractures [2,4,11,13].
Outcome
This study was admission file-based, and it assessed the short-term outcomes by investigating surgical site infection, time to wound healing, and time to partial weight-bearing. Surgical site infection occurred in 5.5% of the cases surgical cases, which falls within the 3-8% range of SSIs found in the literature [49-53]. Open Reduction External Fixation was seen as an important factor in SSI cases, as one-quarter of the OREF cases suffered an SSI. Among the major indications for OREF are open fractures, malunion and infected fracture cases all of which increase the risks for SSI hence explaining this observation in this study. Similar patterns were seen with the wound healing as OREF cases took over a month for wound to heal, as expected with an external fixator(s) in place.
The comparative study by Niloofar between early weight-bearing at 2 weeks and late weight-bearing at 6 weeks following ORIF of ankle fracture cases found the early weight-bearing group to have significantly better functional outcome at the 6-week postoperative checkup relative to the late weight-bearing group, while Firoozabadi [54] found immediate weight-bearing to be of import in management of ankle fractures managed post-operatively.
Partial weight-bearing in this study occurred most frequently at the 1 month and 3 weeks following treatment with a mean of 4.7 weeks (±1.8) (p value 0.00, CI 95%). Operative management cases began weight-bearing between 4 weeks to 8 weeks postoperatively, while the non-operative group began sooner, in less than 4 weeks.
Strengths and Limitations
Strengths
- This study provides data on bimalleolar fractures in Cameroon. The study reveals the prevalence of bimalleolar fractures in the region as well as its hospitalization burden to the victims.
- The data outlines various factors relevant to bimalleolar fracture management and brings out dependence relationships and trends in its occurrence and management which could be used to improve management of future bimalleolar fracture cases in the region.
Limitations
- Some admission files were incompletely filled and reduced the sample size.
- The study has data on the hospital-based bimalleolar fractures while out-patient managed cases and patients managed by bone settlers in the region are not accounted for.
- The study was based on admission file data; hence longer-term outcome patterns could not be ascertained.
CONCLUSION
Bimalleolar fractures are trauma injuries with a male and active population predominance. As has been reported in several studies in Cameroon, road traffic accidents account for most of the bimalleolar fractures in this study [143,144].
Closed fractures were most prevalent, with a left-sided predominance observed. The left-sided predominance is expected with RTAs as the commonest cause of injury. Where Weber Classification was available, Type B fractures were the most prevalent followed by Type A and lastly Type C bimalleolar fractures.
Management of bimalleolar fractures, this study found, was mainly surgical and analysis revealed Weber Type B and C were almost entirely managed operatively while Type A fractures were mostly managed conservatively with cast placement or ankle splint application. Surgical Site Infections occurred in 5.5% of the cases and occurred most commonly in cases that underwent an OREF procedure. Wound healing patterns were similar to SSI patterns, with OREF cases taking longer to heal, while partial weight-bearing occurred most commonly between 3 weeks and 6 weeks following management with a mean time of 4 weeks 5 days.
RECOMMENDATIONS
Faculty of Health Sciences
The paucity of data on the topic in the Fako division is significant, given bimalleolar fractures occur frequently in our setting. There is a need for more studies to be carried out on the topic, for comparative purposes and to improve the data available on bimalleolar fractures in the region.
Health Facility
- Medical research hinges greatly on hospital records of admissions over the years with admission files being pivotal in future studies requiring retrospective analysis. It is vital relevant medical information be documented in the patient files, beginning with a history of the illness, clear outline of investigations and diagnosis, and in-hospital follow-up. We cannot overemphasize the necessity of filling admission files as this study suffered from a lack of radiological and classification information on these bimalleolar fractures files perused.
- The data from this study revealed time to partial weight-bearing in operative cases to be longer than the optimal time found in the literature for the management of ankle fractures. Beginning weight-bearing at 2 weeks postoperatively has been shown to yield better functional outcome than late weight-bearing regimes [55].
- Frakturregistret S (2016) This shows the data in the Fracture Register. Accessed on: July 23, 2020. Available online at: https://sfr.registercentrum.se/
- Court-Brown CM, Caesar B (2006) Epidemiology of adult fractures: A review. Injury 37(8): 691-697.
- Ngunde PJ, Akongnwi ACN, Mefire CA, Puis F, Gounou E, et al. (2019) Prevalence and pattern of lower extremity injuries due to road traffic crashes in Fako Division, Cameroon. Pan Afr Med J 32: 53.
- Elsoe R, Ostgaard SE, Larsen P (2018) Population-based epidemiology of 9767 ankle fractures. Foot Ankle Surg Off J Eur Soc Foot Ankle Surg 24(1): 34-39.
- Kannus P, Palvanen M, Niemi S, Parkkari J, Jrvinen M (2002) Increasing number and incidence of low-trauma ankle fractures in elderly people: Finnish statistics during 1970-2000 and projections for the future. Bone 31(3): 430-433.
