Journal of Tourism and Sports Management (ISSN: 2642-021X)

Research Article
IMPACT OF RISK AND IMAGE ON DESTINATION LOYALTY OF INTERNATIONAL MEDICAL TOURISTS IN PHUKET PROVINCE, THAILAND
30585
Views & Citations29585
Likes & Shares
This research aimed to develop and evaluate a conceptual structural model for establishing a medical tourist’s loyalty by integrating two main factors, namely risk and destination image. Specifically, the objective of this study was to investigate the relationships among risk, image and destionation loyalty in terms ofintention to revisit the destination as well as intention to recommend the destination to others. A quantitative approach was designed to develop and assess the proposed model. Data werecollected from international medical tourists who have travelled primarily to receive medical treatment in Thailand. A survey was designed and administered to clinics thatspecialize in health care for international visitors. The factorial validity of constructs wastested using confirmatory factor analysis (CFA) and Structural Equation Modelling (SEM)was used to test the goodness of the proposed model as well as the study’s researchhypotheses. The empirical results indicate a good fit for the proposed model. The findings also confirmed that perceived risk positively influences image in terms of cognitive, affective and overall dimensions. In turn, both the cognitive and affective dimensions of destination imagepositivelyinfluencethe overall image of medical tourism destination. Finally, medical tourists’ perception of affective and overall dimensions of destination image had positive impact on the destination loyalty. However, their perceived cognitive image did not have a significant influence on their destination loyalty. Both theoretical and practical implications are discussed.
Keyword: Tourist Loyalty, Risk, Destination Image, Medical Tourism
INTRODUCTION
Medical tourism is a niche special interest tourism segment in the globalized health industry (Connell, 2006). Several researchers indicate that medical tourism is not a new phenomenon of travel for health or medical treatment overseas (Hutchinson, 2005). (Connell, 2006). (Smith&Puczkó, 2008). The rapid development of globalization and technological advancement in the past century has had a huge impact in shifting the role of medical tourismthroughout the world. Travel abroad for medical treatments is becoming very popular in the twenty first century as people are becoming more and more aware of their health needs (Campbell,2018). (Lunt, Hardey & Mannion, 2010). (Stanley, 2010). (Texas A&M University, 2016). Moreover, medical tourism is now the main cause of an economic growth in increasing importance as a global industry, with producers and consumers spread around the world. According to report titled “A Precription for a Healthier Economy” presented that international spending in medical tourism products and services grew by 358% in nominal terms between 2000 to 2017, increasing from US$ 2.4 billion (72.5 billion baht) to $11 billion (Bangkok Post, 2019). Thailand, Costa Rica and Mexico areconsidered some of the leading emerging economies for medical inbound spending indicating US$ 589 million, $451 and $315 million, respectively (TTR Weekly, 2019).Therefore, over 50 countries have considered medical tourism as a national industry (Gahlinger, 2008). due to the increasingly number of medical tourists as well as the average growth rate.
Consumer loyalty has been found to be a competitive tool for many tourism destinations in the literature.The growth and survival of medical tourism destinations depend on how loyal their customers arebecause the medical tourism industry is facing with today’s highly globalized and competitive markets.There is therefore a need to understand why medical tourists are faithful to medical tourism destinations, and what determines their loyalty. According to Aaker (1996), loyalty is the key consideration because a highly loyal customer base generates larger sales and profits. (Reichheld & Sasser,1990). asserted that a business might increase its profits by between 25% and 85% by retaining 5% of its customers. Other associated benefits are to fostering a lasting relationship with customers, including the fact that loyal customers are more likely to recommend destinations or businesses to others with a free advertising (Reichheld&Sasser,1990). Therefore, medical tourism destinations can create sustainable competitive advantage in the marketplace by keeping existing consumers rather than attracting new customers.
The literature review provides empirical evidence that trust (Abubakar & Mustafa, 2016; Han & Hyun, 2015; Lertwannawit & Gulid, 2011 & Mechida et al., 2010), human capital, high technology, physical infrastructure (Asyraf et al., 2017; Han & Hyun, 2015), quality (Han & Hyun, 2015;Lertwannawit and Gulid, 2011;Huei et al., 2015), value (Mechida et al., 2010;Lertwannawit & Gulid, 2011) and satisfaction (Asyraf et al., 2017; Han & Hyun, 2015; Lertwannawit & Gulid, 2011) have been considered key variables in influencing consumer loyalty in the context of medical tourism. Moreover, the literature presented that risk and image have consistently been regarded as key determinants in affecting customers’ loyalty. According to (Chi & Qu, 2008). and (Radder & Han, 2015), destination image and tourist satisfaction are important determinants predicting tourists’ intention to revisit a destination. However, no study has yet investigated in regard to relationships among risk, image and loyalty in the field of medical tourism. The present study therefore aimed to fill a gap in the literature. The purpose of this study is to develop and evaluate a conceptual model for establishing a medical tourist’s loyalty by using two main factors, namely risk and destination image affecting medical tourists’ intention to revisit the destination as well as intention to recommend the destination to others. More specifically, the objectives of this study are as followed:
- To investigate the relationship between perceived risk and destination image in terms of cognitive, affective and overall image perceived by medical tourists.
- To explore the role of destination image on consumer loyalty toward the medical tourism destination.
LITERATURE REVIEW
In literature review, theauthor discussed two independent variables, namely risk and destination image and one dependent variable, namely consumer loyalty from the past studies done by other researchers. The author also defined and described in details on each variable with the supporting literature. Therefore, this section reviewed the relevant literature as well as proposed eighthypotheses.
