Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)

Research Article
Patterns of Myocardial Tissue Doppler in Intrauterine Growth Restriction
4196
Views & Citations3196
Likes & Shares
Introduction: One of the consequences of IUGR is the development of cardiac diastolic dysfunction in fetuses. Tissue Doppler in echocardiography is a new technique to detect myocardial tissue function and can act as a useful tool in the identification of this complication. We undertake this study to see the different inferences of this investigative tool in Intrauterine growth restriction.
Objectives: The objective of the study was to carry out Myocardial tissue Doppler in fetuses with intrauterine growth restriction and observe the different inferences.
Design: It was a prospective case control study.
Population: Patients in the third trimester of pregnancy.
Methods: Fetal cardiac function was evaluated with the help of Myocardial Tissue Doppler in IUGR fetuses.
Main Outcome measures: Right and Left Ventricular and Interventricular septal E’, A’, E’/A’ and Myocardial performance index (MPI’).
Results: There were sixty-two IUGR fetuses in the study. Comparison with fifty-eight normal growth fetuses showed lower Right Ventricular late diastolic velocity (A’) in the former in significant measure.
Twenty-seven among the IUGR fetuses also had abnormal vessel Doppler. They did not show any significant difference in their Myocardial tissue Doppler parameters from the rest thirty-five with normal vessel Doppler.
Based on the birth weight of the IUGR fetuses on follow up, they were divided into mild, moderate and severe degree of IUGR. Twelve fetuses with severe IUGR were found to have significantly lower Right Myocardial performance Index and left ventricular early diastolic velocity (E’) than normal fetuses. Twenty-eight fetuses with moderate IUGR had lower but statistically insignificant parameters while the rest twenty-two mild IUGR fetuses showed lower left and right ventricular A’.
Conclusion: Myocardial tissue Doppler shows subtle cardiac dysfunction in IUGR babies in comparison to normal growth babies in the right ventricle particularly in babies with severe IUGR. Further research is needed to ascertain its utility in diagnosing cardiac dysfunction and perinatal complications in IUGR.
Keywords: Cardiac dysfunction, IUGR, Myocardial tissue Doppler
INTRODUCTION
Intrauterine growth restriction (IUGR) contributes to about 30% of perinatal loss and severe neonatal morbidity. Defined in scientific terms as fetal weight below the 10th percentile of the range for the particular gestational age, in more specific terms, it is the inability of the fetus to achieve its full growth potential for its particular genetic capacity. Although the immediate effect of disturbed fetal growth is manifested as a low birth weight, some of its long-term outcomes leave far reaching consequences of the underlying condition like placental dysfunction or aneuploidies. This makes the management of the condition and delivery of the fetus at the correct time highly imperative [1].
Several studies have proved the effect of the pathological process of placental dysfunction in IUGR on the fetal heart [2-5]. Fetal cardiac function is complex and depends on myocardial contractility as well as on extra-cardiac factors such as developmental maturation, loading conditions and fetal disease. As the fetus is increasingly jeopardized, signs of cardiovascular dysfunction appear.
There is decreased left ventricle afterload due to cerebral vasodilatation and an increased right ventricle afterload due to systemic and pulmonary vasoconstriction all in an attempt to preferentially shift the cardiac output in favor of left ventricle to increase perfusion of the brain. With progressive prolonged hypoxia there is deterioration of this adaptive effect with impaired cardiac filling and drop in cardiac function [6,7]. An increase of reverse flow in inferior vena cava occurs with atrial contraction suggesting high pressure gradient in right atrium. This reversed flow extends to the ductus venosus which ultimately causes reduction of end diastolic velocity in the umbilical vein seen as end-diastolic pulsations. These pulsations are frequently associated with acidemia and endocrine changes. By this stage, Ventricular ejection fraction is found reduced in both ventricles. That this happens in ventricles with diametrically opposite hemodynamic conditions supports the hypothesis that intrinsic myocardial function also deteriorates with prolonged adaptive mechanisms of IUGR.
