
3566
Views & Citations2566
Likes & Shares
Diphtheria is a highly contagious vaccine-preventable disease caused mainly by the bacteria Corynebacterium diphtheriae which can be fatal in 5-10% of cases, with a higher mortality rate in young children [2]. It is spread by airborne respiratory droplets [4]. Corynebacterium diphtheriae is a non-spore-forming, non-encapsulated, non-motile, Gram-positive bacillus which produces an exotoxin. It commonly affects the nasal cavities, oropharynx and larynx causing necrosis of tissues and formation of pseudo membranes which lead to respiratory obstruction. Dissemination of the toxins in the blood can cause other complications such as septicemia, disseminated intravascular coagulopathy, myocarditis, heart failure, renal failure and death. Corynebacterium ulcers causes cutaneous disease.
This highly contagious disease has made a strong showing in Nigeria since November last year [1]. Statistics have shown as of August 31st 2023 a total of 5898 suspected cases were reported from 59 LGAs in 11 states across the country, with Kano state carrying a majority of the cases. Other states that reported significant numbers included Katsina, Borno, Bauchi, Kaduna, and Yobe. Of the cumulative 8353 suspected cases reported since the outbreak was first reported in 2022, 4717 cases were confirmed (lab confirmed (169), epidemiologically linked (117) and clinical compatibility (4431).
Authorities have raised concerns due to the current re-emergence of diphtheria in the country [1]. Considering diphtheria is vaccine preventable the rising reported numbers is alarming. WHO [5] has stated that the prevalence of diphtheria suggests inadequate coverage of national childhood immunization programs. Nigeria has experienced a low to moderate coverage of vaccination since its inception. The country currently faces an upsurge in vaccine preventable diseases [6]. The WHO [2] has reported low national coverage of about 57% of the pentavalent vaccine (Penta 3). They further reported the pediatric population to have a majority of the sub-optimal vaccination.
Though multiple interventions have been postulated and many policies implemented. There has still been reports of rising numbers of suspected cases of diphtheria [6]. Since epidemiological studies have shown a clustering of cases in the northern part of the country with Kano state being the focal point, causative factors may suggest sociocultural factors [1]. Authorities have suggested the 2003 vaccine boycott that was precipitated by politicians and religious leaders and is still being promoted widely across the northern part of the country to be the major reason for vaccine hesitancy [4]. To mitigate future outbreaks identification of the main immunization barrier and how to effectively curtail it, must be identified. This study will aim to assess the factors responsible for poor immunization coverage in northern Nigeria.
SCOPE OF THE STUDY
This study will concentrate on caregivers of patients of with a history of suspected diphtheria cases in four states in northern Nigeria.
OBJECTIVES
• To assess the factors responsible for low immunization coverage in northern Nigeria
• To assess the possible barriers to immunization in northern Nigeria
• To assess the limitations to immunization in northern Nigeria
LIMITATIONS OF THE STUDY
This study will be limited to care givers patients of suspected diphtheria cases across four northern states.
METHODOLOGY
This study adopted a descriptive cross-sectional study design with a purposive sampling technique. Whereby interviews were conducted with caregivers of suspected and confirmed diphtheria patients as well as health care workers posted to health facilities in the hot spot areas.
CASE REPORT
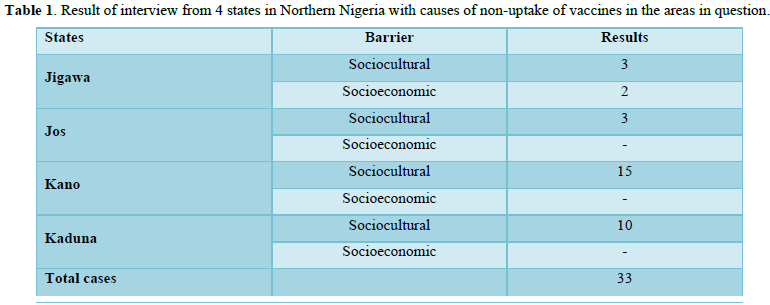
A total of 33 suspected cases were assessed across four states by caregiver interview conducted by health worker. A suspected case was defined as a presentation where a child under the age of 14 presented with acute sore throat, difficulty in breathing, elevated temperature, swelling of the sub-mandibular region of the neck and general malaise. Cases assessed mostly died before confirmation of diagnosis. Responses were classified under socioeconomic and socio-cultural barriers (Figure 1).

The above child died 3 days later.
The table below (Table 1) shows result of interview from 4 states in Northern Nigeria. The interview revealed two major causes of non-uptake of vaccines in the areas in question.
RESULTS
The assessment revealed all cases to be situated in rural areas with low income and education as a common denominator. Most caregivers had not even attended western primary education. Those that had some level of education had strong sociocultural barriers to vaccination. Most of these sociocultural barriers included religious misconceptions and rank distrust in governmental structures due to rife corruption (Figure 2).

The above exhibit shows the rural areas of one of the suspected diphtheria cases.
As evidence above all were from low socioeconomic backgrounds with little to no formal education and a high dependence on their local religious leaders and chiefs. With the exception of 2 cases in Jigawa, a lack of resources or inaccessibility to primary health facilities wasn’t the major reason for vaccine hesitancy but rather a distrust in the government and disbelief in the existence of the disease (Figure 3).