DESTINATION LOYALTY
Due to the increasing competition in medical tourism, loyalty has become a critical part of destination marketing because it can sustain the business as well as the medical tourism destination in the long term by saving marketing costs caused by retaining existing customers and spreading positive recommendations to others. (Oliver,1999). has defined loyalty as “a deeply held commitment to rebuy or re- patronize a preferred product or service consistently in the future, causing same repetitive brand or same brand-set purchasing, despite situational influences or marketing efforts” (p.31). The concept of loyalty is one of the essential assets used to present the business or destination performance (Reichheld, 2003), to measure the success of marketing strategies (Flavian, Martinez, & Polo, 2001). and to a long-term sustainable profitability (Salegna & Goodwin, 2005). Specifically, (Huei et al. 2015). asserted that customer loyalty is the key element in medical tourism success and competitive advantage because medical tourist loyalty can save more cost in finding new customers as well as word-of-mouth promotion. This study focuses on the theories of loyalty in the area of tourism, recreation and medical tourism. The theories of loyalty in the area of medical tourism focused on intention to revisit and willingness to recommend to others. For example, the study of (Han&Hyun,2015). attempted to examine the relationships among perceived medical and service quality, satisfaction, trust and loyalty. The researchers of this study defined loyalty in terms of customer retention including intention to revisit the clinic and the destination country for medical care. The finding revealed that proposed factors, namely perceived medical and service quality, satisfaction and trust in staff and clinic have a strong explanatory power for outcome variables, effectively predicting intention to revisit the clinic and to revisit the destination for medical care. Similarly, (Kim et al. 2017). investigate the roles of servicescapes, emotions, and satisfaction in developing consumer loyalty that focused on post behavior including loyalty toward medical clinic and loyalty toward Korea. The results found that the interrelationship of servicescapes, positive emotion and satisfaction is essential in influencing international medical tourists’ loyalty to a medical clinic. (Abubakar&Mustafa,2016). also investigate the impact of online word-of-mouth on destination trust and intention to travel in the medical tourism sector. The finding presented that online word-of-mouth had a positive impact on destination trust and intention to travel. Additionally, the study of (Mechinda et al.2010). was conducted to investigate the antecedents of tourists’ attitudinal loyalty towards medical tourism. The factors predicting customer loyalty are examined, in other word s, the authors have used five variables; satisfaction, perceived value,trust, destination familiarity and destination image explaining consumers’ attitudinal loyalty towards medical tourism destinations. The authors’ intention is to inform theoretically and applied models for promoting medical tourist loyalty in brief continuing medical tourism industry by applying consumer loyalty from the business. The target population consisted of international medical tourists traveling to Thailand for the purpose of obtaining medical treatments as well as visiting the tourist attractions in Pattaya province, Thailand. The findings reviewed that these five factors including satisfaction, perceived value, trust, destination familiarity and destination image, have an influence on tourists’ attitudinal loyalty toward medical tourism in Pattaya, Thailand.
The researcher has decided to integrate two main dimensions of loyalty, namely behavioral and attitudinal loyalty based on a number of times in the setting of medical tourism (Han & Hyun, 2015, Kim et al., 2017; Huei et al., 2015). Behavioral loyalty is defined as a behavior that is shown by a consumer to a destination within the form of repeated purchases (Back & Parks, 2003). The other dimension or attitudinal loyalty refers to an attitude that is shown by a consumer to a destination within the form of recommending the product/ destination to other consumers (Dick & Basu, 1994; Dimitriades, 2006). To better understand consumer loyalty in terms of intention to revisit in the medical tourism industry leads to increase profitability and to maintain the position of the destination. Another perspective of a tourist loyalty to a medical tourism destination is a willingness to recommend the destination to others including friends, family, and relatives. Medical tourist with positive word-of-mouth to others is considered to be an important factor enhancing the destination image of the destination and therefore the growing number of tourists is accounted to that location (Marrocu & Paci, 2013).
PERCEIVED RISK
“Every willingly takes risks” (Adams, 1995). p.16 is regarded as the starting point of any theory of risk. As humans, we generally engage in some kind of dangerous events every day. Especially, tourists confront with unpredictable incidents all the time during their traveling to the tourist destination. A number of previous studies have discussed risk in the tourism industry, in particular since the 1990s (e.g. Roehl & Fesenmaier, 1992; Sönmez & Graefe, 1998; Maser & Weiermair, 1998). “Risk and tourism are interwoven as the purchase of leisure trip is inherently attached to risk” (Baker, 2015). p. 4. Because of unique features of tourism products and service, it is undeniable that these products and service inherit the intangibility, heterogeneity, perishability, and inseparability (Williams & Baláž, 2013). Consumers in the tourism industry might perceive greater risk than consumers in other industries. In taking up this point of view, researchers have directed substantial effort to understand the conceptualization of risk perceived by medical tourists. The survival of the tourism industry depends on how the destinations or businesses can possess the ability to manage risk as well as the skill to recognize it (Shaw et al., 2012). in hopes that the destinations with risk management will gain and achieve a competitive advantage (Shaw, 2010).
There are numerous definitions of perceived risk from the tourism industry literature. For example, (Sonmez & Graefe 1998). is one of the most cited articles in the discussion of perceived risk definition. The authors define perceived risk as tourists’ perceptions are concerned about damaging to the decision to travel rather than actual security. (Reisinger&Mavondo, 2005). defined risk as the uncertainty as well as negative consequences of buying a product. The perception of risk is also defined as an individual’s subjective assessment of the real risk present at any time (Chang, 2010). The study of (Fuchs&Reichel,2011). defined perceived risk as “a consumer’s perception of the overall negativity of a course of action based upon an assessment of the possible negative outcomes and the likelihood that those outcomes will occur” (p.267). A study by (Yang &Nair,2014). proposed the relationship chains of concepts related to risk perception from a previous literature. The authors argued that relationship chains generated by perceived risk and fear consist of two separate main streams. (Hofstede,2001). indicates that both risk perception and fear are induced by direct stimulus, more specifically; an object triggers fear while perceived risk is triggered by an event with known probability.