Tissue Doppler in echocardiography is a new technique to detect myocardial tissue function. It has already proved its usefulness in children and adults for the same purpose and it is postulated that it can act as a useful tool in the fetuses as well [8].
Myocardial tissue Doppler ultrasonography is a technique that allows measurement of myocardial velocimetry in systole and diastole without the limitations of transvalvular mitral and tricuspid flow analysis which is influenced by a high cardiac rate and afterload conditions. The technique constitutes processing and analyzing the Doppler frequency shift generated by Tissue movement.
Recently the feasibility of tissue Doppler for fetal cardiac assessment has been reported [9-11]. As the cardiovascular changes in IUGR with progressive deterioration of intracardiac perfusion and consequent dysfunction tend to occur sometime before the signs of fetal distress appear on biophysical tests, the technique can detect cardiac dysfunction and may prove to be of valuable help in deciding on the management of fetuses with growth restriction. Studies done so far postulate that tissue Doppler could constitute a sensitive investigative tool in fetuses with IUGR [12-16]. We undertake the present study to see the different inferences of Myocardial tissue Doppler when carried out in IUGR fetuses.
METHODS
The study was a prospective observational study, carried out in a tertiary care hospital over a period of three years. Patients in the third trimester of pregnancy identified to be having intrauterine growth restriction-through ultrasound examination (using the Haddock’s formula to calculate the estimated fetal weight and plotting of charts) were included. The fetuses whose growth curve were below the 10th percentile or showed a fall in the expected growth curve were taken for the study. The growth curves were plotted with standardized custom-made charts used in the hospital for the diagnosis and management of fetal growth restriction. Written and informed consent was obtained from all patients.
All patients were imaged with the Sonoline Adara machine with available frequency of 3.5 MHz and growth curves of the fetuses were plotted with the help of specialized Sonocare software. Fetuses whose growth curve showed a falling trend or persistently remained along the 10th percentile of the curves were taken as the study group. The fetuses with growth curves with normal trend were included in the control group.
Exclusion criteria were patients with multiple gestation and fetuses with cardiac anomalies.
Fetal echocardiography was done along with myocardial tissue Doppler in all these patients with help of Vivid GE machine. Sampling was done at the level of the basal part of the left ventricular free wall, right ventricular wall and interventricular septum. Spectral Tissue Doppler imaging was performed on both groups of fetuses in view of the various limitations of Color Doppler [16].
The variables of tissue Doppler taken for all the three areas were [17]:
- E’-the mean peak value of three early diastolic waves, A’-the mean value of three late diastolic or atrial filling waves, E’/A’-The ratio between the two,
- Myocardial performance index (MPI’) - Calculated by the formula ICT’+IRT’/ET’ where:
- ICT’ - isovolumetric contraction time,
- ET’ - ejection time
- IRT’ -isovolumetric relaxation time.
Conventional Vessel Doppler examination was also done for all of these patients. The variables obtained by myocardial tissue Doppler were compared between the study and control group. Statistical analysis was done with the help of SPSS software 16.
RESULTS
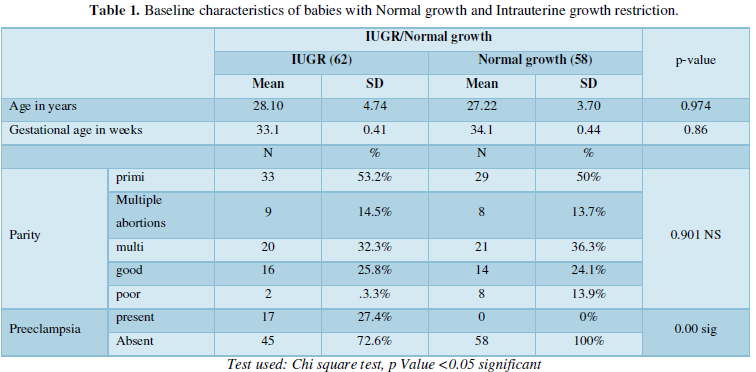
Sixty-two patients with IUGR defined as fetal weight less than the 10th percentile and Fifty-eight with growth appropriate for gestation. None of the demographic parameters show any statistical significance among the two groups save for preeclampsia. This is understandable as preeclampsia is an important risk factor for development of intrauterine growth restriction [18] (Table 1). The average gestational age at which the test was conducted was 33.1+/-0.41 weeks in IUGR babies and 34.1+/-0.44 weeks in Normal growth babies with no statistical significance between the two hence gestational age as a confounding factor is ruled out.
