
4174
Views & Citations3174
Likes & Shares
Background: Tinnitus is a prevalent disorder affecting the quality of life in 0.5-3% of the population. We aimed to develop a novel treatment protocol for the tinnitus through multimodal brain stimulation.
Pre-treatment:
- Informed consent
- Pitch and loudness matching.
Post-treatment:
- Pitch and loudness matching
- Directive counseling and obtaining feedback.
Results: The perception of tinnitus was no longer present in four subjects, while in the remaining subjects, it was reduced to an intensity that no longer troubled them without causing residual facilitation. Across the 33 subjects, tinnitus intensity decreased by an average of 45 dBHL. However, in a few subjects, the intensity of tinnitus decreased by > 45 dBHL. The approach resulted in statistically significant reductions in Tinnitus Functional Index (TFI) and Tinnitus Handicap Inventory (THI) scores. The results correlate with pre and post-treatment THI scores, which dropped from 90% to 0%.
Conclusion: The present study suggests that this novel treatment approach is cost-effective, time-saving, and efficient in eliminating or significantly reducing tinnitus intensity, thereby eliminating negative reactions toward tinnitus.
Keywords: Tinnitus, Multimodal, Audiological, Tinnitus functional index, Tinnitus handicap inventory, Intensity
Writing simultaneously with both hands creates incoordination between both hands, which may be due to hemispheric conflict. Brain asymmetry allows the two sides of the brain to become specialized, increasing its processing capacity and avoiding situations of conflict where both sides of the brain take charge [7].
The Tinnitus Handicap Inventory (THI; [8]) was developed to measure the impact of tinnitus on daily life, with three subscales: functional, emotional, and catastrophic responses to tinnitus. While the overall questionnaire and the functional and emotional subscales show good internal consistency, subsequent validation studies found a unifactorial structure [9]. The Tinnitus Functional Index (TFI) was developed as a new measure of the severity and negative impact of tinnitus, encompassing psychological constructs such as attention, worry, anxiety, and depression, as well as functional constructs like hearing, social life, and activity level [10,11].
Tinnitus retraining therapy (TRT) is an effective treatment for tinnitus but may lead to consequences such as residual inhibition and facilitation. TRT effects are not permanent, as residual inhibition and facilitation occur after a certain period. It takes 12-24 months for individuals to habituate to the negative reactions to tinnitus and its perception, making it a lengthy process. Therefore, there is a need to develop a supplementary treatment or management procedure to reduce and/or eliminate the consequences of tinnitus, increasing efficacy, and reducing the overall treatment duration [12]. Hence, the present study was undertaken to develop a novel treatment protocol for tinnitus management through multimodal brain stimulation.
MATERIALS AND METHOD
The present study included 33 adults aged between 30 and 65 years with unilateral (31 subjects) and bilateral (2 subjects) chronic tinnitus with and/or without hearing loss, independent of their etiology. An audiological test battery was administered to ascertain the type and degree of hearing loss and the characteristics of their tinnitus. Tinnitus Handicap Inventory [8] and Tinnitus Functional Index [10] were administered before and after the treatment sessions to record the subjects' self-report about tinnitus.
The Treatment protocol included five consecutive sessions with a six-month follow-up, and each session of 90 min was divided into three parts:
Pre-treatment:
- Informed consent
- Pitch and loudness matching (20 min)
Treatment:
The bimanual paper-pen task with tinnitus masking (30 min)
Post-treatment:
- Pitch and loudness matching
- Directive counseling and obtaining feedback (40 min)
Session description: Pitch and loudness matching were done pre and post-session by presenting the pure tone and/or NBN in the ear contralateral to tinnitus. Then the subjects were instructed to perform bimanual paper-pen tasks for 30 min while narrowband noise of the same frequency as that of tinnitus was presented at 10 dBSL of tinnitus for 30 min simultaneously in the ear with tinnitus. The paper-pen task was performed bimanually and included carrying out two different writing activities of different contexts by using both hands simultaneously.
Directive counseling was focused on:
- Rationale of treatment
- The subconscious mind and the vicious cycle of tinnitus
- Attention, diversion, and ignorance from tinnitus
- Precautions to be taken to avoid relapse and follow-up
- Clearing subjects' doubts (if any)
The treatment program was conducted for five consecutive sessions, subsequent to which each subject was kept on a follow-up for a period of six months to eliminate the possibility of residual inhibition.