Many scholars indicated that there are an increasing number of studies on risk in tourism since the attack of 9/11 in 2001 coupled with major tragedies, like the SARS outbreak, the Bali bombings, and the Asian tsunami, resulting in tourist flows as well as regional stagnation (McCartney, 2008; Shin, 2005; Kovari & Zimmyi, 2011; Lepp & Gibson, 2003; Pizam et al., 2004; Simpson & Siguaw, 2008; William & Balaz, 2013; Yang & Nair, 2014). Indeed, the literature pointed out that tourism studies on risk and safety has discussed since 1970s (Sonmez & Graefe, 1998; Tsaur, Tzeng & Wang, 1997; Pizam, 1999). and has exponentially increased in the 1990s (Maser & Weiermair, 1998; Roehl & Fesenmaier, 1992; Sönmez & Graefe, 1998). As mentioned by (Blake &Sinclair,2003). (Santana,2004). unforeseen crises as well as risks can significantly impact on a long-term sustainability and the destination’s economy. There has been much dispute between perceived and actual risk in the tourism industry literature. The study of (Dickson & Dolnicar, 2004). claimed that risk perception is highly subjective. However, the tourism literature emphasized that most studies have focused on perceived or subjective risk rather than real or objective risk (Reisinger &Mavondo, 2005; Quintal, Lee, & Soutar, 2010). This may be because it might be difficult to identify the actual scale and range of risk, as indicated by (Bentlet et al., 2001). It is critical to be aware of the fact that investigating tourists’ perceived risk is very important topic for researchers since perceived risk has a positive impact on their current and future travel decision (Yüksel & Yüksel, 2007).For example, the study of (Roehl & Fesenmaier,1992). investigated perceived risk in three dimensions including physical-equipment risk, vacation risk, and destination-specific risk while the other study by (Pennington-Gray&Schroeder,2013). has proposed seven types of risk perception from international tourists including crime, disease, physical, equipment failure, weather, cultural barriers, and political crises. Additionally, a substantial body of tourism literature has identified many studies regarding the perception of tourist risk in terms of travel (Roehl & Fesenmaier, 1992; Sönmez & Graefe, 1998; Maser & Weiermair, 1998; Lepp & Gibson, 2003 Floyd et al., 2004; Dolnicar, 2005; Reisinger & Mavondo, 2006; Kozak et al., 2007; Carlton & Jacobson, 2013). as well as risks perceived at the destination (Fuchs & Reichel, 2006; Eitzinger & Wiedemann 2007; Fuchs & Reichel, 2011; Schroeder et al., 2013; Karamustafa et al., 2013; Çetinsöz & Ege, 2013). Moreover, past studies have provided empirical evidences to support the idea that risk is a key indicator influencing tourists’ travelling in terms of tourists’ decision-making and travel experience (Teng, 2005; Kovari & Zimanyi, 2011). Most researchers found that perceived risk has a strong inverse relationship with travel intentions; in other words, intentions to travel will lower if perceptions of risk are high. (Reisinger & Mavondo,2005). have confirmed that travel safety exhibited a positive association on intentions to travel but conversely travel safety was negatively associated with travel anxiety. Finally, the majority of previous research in the tourism literature has identified the multidimensional nature of the perceived risk construct. In a more relevant study, (Roehl &Fesenmaier,1992). empirically tested the effects of seven facets of risk including equipment risk, financial risk, physical risk, social risk, satisfaction risk and time risk perceived by tourists during their holidays. In addition to the above seven facets, possible four dimensions of risk that includes financial, psychological, satisfaction and time risks have been discussed in the study of (Sönmez&Graefe,1998). In the 2000s, (Lepp & Gibson,2003). have used seven facets of risk perceived by American: health, political uncertainties, terrorism, foreign food, cultural handicaps, political and religious rules and crime risks. A year later, Floyd and his colleagues (2004) found that there was a significant affiliation with travel intention of participants in New York after the 9/11 attacks to travel a holiday during the next year and five facets of risk including perceived social risk, security concerns, travel experience and income. Dolnicar (2005) has suggested five dimensions of perceived risk in examining tourists who intend to travel in domestic and in oversea. These five dimensions of risk included political, environmental, health, planning and property risks. The nationality is used to determine an impact on perceived risk in the study of (Reisinger & Mavondo,2006). The authors included thirteen travel risks including financial, cultural, health, equipment/functional, physical, psychological, political, satisfaction, time, social, missing flights and detonating explosives and biological. The results presented there was a significant relationship between the nationality of tourists and risk perception. More specifically, risk perceived by tourists from Hong Kong, Australia and the United States was higher than the risk perception of tourists from Canada, Greece and the United Kingdom. There are many studies investigating the risk perception in several countries. For instance, (Çetinsöz & Ege,2013). have attempted to risks perceived by foreign tourists during traveling in Alanya. This study has focused on five different facets of risk that included physical risks, satisfaction, time risk, socio-psychological risks and functional risks. Another study by (Schroeder et al,2013). demonstrated the perceived risks of American citizens toward the summer Olympics of 2012 in London and the perceived risk of this study included natural disasters, SARS, food safety, financial crises, infrastructural problems, poor weather conditions, political problems and terror incidents. Crime rates and the terror activities are the highest risks perceived by the respondents. The other study by (Karamustafa et al. 2013) aimed to examine the perceived risks regarding Turkey as a tourism destination including six dimensions of risk: time and social risk, financial risk, physical risks geopolitical risks, risks involving holiday experiences, weather conditions and risks regarding hotels. Therefore, the study of perceived risk is still an important issue for researchers in the context of tourism since how tourists perceive risk is more likely to affect their travel in the future.
