Research Article
Depression, Anxiety and Stress Levels Among Medical and Dental Students in North India
1487
Views & Citations487
Likes & Shares
Introduction: In medical and dental colleges increased levels of psychological disturbances such as depression, anxiety, and stress (DAS) among students affect the way these students take care of patients while moving from pre- clinical to clinical departments.
Aim: The aim of this study is to assess DAS among undergraduate medical and dental students in Mathura city, Uttar Pradesh, India.
Materials and Methods: The medical and dental college students from K.D Medical College and K.D Dental College students were included. A short questionnaire version of depression, anxiety and stress scale was distributed and filled by students. Comparison among the variables was done using ANOVA and Independent t-test.
Results: The study group comprised 200 (23.7%) males and 645 (76.3%) females. The overall mean DAS score and its dimensions were not significant based on gender. Married students showed significantly more DAS compared to unmarried (P < 0.05). When the year of study was considered for all colleges together, the overall mean DAS score and its individual dimensions score were significantly high among III-year students followed by IV, I, and II years (P < 0.05).
Conclusion: Clinical years were more stressful than the nonclinical years. This suggests a need for special attention to the structure of the clinical program, particularly at the point of transition from the preclinical to the clinical phase.
Keywords: Anxiety, Dental, Depression, Students
INTRODUCTION
The Depression, Anxiety, Stress Scales (DASS) was developed in1995 to measure the presence of depression and anxiety and to address discriminating between anxiety and depression [1]. Depression, anxiety and stress (DAS) have been recognized by the World Health Organization (WHO) as an important mental health disorder. Among the global burden of diseases DAS are the fourth leading contributors and it has been projected that by 2020 will become the second leading contributors after the cardiovascular-related diseases [2]. Depression is a common mental disorder that presents with depressed mood, loss of interest or pleasure, feelings of guilt or low self-worth, disturbed sleep or appetite, low energy, and poor concentration [3]. Hence, depression is associated with a constellation of psychological, behavioral and physical symptoms. Anxiety is a psychological disorder that is associated with significant suffering and impairment in functioning with blend of thoughts and feelings characterized by a sense of uncontrollability and unpredictability over potentially aversive life events [4]. Stress, on the other hand, is a consequence of or a general response to an action or situation that places special physical or psychological demands, or both on a person. As such, stress involves an interaction of the person with the environment [5].
In general, everyone working or not working and employed or unemployed experiences these mental health disorders. However, students in health care are at the higher risk due to the educational and transitional nature of student's life which they are not coping up. They have to adjust themselves with life, environment which requires compliance with academic stress, dealing with patients, new social norms and new people they meet and live. Very important that increasing demand to perform well academically and professionally may contribute to increasing levels of DAS. Depression is a serious and often under-diagnosed mental health problem in college students which may have fatal consequences.
Medical and dental colleges are known to be highly demanding and stressful learning environments. These professions are one of the top professional courses chosen because of their esteemed place and financial security in the Indian society. The students are experiencing the burden of vast syllabus, high level of competition, inability to cope up with the high expectations of parents after joining the course. This usually creates stress among them which will have negative impact on their mental status of health leading to sleep deprivation, reduced concentration, lack of confidence in handling patients, loss of self-esteem, anxiety, depression, interpersonal conflict, substance abuse, suicidal attempts etc. leading to elevated levels of DAS among students [6].
Retrieving knowledge about psychiatric morbidity is important as early detection and intervention may help in preventing and minimizing the effects of distress and help the students to deliver the best comprehensive care to the patients in the future. It is no surprise that mental health of medical students in India as an area of research domain has attracted the second highest attention of the faculty in medical colleges of country after medical education, learning process, and evaluation [7]. Extraordinary pressures, including a heavy schedule are responsible for depressive symptoms and major stressor for all the dental students was examination and grades and fear of facing parents after failure followed by full working day, receiving criticism from supervisors about academic or clinical work, amount of cheating in dental faculty, rules, and regulations of the faculty and fear of unemployment after graduation [8]. Hence, the present study aimed to assess the DAS among medical and dental students using depression, anxiety, and stress scale (DASS-21). The objectives of the study were to measure the presence of anxiety, stress and depression in medical and dental undergraduates based on gender and type of course.
METHOD AND MATERIALS
Study Design and Participants
A cross-sectional questionnaire survey was conducted among undergraduate medical and dental students studying in K.D Medical college and K.D Dental college, Mathura. Uttar Pradesh, India. for a period of 6 months. After obtaining the Institutional Ethical Committee approval, the Dean of both medical college and dental college was met and permission was obtained to conduct the study among the medical students. The study was conducted in full accordance with the World Medical Association Declaration of Helsinki. All the students studying in first year and final year spent more than six months and willing to participate in the study were included in the study. A self-administered measure was used to assess depression, anxiety and stress DASS-21 was distributed to undergraduate medical and dental students during lecture hours in the classroom. The details obtained from the students included age (in years), gender (male/female), year of study (I/II/III/IV), and college [4].