Statistical Analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) software, version 25 (IBM Corp., Armonk, NY, USA). Values for continuous variables are presented as mean ± standard deviation. The mean scores of TFI and THI were compared using the paired sample t-test. Differences with p
RESULTS
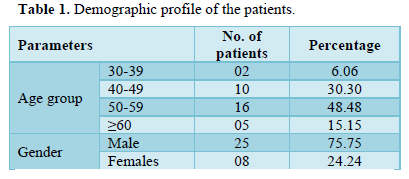
A total of 33 adult patients were enrolled in the study. Most of the patients were in the age group of 51-60 years (48.48%) with male predominance (75.75%), (Table 1). The mean age of patients was 57±11.3 years, ranging from 30-65 years.
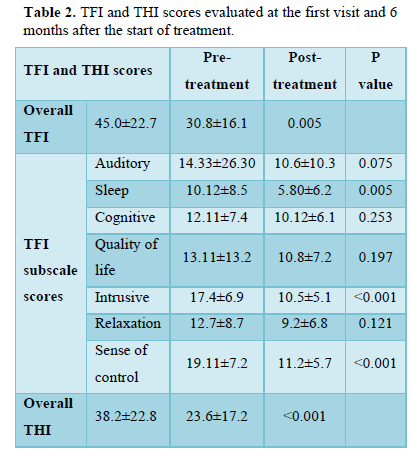
The perception of tinnitus was no longer present in 4 subjects while in the remaining subjects, it reduced to an intensity that its perception no longer troubled them without causing residual facilitation. The negative reactions (e.g., stress, anxiety, frustration, irritation) to the tinnitus were decreased in all subjects. Across the 33 subjects, the intensity of tinnitus decreased by an extent of 45dBHL an average. However, in a few subjects, the intensity of tinnitus also decreased by more than 45 dBHL. The approach resulted in statistically significant reductions in Tinnitus Functional Index and Tinnitus Handicap Inventory scores, (Table 2). The results correlate with pre and post-treatment score of the Tinnitus Handicap Inventory that dropped from 90% to 0%.
DISCUSSION
Brain mapping studies (qEEG) report multiple parallel overlapping subnetworks in non-auditory brain areas exhibiting abnormal, constant, and spontaneous neural activity related to tinnitus perception, with each subnetwork and area reflecting a specific aspect of tinnitus percept. The paper-pen task and directive counseling are designed and delivered to induce normal, rhythmically constant, and premeditated neural activity while masking the abnormal, constant, and spontaneous neural activity in the aforementioned subnetworks and specific non-auditory areas. Counseling focused on breaking the vicious cycle causing and maintaining tinnitus presence. Diverting auditory attention alone is insufficient to reduce tinnitus severity.
Bimanual paper-pen tasks represent top-down activities. Top-down processing refers to how the brain utilizes information already brought into the brain by sensory systems [13]. Top-down modulation underlies the ability to selectively attend to relevant stimuli and ignore irrelevant ones [14]. In this study, the bimanual paper-pen task represents top-down activity, allowing the brain to selectively attend to the bimanual written activity as a relevant stimulus and ignore tinnitus as an irrelevant stimulus.
Mechanisms underlying tinnitus suppression by task involvement may include the inhibition of auditory regions by top-down structures [15]. During the treatment procedure, various simultaneous ongoing processes in the brain may contribute to the aim:
- The paper-pen task is considered a relevant stimulus, focusing the brain on it while ignoring irrelevant tinnitus, contributing to the spontaneous habituation of tinnitus.
- fMRI studies report excess and abnormal neural firing in specific brain areas of individuals with tinnitus. The paper-pen task has been designed to increase communication between the right and left hemispheres of the brain, enhancing relevant neural activity in areas including the supplementary motor area, dorsolateral prefrontal lobe, orbitofrontal cortex, auditory cortex, and insula. This increased relevant neural activity is hypothesized to regulate abnormal neural firing, aiding in resolving tinnitus. fMRI studies during treatment sessions will help validate these hypotheses.