In attempting to understand the manner in consumers who engage in the new emerging market or medical tourism, it appears that perceived risk is one of the main concerns for medical tourism destination around the world. As mentioned in several previous studies, a tourism product is mostly a service rather than product. (Reisinger et al. 2010). further explained that service has focused on the service process, performance and service encounter, in other words, the interaction between the customer and the firm or service provider. That means service industry characterized by their inherent properties, namely heterogeneity, perishability, inseparability and intangibility (Guseman, 1981; Murray & Schlacter, 1990; Mitchell & Greatorex, 1993; Mitchel, 1999). Although tourism industry is found to be closely related to uncertainty, worry, fear and anxiety, medical tourism is riskier than other types of tourism because of the purpose of medical tourism, combining both travelling and obtaining medical treatments in other countries. There are a number of reasons why perceived risk is an appropriate place to look at the manner in which traditional theories and propositions of marketers hold up in the medical tourism segment. First of all, the concept of perceived risk offers on the basis of a comprehensive view explaining why medical tourists are often motivated to avoid negative aspects rather than to seek positive aspects in a given buying situation. As noted by (Mitchell,1999). the theory of perceived risk demonstrates that consumers begin the process of inclining to minimize the perceived risk instead of maximizing the expected pay off or positive result. In addition, it has some evidence to show that when risk perceived by consumers has been noticed in a buying situation, it has been shown the subsequent consumer in line with such risks (Taylor, 1974). Second, the increased perceived risk analysis in medical tourism leads to increase marketing efficiency. In other words, to better understand how medical tourists’ perceived risk about the destination in oversea, can bring more useful strategies into all marketing activities including segmentation, positioning, targeting and also image development. Third, perceived risk theory is expandable to almost all kinds of consumer products and services. The successful theory of perceived risk can ever be definitely proven by previous studies with a wide range of different product types (Mitchell, 1999; Hisrich et al., 1972; Cunningham, 1967; Arndt, 1967; Peter & Tarpey, 1975). Therefore, investigating consumer risk perception within medical tourism environment offers a great deal to potential medical tourism marketing. More specifically, the perceived risk can influence marketing decision making concerning efficient resources location (towards marketing strategies considering the impact of products’ perceived risk), segmentation strategies can be designed according to risk reduction strategies employed by customers (Mitchell & McGoldrick, 1996; Mitchell, 1999), perceived risk can be considered to develop the image and positioning of a brand and it can even help to generate ideas for new products (Mitchell & Boustani, 1993). In the context of medical tourism, few previous studies have used perceived risk as one of antecedents of tourists’ behavioral intention to travel for medical care to a foreign destination (Wang & Wang, 2013; Garrouch, 2015). As noted by Crooks et al., 2010 and Turner, 2011, as health-care practices differ among countries, patients seeking offshore treatment are exposed to several risks. (Samir & Kasim,2011). indicated that it is necessary to understand that medical tourism is not a completely regulated industry. As mentioned by Hall (2013), in medical tourism, where the focus is curative and the traveler is, by tendency, ill, the perceived risk tends to be much higher as much more is at stake than in other subsectors of health tourism, for example, wellness tourism, where the focus is on wellbeing in general. (Bies& Zacharia,2007). (Crooks et al. 2010). (Leah,2008). point out that the main risks include exposure to medical malpractice, difficulties obtaining follow-up care, and the danger of infectious disease transmission.
In this study, perceived risk can be defined as the likelihood of perception of an individual about the probability that a particular action will lead them to a situation exposed with danger more than acceptable limit, and will lead to influence travel-making (Manfield, 2006). The present study attempted to investigate the underlying dimensions of risk perceived by international medical tourists in hopes that the findings will help to broaden the understanding of risk perception in the context of medical tourism. In particular, the author attempted to investigate the relationship between perceived risk and destination image. The author would not depend on the multidimensional of perceived risk. Instead, the author analysed the perceived riskas a whole. However, the author would not focus on which dimension of perceived risk is influencing the other parameters.
DESTINATION IMAGE
There are various definitions found in the literature. The majority of previous studies defined destination image as a set of ideas, expectations, emotion thoughts and impressions that a person as toward a specific destination (Kim & Richardson, 2003; Assaker, 2014; Baloglu & McCleary, 1999; Beerli & Martin, 2004). Similarly, the study (Crompton,1979). is one of the most commonly cited terms of destination image describing as “the sum of beliefs, ideas and impressions that a person has of a destination” (p.18). In the field of tourism industry, a construct of image is widely applied in many tourist destination researches because of tourism depending on image (Tasci & Gartner, 2007). The image of destination is a very important concern perceived by tourists rather than other tangible resources and also the perception of destination image has become more popular area of investigation than the reality among tourism studies (Gallarza et al., 2002). It is not easy to assess destination image perceived by tourists due to tourism industry relying more on service than physical products (Nadeau et al., 2008) as well as the differences in perceptions of the same destination among different visitors (Pike, 2004). Likewise, several researchers asserted that the difficulty of assessing the image of destination for a certain place since images can be different regarding to different markets (Fakeye & Crompton, 1991; Leisen, 2001; Russell, Thomas & Fredline, 2005). However, the topic of destination image is still receiving the attention of both academics and practitioners based on the fact that destination image has been found to influence choice of destinations, travel decision, (Hunt, 1975; Chen & Tsai, 2007; Nadeau et al., 2008), satisfaction and post-purchase behavior (Chon, 1990; Um & Crompton, 1990; Echtner & Ritchie, 1991; Oppermann, 2000; Bigné et al., 200; Echtner & Ritchie, 2003; Chen & Tsai, 2007; Zhang et al., 2014).
Several researchers utilize three main dimensions of destination image – cognitive, affective and conative (Bloglu & McCleary, 1999; Dann, 1996; Konecnik & Gartner, 2007; Pike & Ryan, 2004; Stepchenkova & Mills, 2010; Tasci & Gartner, 2007; Tasci et al., 2007). The study of Boulding (1956) indicated that an image comprises what one knows and thinks about an object (cognitive), how one feels about it (affective), and how one acts using this information (conative). More specifically, cognitive image may be considered as the sum of what is known about a destination consisted of induced or organic aspects (Gunn, 1988). It can be seen that cognitive image refers to knowledge, beliefs or awareness deriving from previous visits. The tourism industry literature pointed out that most studies analyze cognitive image by focusing on tangible physical attributes (Pearch, 1977; Pike, 2002). Affective image is described as an individual’s feelings towards an object including favorable, unfavorable, or neutral (Gartner, 1993). Similarly, affective component is described as the evaluation stage, concerning the feelings that the individual associates with the place of visit (Baloglu & Brinberg, 1997; Baloglu & McCleary, 1999; Beerli & Martín, 2004). Affective image has become operational in the evaluation stage of the destination selection process (Gartner, 1993) that had been overlooked selection in the literature of tourism industry (Walmsley and Young, 1998). (Baloglu & McCleary,1999). have further asserted that affective image has been considered one of the most influential factors in the tourism industry since this image always uses by destinations for better efficiency. In the study of (Pike,2002). the author has reviewed 142 published articles focusing on destination image in the literature and the study found that only six dimensions presented an explicit interest in affective images. However, four semantic differential scales used most often in the literature consist of positive dimension including arousing, exciting, pleasant and relaxing, and negative dimension including sleepy, gloomy, unpleasant and distressing (Baloglu & Brinbberg, 1997; Baloglu and McCleary, 1999; Baloglu &Mangaloglu, 2001). This is consistent with the study of (McLellan &Foushee,1983). that states that the image of destination can be described as a mixture of both positive and negative perceptions. In other words, tourists are more likely to consider and choose destinations with positive images in their travel decision process (Goodrich, 1978; Woodside & Lysonski, 1989). Finally, conative image is the likelihood of visiting a destination within a certain time period. The tourism industry literature composed of action in terms of the individual’s actual conduct or intention to revisit and recommend the destination to others (Bigné et al., 2001; Gartner, 1993; Konecnik & Gartner, 2007; Pike & Ryan, 2004; Tasci & Gartner, 2007; Tasci et al., 2007), and to spread positive word of mouth (Baker & Crompton, 2000).