At the above facility, none of the assessed cases reported to the health facility are reported on time. Even when they report to the rural facilities as seen in the above exhibit, the facilities are poorly maintained and ill equipped to handle diagnose and treat such cases.
Most cases reported to health facilities after worsening of symptoms with acute dyspnea and advent of bull neck. By the time cases had reported for effective management complications such as acute renal injury, airway obstruction, epistaxis and bleeding diathesis had developed with the death rate being about 83%. A resultant 17% still have ongoing infection as at the time of this report.
DISCUSSION
Diphtheria is known as a childhood disease, most common in children below 15 years, but with waning immunity and increase in unvaccinated individuals in countries with low diphtheria prevalence has resulted in an increase in case detection among people above 40 years [7]. Nigeria like most countries has adopted the vaccination Program named EPI (expanded program on immunization), with diphtheria among the DTP (Diphtheria, Tetanus and Pertussis) combination administered to infants at 6, 10 and 14 weeks of age [8].
The high numbers of diphtheria outbreak in northern Nigeria is a direct consequence of poor vaccine uptake [8]. The refusal of vaccine uptake is termed vaccine hesitancy. Vaccine hesitancy has been a major problem in northern Nigeria [9]. This hesitancy has been traced to a myriad number of reasons: distrust in government policies due to high levels of corruption and government inefficiencies has been a major driving force in vaccine hesitancy in Nigeria [10]. The inability of government to provide safety nets during perceived out breaks has resulted in a rank distrust by the populace [11]. The perception of low to no outbreak of diphtheria and other fatal vaccine preventable childhood diseases has been another major driver of vaccine hesitancy in northern Nigeria [9]. Other authorizes have reported the strong influence of religion in creating barriers to vaccine acceptance [12]. These reasons were found to resonate with the population assessed. Lack of trust in even the health facilities resulted in a delay of patients reporting to hospitals on time or only when complications have already developed.
Another important factor to the high numbers of this particular outbreak could be the lack of well-trained staff in the rural health facilities. The recurrence of diphtheria outbreaks is dependent on the ability of the healthcare services to meet the health needs of these communities. A weak health care system has a direct relationship with disease outbreaks [1,13]. Effective disease surveillance and reporting systems are crucial for early detection and containment of diphtheria outbreaks, however Nigeria’s surveillance systems are suboptimal at best [13-15]. Ensuring diseases are caught and contained early is highly dependent on adequate monitoring systems and well-trained staff employed in high risk rural areas.
CONCLUSION
Nigeria, a country with a large foreign debt and a struggling economic system, is ill equipped to tackle the constant advent of highly fatal communicable disease outbreaks. In the face of scare resources, the need to mitigate such preventable diseases is of paramount importance. To ensure population compliance a strong effort must be made by government to instill community trust and acceptance of government health policies.
RECOMMENDATIONS
A mindset change needs to be accomplished by engaging local religious leaders and community leaders. No matter how many facilities are put in place if the community are unwilling to access these facilities the facilities will not have the desired impact. Hence, raising awareness using the persons the communities listen to will go much farther in curbing this outbreak than any intervention previously proposed.
The government should also commit to improving the state of rural health care facilities and employment of skillfully trained staff to manage disease outbreaks. Moreover, rural outreach should be made to improve public confidence in government will to improve healthcare of the communities.
- Aradi G (2023) Nigeria diphtheria outbreak kills 600. Available online at: https://www.bbc.com/news/world-africa-67086849
- WHO (2023) Diphtheria-Nigeria. Available online at: https://www.who.int/emergencies/disease-outbreak-news/item/2023-DON485
- Abubakar MY, Lawal J, Dadi H, Grema US (2020) Diphtheria: A re-emerging public health challenge. Int J Otorhinolaryngol Head Neck Surg 6: 191-193.
- Sadoh AE, Oladokun RE (2012) Re-emergence of diphtheria and pertussis: Implications for Nigeria. Vaccine 30(50): 7221-7228.
- WHO (2006) Position Paper-Diphtheria. Available online at: https://www.who.int/publications/m/item/wer8103-diphteria-position-pager
- Nnaemeka VC, Okafor NA, Orababar OQ, Anikwe R (2023) COVID-19 vaccine acceptance in Nigeria: A rapid systematic review and abstract. pp: 48.
- Medugu N, Musa-Booth TO, Adegboro B, Onipede AO, Babazhitsu M, et al. (2023) A review of the current diphtheria outbreaks. Afr J Clin Exp Microbiol 2: 120-129.
- Oluloja NO, Anjorin ET, Ekerin O, Afolabi OT, Inuoja JM (2023) A looming epidemic: Combating the recurrent outbreaks of diphtheria in Nigeria. Pan Afr Med J 45: 186.
- Dube E, Larberge C, Guay M, Bramadat P, Roy R, et al. (2013) Vaccine Hesitancy: An overview. Hum Vaccin Immunother 9(8): 1763-1773.
- Ikwuka DC, Akintan P, Ogunbosi BO, Alao MA, Ibrahim OR, et al. (2022) COVID-19 vaccine hesitancy in six geopolitical zones in Nigeria: A cross-sectional survey. Pan Afr Med J 42: 179.
- Lucia S, Vincent S (2021) COVID-19 vaccine hesitancy report 2021.
- Volet AK, Scavone C, Matamoros DC, Capuano A (2022) Vaccine hesitancy among religious groups: Reasons underlying this phenomenon and communication strategies to rebuild trust. Front Public Health 10: 824560.
- Omoleke II, Taleat BA (2017) Contemporary issues and challenges of health sector in Nigeria. Res J Health Sci 5(4): 210-216.
- Grundy J, Biggs BA (2019) The Impact of Conflict on Immunization Coverage in 16 Countries. Int J Health Policy Manag 8(4): 211-221.
- Sato R, Fintan B (2020) Fear, knowledge, and vaccination behaviors among women in Northern Nigeria. Hum Vaccin Immunother 16(10): 2438-2448.
-
 Table 1
Table 1




QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- BioMed Research Journal (ISSN:2578-8892)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)