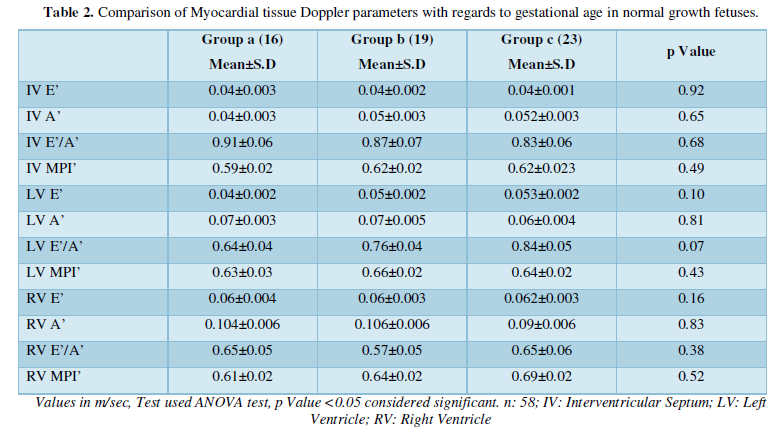
To further look for any variation in cardiac function with increasing gestational age, the normal growth babies were divided into three groups based on the gestational age at which fetal echocardiography was performed at intervals of four weeks. Groups based on gestational age at the time of test:
- Test between 28-32 weeks-16
- Test between 32 -34 weeks-19
- Test between 34-36 weeks-23
Using the ANOVA test on account of presence of three groups, no significant difference was found among the mean values of all the parameters among the three groups statistically. The Myocardial tissue Doppler parameters did not show any significant difference between the variables with increasing gestational age or any increasing or decreasing trend of the parameters with gestational age showing constant cardiac function throughout the third trimester (Table 2).
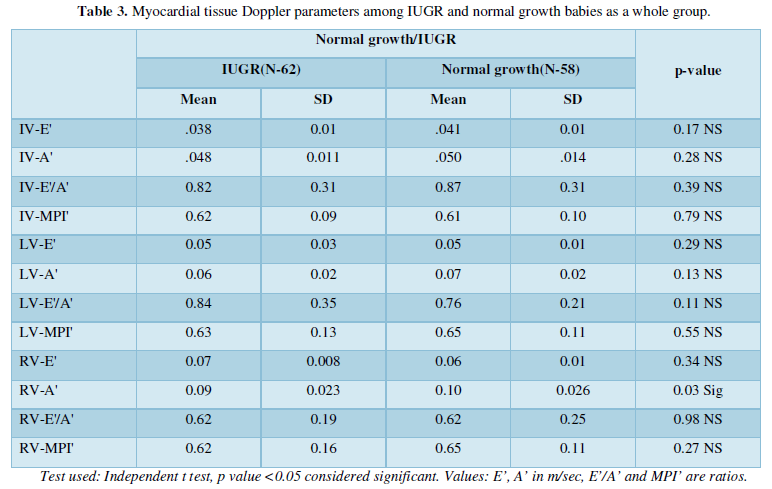
The Myocardial tissue Doppler parameters of the two groups of IUGR and normal growth babies were compared using the independent t-test (Table 3). All the parameters of IUGR babies were found to be lower than the ones with normal growth. This however was found statistically significant only for the right ventricle A’. Atrial contraction velocity at the level of right ventricle is hence lower in IUGR babies indicating diastolic dysfunction in them.