DASS-21 [9] is a 21-item short version synthesized from the original 42-item survey. This prevalidated questionnaire has seven items for each of the three scales designed to measure the negative emotional states of DAS. Items 3, 5, 10, 13, 16, 17, and 21 form the Depression scale; items 2, 4, 7, 9, 15, 19, and 20 form the anxiety scale and items 1, 6, 8, 11, 12, 14, and 18 are included in the stress scale. A four-point severity/frequency scale was used to rate the extent to which the respondents had applied/experienced each state/symptom over the past week from “never” (0), “some degree” (1), considerable degree (2) “most of the time” (3). The sum of the scores obtained was multiplied by 2 and then evaluated as per the severity-rating index. Details regarding socio-demographic characteristics were also collected.
Data were entered and analyzed using the Statistical Package for Social Sciences Software (Statistical data 2003 SPSS, Inc., an IBM company, Chicago, Illinosis, USA version 12.0). One way analysis of variance (ANOVA), Post-hoc analysis, and independent t-test was used for comparison among the variables. Correlation among the three variables of DAS was calculated by Karl Pearson correlation coefficient, and the internal consistency (reliability) for the DASS was measured using Cronbach's alpha. Differences were tested at a significance level of P < 0.05.
RESULTS
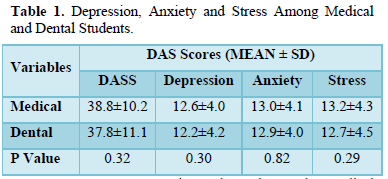
Out of 460 questionnaires distributed to medical and dental students, 415 students completed questionnaire yielding a response rate of 90.21%. The study group comprised 297 (71.56%) with mean age 21.26 ± 2.0 years in medical students and 118 (28.43%) dental students with mean age of 21.43 ± 1.87 years (Table 1).
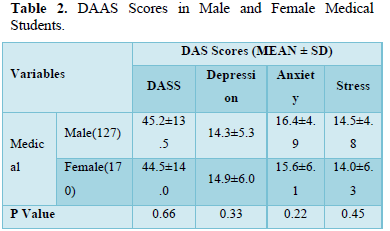
Out of a total of 297 medical students, the severity of Depression scores was mild n=12, moderate n= 7, severe N=4, extremely severe (n = 3). Anxiety score were mild (n= 15), moderate(n=7), (severe =4) and extremely severe (n = 2). Stress was, mild (n= 16), moderate (n= 5), severe (n = 4), extremely severe (n = 3) (Table 2,3).
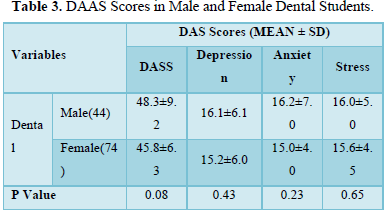
Out of a total of 118 dental students, the severity of Depression scores was mild n=12, moderate n= 7, severe N=4, extremely severe (n = 3). Anxiety score were mild (n= 15), moderate(n=7), (severe =4) and extremely severe (n = 2). Stress was, mild (n= 16), moderate (n= 5), severe (n = 4), extremely severe (n = 3) (Table 4).
DISCUSSION
It has been reported that dental students express considerable stress symptoms during their training and that they are more anxious than the general population, showing higher levels of depression, obsessive-compulsive disorders, and interpersonal sensitivity than age-matched norms [10]. Thus, recognizing the importance of mental health, the present study was carried out to assess the DAS among undergraduate dental students in Hyderabad city using DASS-21.
The DASS is the only self-report scale which measures all the three negative emotional states, i.e., depression, anxiety, and stress altogether and is designed to maximize discrimination between the three components it measures [9]. The DASS has high reliability and a factor structure that is consistent with the allocation of the items to subscales, exhibiting high convergent validity with other measures of anxiety and depression in both clinical and community samples [9,11]. In the current study, we have used DASS-21 which is a short form of the DASS-42 and has a number of advantages over the full-length version. First, and most obviously, it takes less time to complete. Second, the items retained from the full-length version are generally superior to those omitted and as a result, has a cleaner factor structure. Furthermore, it has been revealed that the short form of DAS is more consistent compared to full-scale version [9,11]. In India, there has been an increase in the number of women taking up dentistry [12]. This has been identified in the present study as well where in 76.3% of the study participants were females. In our study, the overall mean DAS score and its dimensions between male and female students were not statistically significant. This is in agreement with the findings reported by Bradely [13] and Heath [6] but in contrast with studies done by Alzahem [14] and Madhan [15] wherein they reported female students to have more DAS levels.
When marital status was considered, married students showed more symptoms of all the three negative emotional states, i.e., DAS than their unmarried colleagues. This could be due to increased responsibilities wherein the students have to simultaneously balance their personal and professional life. Conversely, in a study by Madhan [15] more symptoms were observed in unmarried students.