- Increased relevant neural activity in these areas may mask abnormally increased irrelevant neural activity causing tinnitus at the central level, suppressing centers responsible for tinnitus generation.
- Directive counseling, provided considering the subjects' backgrounds, helps in breaking the vicious cycle of maintaining tinnitus presence.
- Narrowband noise presented at 10dBSL of tinnitus for 30 min efficiently masks tinnitus. This combined effect of intensity and duration of masking noise overcomes residual inhibition and promotes permanent habituation to tinnitus perception [16].
CONCLUSION
The present study suggests that this novel treatment approach is cost-effective, time-saving, and efficient in either eliminating tinnitus or reducing tinnitus intensity to a negligible level, eliminating negative reactions towards tinnitus. The approach shortens the duration of a complete treatment program from 24 months to four weeks or even less. fMRI studies conducted during treatment sessions will help monitor changes in neural activity within the brain, providing the rationale for the success of this approach.
- McFadden D (1982) Tinnitus: Facts, Theories, and Treatments. Washington, DC: National Academy Press: Washington, DC 13(3): 150.
- McCormack A, Edmondson-Jones M, Somerset S, Hall D (2016) A systematic review of the reporting of tinnitus prevalence and severity. Hear Res 337: 70-79.
- Biswas R, Hall DA (2020) Prevalence, Incidence, and Risk Factors for Tinnitus. Springer Berlin Heidelberg pp: 1-26.
- Jastreboff PJ, Hazell JWP (1994) Neurophysiological model of tinnitus: Dependence of the minimal masking level on treatment outcome. Hear Res 80: 216-232.
- Salvi RJ, Lockwood AH, Burkard R (2000) Neural plasticity and tinnitus. In: Tyler R, ed. Tinnitus Handbook. San Diego: Singular pp: 132-148.
- Cacace AT (2003) Expanding the biological basis of tinnitus: Cross-modal origins and the role of neuroplasticity. Hear Res 175: 112-132.
- Wilson PH (2009) Classical conditioning as the basis for the effective treatment of tinnitus-related distress. ORL J Otorhinolaryngol Relat Spec 68(1): 6-13.
- Newman CW, Jacobson GP, Spitzer JB (1996) Development of the Tinnitus Handicap Inventory. Arch Otolaryngol Head Neck Surg 122(2): 143-148.
- Kennedy V, Wilson C, Stephens D (2004) Quality of life and tinnitus. Audiol Med 2: 29-40.
- Meikle MB, Henry JA, Griest SE, Stewart BJ, Abrams HB, et al. (2012) The tinnitus functional index: Development of a new clinical measure for chronic, intrusive tinnitus. Ear Hear 33(2): 153-176.
- Fackrell K, Hall DA, Barry J, Hoare DJ (2018) Performance of the Tinnitus Functional Index as a diagnostic instrument in a UK clinical population. Hear Res 358: 74-85.
- Bauer CA, Berry JL, Brozoski TJ (2017) The effect of tinnitus retraining therapy on chronic tinnitus: A controlled trial. Laryngoscope Investig Otolaryngol 2(4): 166-177.
- Baluch F, Itti L (2011) Mechanisms of top-down attention. Trends Neurosci 34(4): 210-224.
- Gazzaley A, Cooney JW, McEvoy K, Knight RT, D'Esposito M (2005) Top-down Enhancement and Suppression of the Magnitude and Speed of Neural Activity. J Cogn Neurosci 17(3): 507-517.
- Searchfield GD, Kobayashi K, Sanders M (2012) An adaptation level theory of tinnitus audibility. Front Syst Neurosci 6: 46.
- Feldmann H (1971) Homolateral and Contralateral Masking of Tinnitus by Noise-Bands and by Pure Tones. Audiology 10: 138-144.
-
 Table 1
Table 1 -
Table 2


QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Stem Cell Research and Therapeutics (ISSN:2474-4646)
- Journal of Cell Signaling & Damage-Associated Molecular Patterns
- Oncology Clinics and Research (ISSN: 2643-055X)
- Journal of Renal Transplantation Science (ISSN:2640-0847)
- International Journal of Clinical Case Studies and Reports (ISSN:2641-5771)
- Journal of Spine Diseases
- Journal of Clinical Trials and Research (ISSN:2637-7373)