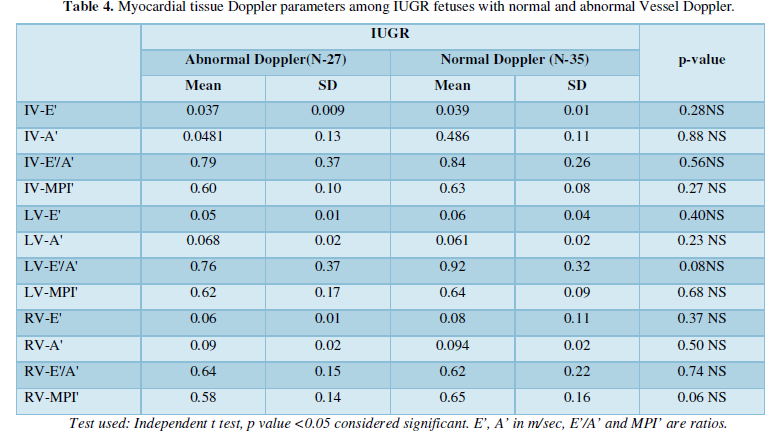
Both the groups were also subjected to conventional vessel Doppler which is regarded the standard test to look for uteroplacental insufficiency. Abnormalities of severe degree are indicative of impending adverse outcomes and an indication for delivery. All the babies with normal growth had normal conventional vessel Doppler. Among the babies with IUGR, twenty-seven had abnormal vessel Doppler (defined as raised umbilical artery indices, absent or reversed end diastolic flow) while thirty-five had normal vessel Doppler.
The two groups of IUGR fetuses so formed based on conventional vessel Doppler were compared between each other. The tissue Doppler parameters were lesser in the IUGR babies with abnormal vessel Doppler than the ones with normal. None of them were however statistically significant. This indicates that Myocardial tissue Doppler is not able to differentiate between the babies requiring more particular attention as defined by conventional Vessel Doppler (Table 4).
The babies with IUGR were classified on the basis of severity which was assessed based on the birth weight. This was done as:
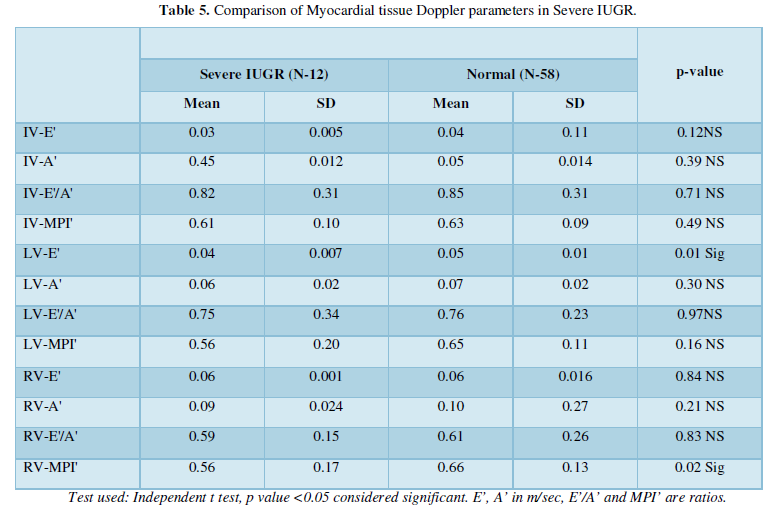
- Severe IUGR-(Birth weight < 1.5 kg)-12 in present study
- Moderate IUGR-(Birthweight-1.5 -2 kg)-28 in present study
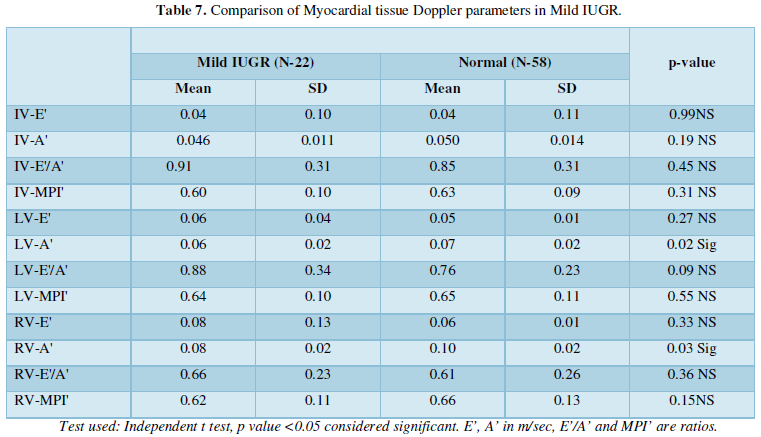
- Mild IUGR-(Birth weight-2-2.5 kg)-22 in present study
On comparing the myocardial tissue parameters between babies with severe IUGR and normal growth babies, all were found lesser than the normal growth babies (Table 5). Statistically significant however were the right ventricular parameter MPI’ as well as left ventricular E’. This indicates dysfunction of both ventricles with increased severity of cerebroplacental insufficiency.
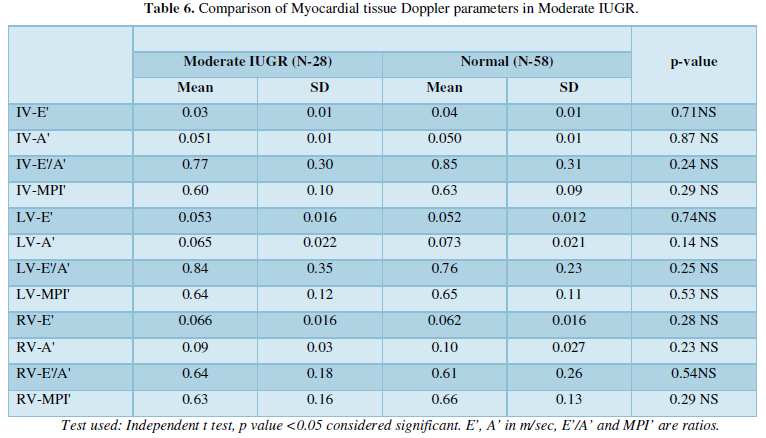