There is a need to understand destination images related to the emerging tourism market, medical tourism. Although destination image has been interested in the tourism industry literature for a long time, this is rarely discussed in the work on the field of medical tourism. In general, destination image plays a big role in the marketing of a destination, particularly in the tourism industry. Similarly, destination image is considered one of the most important predictors in medical tourism (Mohamed et al., 2012). (Pollard,2012). stated that destination image is something hard to change or influence, in other words, “you are what you are… or what people believe you to be”. Image is often a simple version of impression about the destination created by the tourists. (Pollard,2012). Further illustrates that if medical tourists decide to travel the United States for medical treatment, they will find the latest technology with high cost. Moreover, if medical tourists go to India for medical tourism, they are bound to suffer “Delhi belly” at some stage. This implies that if the destination country of medical tourism has a positive image, medical tourists will draw on their perception of that destination, be they real or imagined. (Jalivand et al. 2012). mentioned that destination image positively affects tourists’ attitude. That means a positive image of medical tourism destinations will lead to positive attitude towards developing behavior intention of medical tourists. In other words, it is an important component that affects future customers’ decision-making process and behavior.
With regard to the importance of destination image in medical tourism industry, far less information is available with very few studies being conducted. Two studies have investigated the relationship between destination image and medical tourists’ attitudinal loyalty (Mechinda et al., 2010). and the relationship between brand image and perceived service quality (Huei et al., 2015). This study made under the assumption that a better understanding of the importance of image can bring insights with regards to more effective and efficient ways of marketing for medical tourism destinations. Realizing the current need to examine closely the perception of medical tourists, this study aims to incorporate destination image in terms of cognitive, affective and overall image of the destination perceived by medical tourists in building medical tourist loyalty model. Overall image of the destination can be defined as mental pictures a person holds about the characteristics of a destination including tourism infrastructure to cultural, natural and social attributes (Coshall, 2000; Beerli & Martin, 2004). While cognitive image refers to the individual’s own beliefs and knowledge and how individual perceived about the attributes of the destination (Beerli & Martín, 2004; Lepp, 2011), affective image refers to the evaluation stage, concerning the feelings that the individual associates with the place of visit (Beerli & Martín, 2004). The present study aims to integrate destination image in the customer loyalty of medical tourism literature in hopes that this can contribute to a better understanding this phenomenon as well as can create an appropriate destination image leading to his or her destination loyalty. In the view of the fact that a consumer is a critical part of a successful positioning, marketing strategy (Echtner & Ritchie, 1993), tourism development within a destination (Chon, 1990; Echtner and Ritchie 1991, 1993; Gunn, 1972; Hunt, 1975; Smith, 2001) and understanding tourists’ destination choice processes (Reilly, 1990).
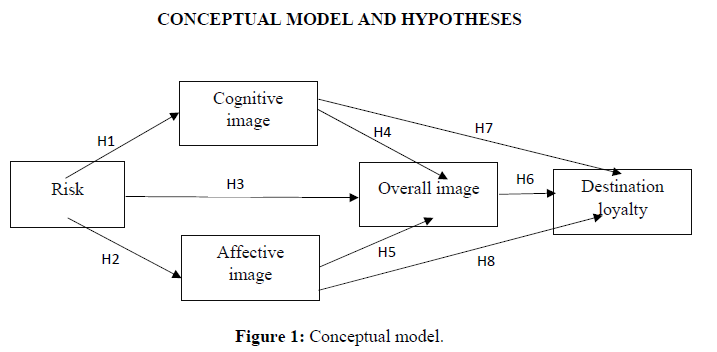
The model highlights the relationship between risk and image in terms of cognitive, affective and overall image perceived by medical tourists as presented in Figure 1. Many researchers in the tourism industry have investigated destination image for a long time. Tourism is unlike other industries, in other words, people have to buy in the sense that they are not able to fully see what you are buying before you travel to the destination. It is essential a destination holding a proper and accurate image. Having a positive image attached to a destination is a tool that will help to attract people to the destination. Therefore, the image of a destination is a key factor in conveying the destination’s physical attributes to tourists (Tasci & Gartner, 2007), attracting tourists as well as providing a positive travel experience (Prayag & Ryan, 2011). Due to destination image representing the very closely actual destination, destination image positively perceived by tourists play a significant role in competing against other destinations. It is critical to be aware of the fact that perceptions that people hold of a destination are crucial for the tourism industry as they directly influence individuals’ travel choices as well as their loyalty. In this manner, tourists’ negative awareness concerning safety and security present at a destination can prove disastrous for its ability to attract visitors (Resinger & Mavondo, 2005). So far it has been suggested that risk should be studied together with destination images because of crisis management teams, as well as destination managers, need to alter negative perception and reinforce positive perceptions (Sonmez, 1998). (Chew & Jahari, 2014). further asserted that researchers and practitioners need to understand these relationships better because perceived risk might have on tourists’ perceived destination image and travel choices. That means it is undeniable that risk and destination image are related concepts. Previous studies in tourism industry tend to examine risk perceptions isolating from destination image (Floyd et al., 2003; Fuchs & Reichel, 2011; Kozak et al., 2007). Very few studies have focused on the relationship between perceived risk and image perceived by tourists in the literature of tourism industry, yet no studies in the context of medical tourism. Therefore, this relationship is needed to better understand by medical tourism destinations to provide useful information for improving destination image by altering perceived risk levels.
