
60
Views & Citations10
Likes & Shares
Conclusion: This case illustrates the clinical value of Hoagland Sign in early identification of EBV. Awareness of this underrecognized sign may facilitate prompt diagnosis and appropriate management of infectious mononucleosis.
CASE REPORT
A 21-year-old female with no known comorbidities presented with a 7-day history of high-grade fever, bifrontal headache, and bilateral periorbital swelling, which was more pronounced in the mornings. There was no history of rash, breathlessness, or allergic reactions. Two weeks prior, she had experienced neck pain followed by localized pruritus, which subsided with antihistamines. She also had a history of recurrent oral ulcers.
Previously, she was evaluated at a local hospital where a non-contrast CT brain showed right-sided deviated nasal septum (DNS) and a left maxillary sinus polyp. As symptoms persisted, she was referred for further evaluation.
On examination, she was febrile (101.2°F), with mild pallor, bilateral periorbital edema (Figure 1), bilateral tonsillar enlargement with exudates, posterior cervical lymphadenopathy, and signs of bilateral dacryoadenitis. Respiratory examination revealed decreased breath sounds on the right.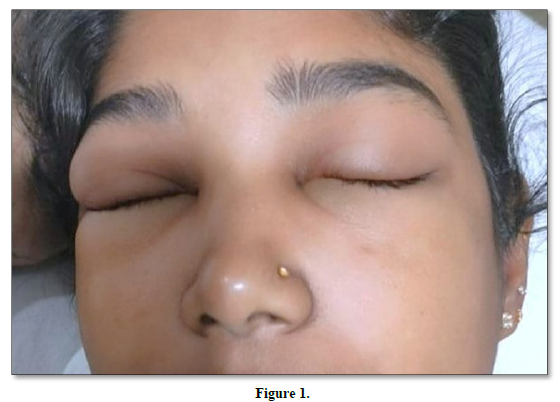
Blood tests showed normocytic anemia, leukocytosis, thrombocytopenia, and mildly elevated inflammatory markers. Liver function tests indicated mild transaminitis and hyperbilirubinemia. Peripheral smear revealed dimorphic anemia and reactive lymphocytosis. Widal test was negative. Ophthalmology consultation confirmed bilateral dacryoadenitis. EBV IgM serology was positive.
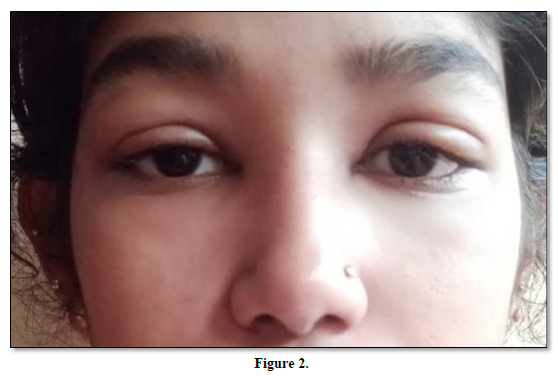
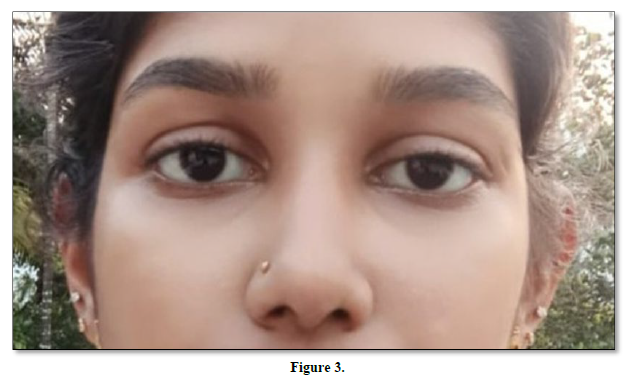
The patient was managed with intravenous corticosteroids and supportive measures, including topical eye drops. Her symptoms gradually improved, with resolution of fever and periorbital swelling (Figures 2 & 3). She was discharged in a stable condition with outpatient follow-up.
DISCUSSION
Hoagland Sign refers to bilateral periorbital edema observed in EBV infections and is considered an early manifestation of infectious mononucleosis. It likely results from lymphatic obstruction or inflammation of the lacrimal glands [2,3]. This presentation can easily be misdiagnosed as an allergic or bacterial condition, delaying appropriate management.
Dacryoadenitis is a rare but recognized feature of EBV infection and typically presents bilaterally, in contrast to the unilateral involvement seen in bacterial causes [4]. Ophthalmological examination in our case supported this diagnosis.
Although corticosteroids are not routinely indicated in uncomplicated IMN, their use in cases with significant ocular inflammation or airway compromise is documented and may accelerate recovery [5].
Early recognition of Hoagland Sign can streamline diagnostic evaluation, minimize unnecessary antibiotic use, and avoid excessive investigations. In our patient, the correct diagnosis led to a favorable outcome with conservative management.
- Hoagland RJ (1952) The clinical manifestations of infectious mononucleosis: A report of two hundred cases. Am J Med Sci 223(4): 469-482.
- Balfour HH Jr, Dunmire SK, Hogquist KA (2015) Infectious mononucleosis. Clin Transl Immunol 4(2): e33.
- Grotto I, Mimouni D, Huerta M, Mimouni M, Cohen D, et al. (2003) Clinical and laboratory presentation of EBV-positive vs EBV-negative patients with suspected infectious mononucleosis. Scand J Infect Dis.35(5): 354-357.
- Deaño J, González-López JJ (2014) Dacryoadenitis as the first manifestation of Epstein-Barr virus infection in young adults. Ocul Immunol Inflamm 22(5): 393-395.
- Pavan-Langston D (2005) Viral diseases of the eye. In: Foster CS, Azar DT, Dohlman CH, eds. Smolin and Thoft's The Cornea: Scientific Foundations and Clinical Practice. 4th Philadelphia: Lippincott Williams & Wilkins.



QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- International Journal of Diabetes (ISSN: 2644-3031)
- Journal of Pathology and Toxicology Research
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)