The comparison when made between moderate IUGR and normal growth babies showed reduced parameters in the former but none of which were statistically significant indicating probable cardiac compensation in babies with Moderate IUGR (Table 6).
On Comparison between babies with mild IUGR and Normal growth, both the right and left ventricular A’ were found significantly reduced in IUGR babies among all the parameters (Table 7).
DISCUSSION
It was a prospective observational study conducted to assess the ability of Myocardial tissue Doppler to detect cardiac dysfunction and predict perinatal outcome in IUGR. One hundred and twenty patients were taken among which sixty-two were IUGR and fifty-eight were fetuses with normal growth.
Myocardial tissue Doppler was used for the study which uses the high amplitude and low frequency signals generated by the myocardial tissue while movement during the cardiac cycle giving an impartial view of the actual functioning of the different ventricles of the heart without being biased by the load conditions [8]. In adults this technique has been used for assessing cardiac systolic and diastolic functions. These assessments can be performed by measuring myocardial velocity, myocardial velocity gradient, myocardial strain and strain rate. Strain implies the differential velocities in the cardiac wall and does not reflect overall movement of the heart. This can enable us to identify if there is actual cardiac dysfunction or just altered functioning as a compensation to tide over unfavorable circulatory changes. Whether it can be used as successfully in the fetal period remains to be seen.
Dating forms an important consideration in the diagnosis of intrauterine growth restriction. Many babies are wrongly diagnosed to have IUGR when actually they may be normal for the actual period of gestation. In our data, most of the patients had excellent or good dating, so it can be reliably said that no patient was falsely categorized into either group.