The literature states that the lower the perceived risk by tourists the more the destination will be perceived as familiar and attractive to tourists (San Martin & Del Bosque, 2008). Some scholars also asserted that insecurity and perceived risk directly affect destination image (Georges, 2010; Sonmez & Graefe, 1998; Qi, Gibson & Zhang, 2009). Other studies attempted to investigate the relationship between each of perceived (e.g. disaster risk, socio - psychological risk, health risk, financial risk) and destination image in both cognitive and affective image. For example, several (Hsu & Lin, 2006). physical risk perceived by tourists as a severe consequence during their traveling can significantly influence tourists’ subjective perception of the destination leading to confer higher overall perceived travel risk.Subsequently, the perceived risk would create a negative image of the destination. Moreover, (Lehto et al. 2008). pointed out that events of natural disaster, or perceived disaster risk, have a significant influence on tourists’ affective (feeling) responses and in turn develop negative destination image. A more recent study by (Chew & Jahari, 2014). has confirmed the relationship between perceived travel risk and destination image. More specifically, the findings presented two of three tested types of perceived risks: socio-psychological and financial riskswere relevant to Malaysian repeat tourists to Japan in reforming their destination image of the disaster-struck country. The author can assume that perceived risk has a negative correlation on all dimensions of destination image including cognitive, affective and overall dimensions in the context of medical tourism. Thus, the hypothesesare proposed:
Hypothesis 1: There is a direct negative relationship between risk and cognitive image perceived by medical tourists
Hypothesis 2: There is a direct negative relationship between risk and affective image perceived by medical tourists
Hypothesis 3: There is a direct negative relationship between risk and overall image perceived by medical tourists
According to (Tasci & Gartner,2007). the authors developed the multifaceted concept of destination image describing that destination image consists of a holistic image component (overall image) and an attribute component (cognitive and affective image) dominantly draws upon attributes through the formation of cognitive and affective images, while the combination of these images form the overall image. Moreover, it has for a long time been supported that cognitive and affective image are strongly associated in forming the overall image of the destination (Baloglu & McClearly, 1999; Beerli & Martin, 2004; Hosany & Uysal, 2006; Philips & Jang, 2008). Therefore, the study proposes the following hypothesis:
Hypothesis 4: There is a direct, positive relationship between cognitive image and overall image
perceived by medical tourists
Hypothesis 5: There is a direct, positive relationship between affective image and overall image
perceived by medical tourists
The following attempt in this study was to examine the role of overall destination image on medical tourists’ loyalty. It is important to examine the concept of image and its relation to the satisfaction obtained in order to determine visitors’ intentions to revisit and to recommend the destination (Bigné et al., 2001; Cai et al., 2004; Yoon & Uysal, 2005). Destination image is considered one of the key elements of marketing activities, particularly in loyalty. Literature considers image discretely approached, as a necessary antecedent of loyalty. Perceived destination image varies among consumers, and positive destination image would improve satisfaction. The research revealed that the role of destination image as an independent variable influenced consumer behaviors including before, during and after visiting a destination (Mohamad et al., 2012; Chen and Tsai, 2007; Bigne, Sanchez and Sanchez, 2001; Chen and Hsu, 2000; Schroeder, 1996; Ross, 1993). Several studies have asserted for the significant role of destination image in forming customers’ satisfaction as well as their loyalty (Ramseook- Munhurruna & Naidooa 2015; Chen & Tsai 2007; Prayag & Ryan, 2012). To support in this study, many researchers have confirmed the effect of destination image on consumer loyalty in the literature. It is undeniable that image seems to be a crucial factor deciding whether consumers will revisit a destination. Additionally, (Bosque & Martin,2008). have noted that the influence of image on customer loyalty must be noticed because a positive image of the destination is the main cause of tourists’ revisiting or recommending the destination to others. Numerous studies have indicated that the destination image with more attractive results in consumers’ revisits in the same destination. For example, (Li,2013). revealed that if the image is more positive, tourists are more likely to visit or revisit the destination. The positive relationship between image and loyalty has been highlighted in the study of (Bosque&Martin,2008). (Yoon & Uysal,2005). The research by (Mohamed et al. (2011), (Yossamorn & Phokha,2012). (Bigne et al. 2001). have also demonstrated the positive destination image perceived by consumers positively influence the willingness of travelers to revisit or recommend the destination. Therefore, the empirical studies presenting the positive relationship between destination image and consumer loyalty have suggested by many researchers (Hunt, 1975; Pearce, 1982; Tasci &Gartner, 2007; Um et al., 2006; Prayag & Ryan, 2012; Yosamorn & Phokha, 2012). In conclusion, the aim of the present study is to investigate the association of uniqueness of medical tourism destination’s image and consumer loyalty. This states that a desirable medical tourism destination image leads to medical tourist loyalty for a particular destination, or medical tourism destination in this study. As discussed earlier, this can assume that when medical tourists who perceived stronger positive destination image will result in improving their loyalty toward the destinationbecause it is viewed as having a positive image among other consumers, especially in credence products and services and this alone may provoke some amount of unwillingness to switch (Wang, 2010). Thus, the following hypotheses can be inferred from the above discussion:
Hypothesis 6: There is a direct positive relationship between overall image of medical tourism destination and medical tourists’ loyalty
Hypothesis 7: There is a direct positive relationship between cognitive image of medical tourism destination and medical tourists’ loyalty
Hypothesis 8: There is a direct positive relationship between affective image of medical tourism destination and medical tourists’ loyalty
METHODOLOGY
Data collection
The target population of the study was international tourists obtaining medical treatment in Phuket province, Thailand during a one-year period from October 2018 to October 2019.Based on the literature review, the reason the researcher selected Thailand as the main destination for this study because Thailand is a major hub of medical tourism in Asia. Most international medical tourists seek medical treatments from open-heart surgery to gender reassignment.According to the Ministry of Tourism and Sports website, Thailand had received 1.2 million medical tourists from other countries in 2017. The determination of sample sizes came up 400by using Taro Yamane’s formula with an error 5% and with a confidence coefficient of 95% (1967). Also, there are various rules-of-thumb in determining sample size requirements for Structural Equation Modeling (SEM). A common rule of thumb is that SEM studies should include a minimum sample size of 100, suggested by (Boomsma,1985). Similarly, (Hair et al. 2006). suggested that sample size of SEM should be ranged from 100 to 200. The same authors further noted that sample size should be large enough or at least 5 times of the number of parameters. Another rule-of-thumb proposed by (Bentler&Chou,1987). indicated that 5 or 10 observations per estimated parameter might be acceptable. The other rule-of-thumb noted that SEM studies should strive from 10 cases per variable (Nunnally, 1967). Therefore, the sample size of this study was 425 international medical tourists that met the mentioned criteria.