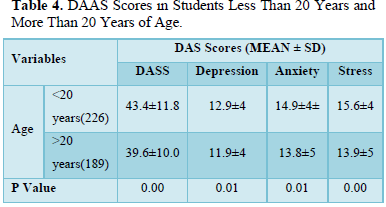
In this study, when academic years of all the four colleges together were considered, the overall DAS score was higher among III Year students. This can be due to the fact that in this year of study students are introduced to clinical training involving patients for the first time and need to concentrate on both dental and medical subjects. In addition, they are required to directly deal with patients and have to complete certain clinical requirements. Patient being late or not showing up for their appointment may contribute to increase in the stress. Our findings are in agreement with previous studies, which suggest that clinical years are more stressful than the nonclinical years [10,16]. On the other hand, findings reported by Westerman [11] showed that the nonclinical years (I and II) were more stressful.
The present study has to be generalized with a limitation such as the self-reporting and close-ended nature of the questionnaire since there is no interviewer to intervene in the case of any misunderstanding in the communication exchange between the researcher and the respondent. Close-ended questions limit the respondent to the set of alternatives being offered.
CONCLUSION
The present study reports high prevalence of DAS among this group of undergraduate dental students. While the first two (preclinical) years have less prevalence, dental students in the clinical years have more. This suggests a need for special attention to the structure of the clinical program, particularly at the point of transition from the preclinical to the clinical phase. Moreover, the highest perceived sources of DAS reported by students should be further investigated and methods to minimize them should be developed and implemented. A congenial environment needs to be created in the dental schools so that students can pursue their studies with less anxiety or stress. Strategies for stress prevention and management should be implemented in dental schools to improve students' well-being, prevent drop out, and ensure proper patient care [17-22].
FUNDING
Nil
- Lovibond PF, Lovibond SH (1995) The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther 33: 335-343.
- World Health Organization. Mental Health: Depression. Available online at: http://www.int/mentalhealth/management/depression/definition/index.html
- Marcus M, Yasamy MT, Van Ommeren M, Chisholm D, Saxena S (2012) Depression: A Global Public Health Concern. WHO Department of Mental Health and Substance Abuse. 1: 6-8.
- Md Yasin AS, Dzulkifli MA (2009) Differences in psychological problems between low and high achieving students. J Behavior Sci 4: 60-71.
- Ghaderi AR, Kumar V, Kumar S (2009) Depression, anxiety and stress among the Indian and Iranian students. J Indian Acad Appl Psychol 35: 33-37.
- Heath JR, Macfarlane TV, Umar MS (1999) Perceived sources of stress in dental students. Dent Update 26: 94-98.
- Sachdeva S, Sachdev TR, Sachdeva R, Dwivedi N, Taneja N (2017) Published research studies conducted amongst Indian medical undergraduate students: Bibliometric analysis. Indian J Community Health 29: 287-291.
- Acharya S (2003) Factors affecting stress among Indian dental students. J Dent Educ 67: 1140-1148.
- Harikiran AG, Srinagesh J, Nagesh KS, Sajudeen N (2012) Perceived sources of stress amongst final year dental under graduate students in a dental teaching institution at Bangalore, India: A cross sectional study. Indian J Dent Res 23: 331-336.
- Schmitter M, Liedl M, Beck J, Rammelsberg P (2008) Chronic stress in medical and dental education. Med Teach 30: 97-99.
- Lovibond SH, Lovibond PF (1995) Manual for the Depression Anxiety Stress Scales. 2nd Sydney: Psychology Foundation.
- Pani SC, Al Askar AM, Al Mohrij SI, Al Ohali TA (2011) Evaluation of stress in final-year Saudi dental students using salivary cortisol as a biomarker. J Dent Educ 75: 377-384.
- Bradely IF, Clark DC, Eisner JE, De Gruchyy K, Singer DL, et al. (1993) The student survey of problems in the academic environment in Canadian dental faculties. J Dent Educ 57: 225-231.
- Alzahem AM, van der Molen HT, Alaujan AH, Schmidt HG, Zamakhshary MH (2011) Stress amongst dental students: A systematic review. Eur J Dent Educ 15: 8-18.
- Madhan B, Rajpurohit AS, Gayathri H (2012) Mental health of postgraduate orthodontic students in India: A multi-institution survey. J Dent Educ 76: 200-209.
- Tedesco LA (1986) A psychosocial perspective on the dental educational experience and student performance. J Dent Educ 50: 601-605.
- Takayama Y, Miura E, Miura K, Ono S, Ohkubo C (2001) Condition of depressive symptoms among Japanese dental students. Odontology 99: 179-187.
- Kieser J, Herbison P (2000) Clinical anxieties among dental students. N Z Dent J 96: 138-139.
- Kumar S, Dagli RJ, Mathur A, Jain M, Prabu D, et al. (2009) Perceived sources of stress amongst Indian dental students. Eur J Dent Educ 13: 39-45.
- Garbee WH Jr, Zucker SB, Selby GR (1980) Perceived sources of stress among dental students. J Am Dent Assoc 100: 853-857.
- Rajab LD (2001) Perceived sources of stress among dental students at the university of Jordan. J Dent Educ 65: 232-241.
- Westerman GH, Grandy TG, Ocanto RA, Erskine CG (1993) Perceived sources of stress in the dental school environment. J Dent Educ 57: 225-231.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4




QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)