Parity is not a risk factor for the development of growth restriction and our cases show statistically insignificant distribution among primigravidas, multigravidas and patients with multiple abortions.
Preeclampsia is a major risk factor for development of intrauterine growth restriction and nearly 30% of our cases had preeclampsia also [18]. No other maternal or fetal comorbidity was found in a significant measure.
All measurements were made on the same machine and were carried out by the same trained person on both the study and control groups. Hence the chances of interobserver variations and the problems of expertise and knowledge in carrying out this test were nullified.
The parameters obtained for all normal growth babies were compared amongst each other and no significant increasing or decreasing trends were seen with increasing gestational age. Paladini [10] found that all variables except for end diastolic subepicardial velocities showed a positive correlation with gestational age while the ratio of E’/A’ remained constant. Similarly, Elmstedt [19] with the application of tissue Doppler imaging in fetuses concluded fetal myocardial contractility decreased with gestational age. However, both studies have taken subjects from 17-18 to 37-42 weeks while all our subjects are in the third trimester.
Our results indicate no change in tissue function with increasing proximity to term excluding gestational age as a factor influencing our results.
On comparison of the Myocardial tissue Doppler parameters in all the babies with IUGR and babies with normal growth, it was found that all the variables were lower in the former. This is suggestive of an overall reduction in the level of effective cardiac function in babies with IUGR. The parameter significantly reduced was Right ventricular A’ which is dependent on the force of atrial contraction. With increasing gestational age, the dependence of ventricular filling on the atrial contraction wave reduces. The finding of the study shows a persistence of the same in IUGR babies. It also shows that the right atrium is the first area to be affected with the increasing hypoxia of the placental insufficiency. In fetal life it is the right side of the heart which plays the dominant role in the circulation of blood. As a result, this is the area to be more in requirement of oxygen and nutrients and also more susceptible for hypoxia and ischemia. This therefore explains the observation of right sided parameters to be abnormal with IUGR [20].
The findings when the comparison was made after dividing the cases based on the severity of IUGR showed varying results. In Mild IUGR, the late diastolic velocities of both ventricles are found reduced. This indicates that the atrial contraction phase of both sides of the heart is the first to be affected with the onset of hypoxia and cerebroplacental redistribution. This is understandable on account of its being a more active process with respect to the other phases requiring more oxygen and nutrients for its effective function.
The moderate IUGR babies with their non-significant variables demonstrate an adaptation of the myocardium to tide over the difficult conditions and bring on a state of homeostasis. The affected variables in severe IUGR indicate the failure of these compensatory mechanisms leading back to ischemic changes. As stated earlier, the right side of the heart is the more active side and hence its whole myocardial function is affected than the left where the passive early diastolic velocity has just started to reduce.
Myocardial tissue Doppler found no differences in the IUGR babies with normal and abnormal Doppler. Though this suggests ischemic myocardial changes even before the deterioration of the fetus can be picked up by vessel Doppler, it also indicates myocardial tissue Doppler is not able to differentiate between the fetuses requiring immediate attention and those not as the former.
A major limitation of this study is that not many very severe IUGR babies (birth weight <1kg) could be included. This was because many of these cases were unbooked and referred with fetal compromise necessitating immediate delivery. As a result, whether the dysfunction spreads to the left ventricle and interventricular septum was not seen. Another limitation is that Troponin T levels of these babies could not be done to correlate presence of deranged Myocardial Doppler findings with actual myocardial damage. However, probable crossing of placental barrier by Cardiac Troponin may not have allowed a proper conclusion [2].
Different studies undertaken in this regard have found variable results. Watanbe [22] found a difference in the systolic cycle with right S’/left S’ higher in IUGR fetuses but lower in hydrops babies than normal growth ones. Naujorks [12] found higher left and septal E’/A’ and lower left E/E’ in IUGR. Comas [13] through their findings stated that there was higher E’/A’ and MPI’ in early IUGR while Larsen [23] had lower left and right A’ and higher left E’/A’ in IUGR. All these studies however have taken a small sample size of around 15-25 in contrast to our sample size of 62.