For data administration in this study, a self-administered survey questionnaire was decided to use a paper-based survey in the present study. The researcher contacted clinics/ hospitals in Phuket province, Thailand to get permission and assistance in conducting the research. The staffs at clinics helped to pass out the survey questionnaires to their international customers. The participants who qualify as medical tourists and are age 19 years old or older were passed out the questionnaires. If medical tourists agree, the staffs/ the researcher clearly communicated that participation is completely voluntary and no negative consequences would occur if individuals decided not to participate. Enveloped will be provided for the participants in order to submit questionnaires anonymously. The researcher collected the survey questionnaires from the staffs. Then returned surveys were reviewed by the researcher to ensure valid responses and data from valid questionnaires have been input into SPSS to be analyzed in generating a report.
Ethical concerns are important aspects of research while collecting data. As indicated by Jennings (2010), Ethics in research must be accounted for protecting the research participants’ rights and the standing in the scientific community (Jennings, 2010). The researcher must comply with moral and professional obligations when conducting the research, even if the research is conducted with participants who are unaware or unconcerned with the ethics of the study (Neuman, 2011). For these reasons, the cover letter was attached to the questionnaire in order to ensure the purpose of the study is consistently and honestly in alignment with the data collection. As suggested by (Creswell,2009), it is a need to establish trust and credibility between the researcher and the respondent while conducting the research. Furthermore, the respondent’s right to confidentiality, anonymity, voluntary participation, protection from harm, and protection from any action are considered very important issues when answering the research questions (Jennigns, 2010). This was detailed in the consent form that was completed by all respondents prior to their involvement in the research. Also, the researcher must act professionally when conducting the research and inform potential respondents about their rights and the research objectives before beginning their survey. Also, participation in the research was voluntary, and they can withdraw at any stage before submission of the research. Finally, protecting and confidentiality for the qualitative approach are needed during the process of coding the names and using pseudonyms for individuals and places to protect their identity (Creswell, 2009).
Study instrument
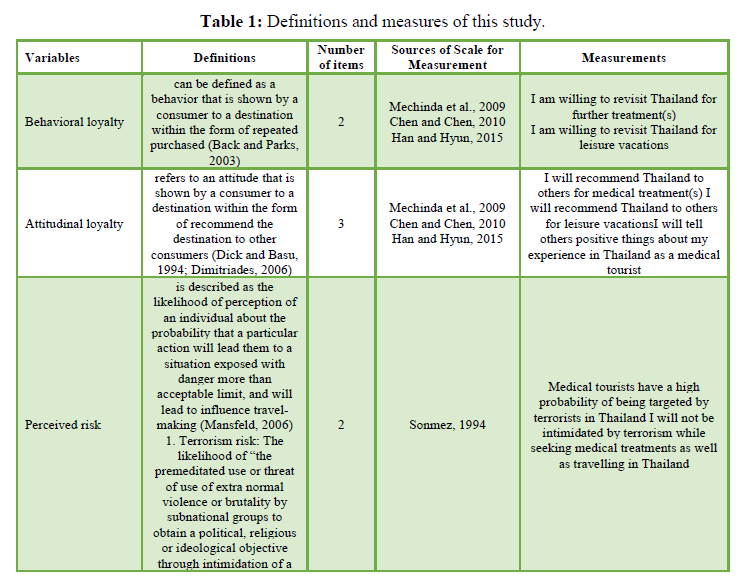
The questionnaire was used as the instrument of this quantitative study.The questionnaire was designed in English to cater to international medical tourists. Based on the review of related literature, the tool of the present study was developed regarding perceived risk, destination image concerning cognitive, affective and overall image, and destination loyalty. The questionnaire as the quantitative study instrument was developed based on prior studies employing well-established scales. The survey instrument contained scales measuring perceived risk, destination image and destination loyalty. The respondents' demographic was also included in the questionnaire. More specifically, the present study depends on three main dimensions of perceived risk relating to medical tourism including perception of terrorism risk, physical and health risk, and communication risk using risk scales developed by (Sonmez,1994). (Crooks et al. 2010). (Tsaur et al. (1997). (Roehl,1988), (Um&Crompton,1992), (Yamamoto& Gill, 1999). (Han & Weaver,2003). The perceived risk consisted of 10 items. All scales of three dimensions of perceived risk will be measured using five-point Likert scale items ranging from (1) strongly disagree to (5) strongly agree. The two items for terrorism risk was adapted to reflect medical tourists' behavior (e.g., Medical tourists have a high probability of being targeted by terrorists). Physical and health risk was measured with five items by asking how worried respondents are with injury and sickness because of conditions like laws and order, weather and hygiene during their traveling in Thailand for medical treatment(s) (e.g. There is a possibility of contracting the infectious disease in Thailand). The last dimension of risk was communication risk measuring with three items (e.g. It is important that people whom I meet speak English during my medical tourism in Thailand).
Destination image. The cognitive, affective and overall image was included in this study. The overall image of the destination is operationalized by selecting an attribute from the overall scale by Baloglu and McCleary (1999) that is relevant to the study context (e.g. Overall image of Thailand as a medical tourism destination). This scale was measured by mean of a five-point Likert scale with an anchor ranging from (1) strongly disagree to (5) strongly agree. Affective image of the destination was operationalized by using a four-item bipolar scale developed by Russell and Pratt (1980). The scale is measured by a five-point semantic differential scale including 1=sleepy and 5= Arousing, 1= Gloomy and 5=Exciting, 1=Unpleasant and 5=Pleasant, and 1=Distressing and 5=Relaxing. And cognitive image developed by Beerli and Martin, 2004 and Bologlu and McCleary, 1999 was operationalized by using a five-point Likert scale ranging from (1) strongly disagree to (5) strongly agree Table 1.