- Somersalo A, Paloneva J, Kautiainen H, Lönnroos E, Heinänen M (2014) Incidence of fractures requiring inpatient care. Acta Orthop 85(5): 525-530.
- Thur CK, Edgren G, Jansson K-Å, Wretenberg P (2012) Epidemiology of adult ankle fractures in Sweden between 1987 and 2004. Acta Orthop 83(3): 276-281.
- Koval KJ, Lurie J, Zhou W, Sparks MB, Cantu RV, et al. (2005) Ankle Fractures in the Elderly: What You Get Depends on Where You Live and Who You See. J Orthop Trauma 19(9): 635-639.
- Juto H, Nilsson H, Morberg P (2018) Epidemiology of Adult Ankle Fractures: 1756 cases identified in Norrbotten County during 2009-2013 and classified according to AO/OTA. BMC Musculoskelet Disord 19(1): 441.
- Daly PJ, Fitzgerald RH, Melton LJ, Llstrup DM (1987) Epidemiology of ankle fractures in Rochester, Minnesota. Acta Orthop Scand 58(5): 539-544.
- Court-Brown CM, McBirnie J, Wilson G (1998) Adult ankle fractures-an increasing problem? Acta Orthop Scand 69(1): 43-47.
- Qureshi PAAA (2022) Weber classification of ankle fractures. Accessed on: August 10, 2020. Available online at: https://radiopaedia.org/articles/weber-classification-of-ankle-fractures
- Hsu RY, Bariteau J (2013) Management of ankle fractures. R I Med J 96(5): 23-27.
- Segal G, Elbaz A, Parsi A, Heller Z, Palmanovich E, et al. (2014) Clinical outcomes following ankle fracture: A cross-sectional observational study. J Foot Ankle Res 7(1): 50.
- Broos PL (1991) Bisschop AP. Operative treatment of ankle fractures in adults: Correlation between types of fracture and final results. Injury 22(5): 403-406.
- Lindsjö U (1985) Operative treatment of ankle fracture-dislocations. A follow-up study of 306/321 consecutive cases. Clin Orthop 199: 28-38.
- Hancock MJ, Herbert RD, Stewart M (2005) Prediction of outcome after ankle fracture. J Orthop Sports Phys Ther 35(12): 786-792.
- Egol KA, Tejwani NC, Walsh MG, Capla EL, Koval KJ (2006) Predictors of short-term functional outcome following ankle fracture surgery. J Bone Joint Surg Am 88(5): 974-979.
- Mohta M, Sethi AK, Tyagi A, Mohta A (2003) Psychological care in trauma patients. Injury 34(1): 17-25.
- Miller AG, Margules A, Raikin SM (2012) Risk factors for wound complications after ankle fracture surgery. J Bone Joint Surg Am 94(22): 2047-2052.
- King CM, Hamilton GA, Cobb M, Carpenter D, Ford LA (2012) Association between ankle fractures and obesity. J Foot Ankle Surg 51(5): 543-547.
- Strauss EJ, Frank JB, Walsh M, Koval KJ, Egol KA (2007) Does obesity influence the outcome after the operative treatment of ankle fractures? J Bone Joint Surg Br 89-B(6): 794-798.
- Matson AP, Morwood MP, Peres Da Silva A, Cone EB, Hurwitz SR, et al. (2017) Obese Patients Have Fewer Wound Complications Following Fixation of Ankle Fractures. Foot Ankle Spec 10(5): 435-440.
- Nåsell H, Ottosson C, Törnqvist H, Lindé J, Ponzer S (2011) The impact of smoking on complications after operatively treated ankle fractures-a follow-up study of 906 patients. J Orthop Trauma 25(12): 748-755.
- Marley W, Kelly G, Thompson N (2015) Alcohol-Related Fracture Admissions: A Retrospective Observational Study. Ulster Med J 84(2): 94-97.
- Huang ES, Basu A, O’Grady M, Capretta JC (2009) Projecting the future diabetes population size and related costs for the U.S. Diabetes Care 32(12): 2225-2229.
- Kuubiere CB, Alhassan A, Majeed SF (2012) Management of complex ankle fracture: A Ghanaian experience. J Med Biomed Sci 1(4): 1-6.
- Chichom-Mefire A, Palle-Ngunde J, Fokam PG, Mokom-Awa A, Njock R, et al. (2018) Injury patterns in road traffic victims comparing road user categories: Analysis of 811 consecutive cases in the emergency department of a level I institution in a low-income country. Int J Surg Open 10: 30-36.
- Sobngwi J, Bhatti J, Kounga G, Salmi L-R, Lagarde E (2010) Road traffic crashes on the Yaounde-Douala road section, Cameroon. Accid Anal Prev 42: 422-426.
- Sakaki MH, Matsumura BAR, Dotta TDAG, Pontin PA, dos Santos ALG, et al. (2014) Epidemiologic study of ankle fractures in a tertiary hospital. Acta Ortop Bras 22(2): 90-93.