Another study undertaken by Comas [14] with 58 IUGR fetuses found a lower right E’ and A’ and higher MPI’ than normal growth fetuses. The study does not classify the type of severity of growth retardation of the fetuses taken. There could also genetic and ethnic factors owing to a different population leading to the slightly different findings.
In a study conducted by Niewiadomska-Jarosik [24] in 77 children, in the IUGR group, E wave and E/A ratio were significantly lower and A wave, isovolumetric relaxation time, deceleration time, myocardial performance index as well as E/E′ septal and E/E′ lateral indices were significantly higher compared to healthy peers. This study was conducted in children aged 5-11 years and the findings had the effects of growth of the subjects as well. It however also shows the persistence of myocardial dysfunction in IUGR with increasing age.
The present study was undertaken to see if the upcoming technique of Myocardial tissue Doppler which already has proved its mettle in adults and children could be applied successfully in fetuses as well. While comparing its use in IUGR babies and normal growth babies, significant difference was indeed found in the right ventricle parameters.
CONCLUSION
Myocardial tissue Doppler shows subtle cardiac dysfunction in IUGR babies in comparison to normal growth babies in the right ventricle particularly in babies with severe IUGR. Further research is needed to ascertain its utility in diagnosing cardiac dysfunction and perinatal complications in IUGR.
ACKNOWLEDGEMENTS
The authors would like to thank Dr. Ranjan Shetty, Dr. Lavanya Rai, Dr. Jyoti Shetty, Dr. Sapna Amin, Dr. Pratap Kumar and Dr. Muralidhar V. Pai for their valuable help and guidance in conducting this study.
FUNDING
Cost of study managed by Department of Cardiology, Kasturba Medical College, Manipal.
CONFLICT OF INTEREST
None
ETHICAL APPROVAL
Approved by Kasturba Hospital, Manipal Institutional Ethics Committee on 13th August 2011, Approval No IEC 219/2011.
- Arnardóttir S, Geirsson RT (2011) High Risk Pregnancy Management Options. In: James D, Steer P, Weiner C, Gonik B, Ahmet Alexander Baschat editors. Intrauterine growth restriction. 4th New York. Elsevier. pp: 173-196.
- Mäkikallio K, Vuolteenaho O, Jouppila P, Räsänen J (2000) Association of severe placental insufficiency and systemic venous pressure rise in the fetus with increased neonatal cardiac troponin T levels. Am J Obstet Gynecol 183: 726-731.
- Acharya G, Räsänen J, Mäkikallio K, Erkinaro T, Kavasmaa T, et al. (2008) Metabolic acidosis decreases fetal myocardial isovolumic velocities in a chronic sheep model of increased placental vascular resistance. Am J Physiol Heart Circ Physiol 294: 498-504.
- Crispi F, Hernandez-Andrade E, Pelsers MM, Plasencia W, Benavides-Serralde JA, et al. (2008) Dysfunction and cell damage across clinical stages of severity in growth-restricted fetuses. Am J Obstet Gynecol 199: 254.
- Mäkikallio K, Vuolteenaho O, Jouppila P, Räsänen J (2002) Ultrasonographic and biochemical markers of human fetal cardiac dysfunction in placental insufficiency. Circulation 105: 58-63.
- Bahtiyar MO, Copel JA (2008) Cardiac changes in the intrauterine growth-restricted fetus. Semin Perinatol 32: 190-193.
- Baschat AA (2011) Intrauterine growth restriction. In: James D, Steer P, Weiner C, GonikB, editors. High Risk Pregnancy Management Options. 4th edn New York. Elsevier. pp: 173-196.
- Maulik D (2005) Introduction to Fetal Doppler Echocardiography. In: Maulik, Doppler Ultrasound in obstetrics and gynecology. 2nd edn New York. Springer. pp: 465-482.