- Ganesh SP, Pietrobon R, Cecílio WAC, Pan D, Lightdale N, et al. (2005) The impact of diabetes on patient outcomes after ankle fracture. J Bone Joint Surg Am 87(8): 1712-1718.
- Chaudhry S, Egol KA (2011) Ankle injuries and fractures in the obese patient. Orthop Clin North Am 42(1): 45-53.
- Guss D, Bhattacharyya T (2006) Perioperative Management of the Obese Orthopedic Patient. J Am Acad Orthop Surg 14(7): 425-432.
- Mendelsohn ES, Hoshino CM, Harris TG, Zinar DM (2013) The Effect of Obesity on Early Failure After Operative Syndesmosis Injuries. J Orthop Trauma 27(4): 201-206.
- Koval K, Zhou W, Sparks M, Cantu R, Hecht P, et al. (2007) Complications after Ankle Fracture in Elderly Patients. Foot Ankle Int 28: 1249-1255.
- Strauss EJ, Egol KA (2007) The management of ankle fractures in the elderly. Injury 3: S2-S9.
- Shivarathre D, Chandran P, Platt S (2011) Operative Fixation of Unstable Ankle Fractures in Patients Aged Over 80 Years. Foot Ankle Int 32: 599-602.
- Lynde MJ, Sautter T, Hamilton GA, Schuberth JM (2012) Complications after open reduction and internal fixation of ankle fractures in the elderly. Foot Ankle Surg 18(2): 103-107.
- Olsen JR, Hunter J, Baumhauer JF (2013) Osteoporotic Ankle Fractures. Orthop Clin North Am 44(2): 225-241.
- McKean J, Cuellar DO, Hak D, Mauffrey C (2013) Osteoporotic ankle fractures: An approach to operative management. Orthopedics 36(12): 936-940.
- Zaghloul A, Haddad B, Barksfield R, Davis B (2014) Early complications of surgery in operative treatment of ankle fractures in those over 60: A review of 186 cases. Injury 45(4): 780-783.
- Kettunen J, Kröger H (2005) Surgical treatment of ankle and foot fractures in the elderly. Osteoporos Int 2: S103-S106.
- Valtola A, Honkanen R, Kröger H, Tuppurainen M, Saarikoski S, et al. (2002) Lifestyle and other factors predict ankle fractures in perimenopausal women: A population-based prospective cohort study. Bone 30: 238-242.
- Hasselman CT, Vogt MT, Stone KL, Cauley JA, Conti SF (2003) Conti SF. Foot and ankle fractures in elderly white women. Incidence and risk factors. J Bone Joint Surg Am 85(5): 820-824.
- Pritchard JM, Giangregorio LM, Ioannidis G, Papaioannou A, Adachi JD, et al. (2012) Ankle fractures do not predict osteoporotic fractures in women with or without diabetes. Osteoporos Int 23(3): 957-962.
- Thordarson DB (2000) Complications After Treatment of Tibial Pilon Fractures: Prevention and Management Strategies. J Am Acad Orthop Surg 8(4): 253-265.
- Harper MC (1991) The lateral ligamentous support of the subtalar joint. Foot Ankle 11(6): 354-358.
- Ovaska M (2015) Complications in ankle fracture surgery. Acta Orthop 86(sup358): 1-35.
- Harager K, Hviid K, Jensen CM, Schantz K (2000) Successful immediate weight-bearing of internal fixated ankle fractures in a general population. J Orthop Sci 5(6): 552-554.
- Srinivasan CM, Moran CG (2001) Internal fixation of ankle fractures in the very elderly. Injury 32(7): 559-563.
- Roberts RS (1983) Surgical treatment of displaced ankle fractures. Clin Orthop 172: 164-170.
- Makwana NK, Bhowal B, Harper WM, Hui AW (2001) Conservative versus operative treatment for displaced ankle fractures in patients over 55 years of age. A prospective, randomized study. J Bone Joint Surg Br 83(4): 525-529.
- Thangarajah T, Prasad PSV, Narayan B (2009) Surgical Site Infections Following Open Reduction and Internal Fixation of Ankle Fractures. Open Orthop J 3: 56-60.
- Firoozabadi R, Harnden E, Krieg JC (2015) Immediate Weight-Bearing after Ankle Fracture Fixation. Adv Orthop 2015: 491976.
- Dehghan N, McKee MD, Jenkinson RJ, Schemitsch EH, Stas V, et al. (2016) Early Weightbearing and Range of Motion Versus Non-Weightbearing and Immobilization After Open Reduction and Internal Fixation of Unstable Ankle Fractures: A Randomized Controlled Trial. J Orthop Trauma 30(7): 345-352.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6
-
Table 7
-
Table 8
-
Table 9
-
Table 10
-
Table 11
-
Table 12

