- Harada K, Tsuda A, Orino T, Tanaka T, Takada G. (1999) Tissue Doppler imaging in the normal fetus. Int J Cardiol 71(3): 227-234.
- Paladini D, Lamberti A, Teodoro A, Arienzo M, Tartaglione A, et al. (2000) Tissue Doppler imaging of the fetal heart. Ultrasound Obstet Gynecol 16(6): 530-535.
- Tutschek B, Zimmermann T, Buck T, Bender HG (2003) Fetal tissue Doppler echocardiography: detection rates of cardiac structures and quantitative assessment of the fetal heart. Ultrasound Obstet Gynecol 21(1): 26-32.
- Naujorks AA, Zielinsky P, Beltrame PA, Castagna RC, Petracco R, et al. (2009) Myocardial tissue Doppler assessment of diastolic function in the growth-restricted fetus. Ultrasound Obstet Gynecol 34: 68-73.
- Comas M, Crispi F, Cruz-Martinez R, Martinez JM, Figueras F, et al. (2010) Usefulness of myocardial tissue Doppler vs. conventional echocardiography in the evaluation of cardiac dysfunction in early-onset intrauterine growth restriction. Am J Obstet Gynecol 203: 451-457.
- Comas M, Crispi F, Cruz-Martinez R, Figueras F, Gratacos E (2011) Tissue Doppler echocardiographic markers of cardiac dysfunction in small-for-gestational age fetuses. Am J Obstet Gynecol 205: 571-576.
- Fouzas S, Karatza A, Davlouros PA, Chrysis D, Alexopoulos D, et al. (2014) Neonatal cardiac dysfunction in intrauterine growth restriction. Pediatr Res 75: 651-657.
- Comas M, Crispi F (2012) Assessment of fetal cardiac function using tissue Doppler techniques. Fetal Diagn Ther 32(1-2): 30-38.
- Maulik D (2005) Doppler Ultrasound in obstetrics and gynecology. In: Maulik William J Ott, editors. Doppler Ultrasound in the Diagnosis and Management of IUGR. 2nd New York. Springer. pp: 281-293.
- Mishra R (2007) Ian Donald’s Practical obstetric problems. In: Misra R, Bhatla N, Kochar S. editors. Intrauterine growth restriction. 6th New Delhi. B I Publications pp: 333-344.
- Elmstedt N, Ferm-Widlund K, Lind B, Brodin L-A, Westgren M (2012) Fetal cardiac muscle contractility decreases with gestational age: A color-coded tissue velocity imaging study. Cardiovasc Ultrasound 10: 19.
- Verburg BO, Jaddoe VW, Wladimiroff JW, Hofman A, Witteman JC, et al. (2008) Fetal hemodynamic adaptive changes related to intrauterine growth: The Generation R Study. Circulation 117: 649-659.
- Iacovidou N, Boutsikou M, Gourgiotis D, Briana DD, Baka S, et al. (2007) Perinatal changes of cardiac troponin-I in normal and intrauterine growth-restricted pregnancies. Mediators Inflamm 2007: 53921.
- Watanabe S, Hashimoto I, Saito K, Watanabe K, Hirono K, et al. (2009) Characterization of ventricular myocardial performance in the fetus by tissue Doppler imaging. Circ J 73(5): 943-947.
- Larsen LU, Petersen OB, Sloth E, Uldbjerg N (2011) Color Doppler myocardial imaging demonstrates reduced diastolic tissue velocity in growth retarded fetuses with flow redistribution. Eur J Obstet Gynecol Reprod Biol 155(2): 140-145.
- Niewiadomska-Jarosik K, Zamojska J, Zamecznik A, Wosiak A, Jarosik P, et al. (2017) Myocardial dysfunction in children with intrauterine growth restriction: an echocardiographic study. Cardiovasc J Afr 28(1): 36-39.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6
-
Table 7







QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Advance Research on Alzheimers and Parkinsons Disease
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Allergy Research (ISSN:2642-326X)