Destination loyalty. Loyalty in this study includes both behavioral and attitudinal loyalty. In other words, destination loyalty is measured by asking respondents their intention to revisit as well as the intention to recommend the destination with a scale developed by (Mechida etal.2009). (Chen,2010). (Han & Hyun,2015). The five-item scale (e.g., Intention to revisit the destination for further medical treatment(s)) is measured using a seven-point Likert scale ranging from (1) strongly disagree to (7) strongly agree.

Data analysis
The Statistical Package for Social Sciences (SPSS) and Analysis of Moments Structure (AMOS 23.0) software were used for the analysis in this study.SPSS was used for generating the descriptive and inferential statistics while AMOS was used to conduct a two-stage structural equation modeling (SEM) procedure, as suggested by (Anderson & Gerbing,1988). in order to test the hypothesized relationships. The total of 800 questionnaires were distributed, 452 usable samples were obtained. The author eliminated those with missing data, as recommended by (Hair et al., 1998; Tabachnick & Fidell, 2001). Therefore, 425 were used for data analysis, indicating a 53.1 % response rate.
RESULTS
Respondents profiles
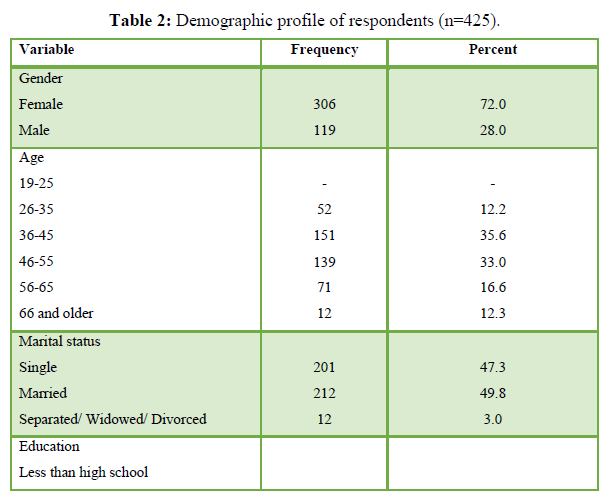
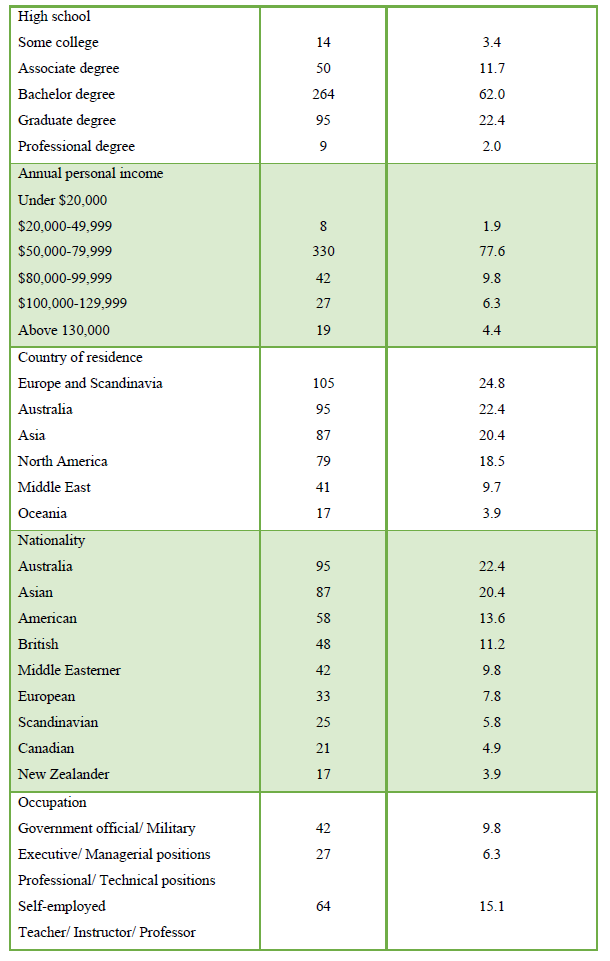
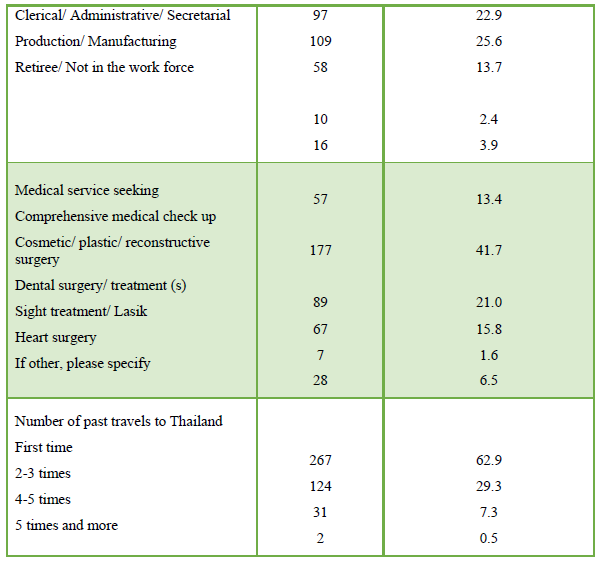
While about 72 percent of the medical tourists were female, 28 percent were male. The majority of international medical tourists, or 35.6 percent were 36-45 years old as well as 47.3 percent were single. For education, the majority of international medical tourists, or about 62 percent earned a bachelor degree. Additionally, the majority of participants, or about 78 percent had annual income between 50,000-79,999. Most of them came from Europe and Scandinavia (24.88%), followed by Australia (22.44%), Asia (20.48%), North America (18.54), Middle East (9.76%) and Oceania (3.90%), respectively. Similarly, 26.34 percent of them were Australian and New Zealander, followed by European and Scandinavian (24.88%), Asian (20.48%), American and Canadian (18.54%), Middle Easterner (Arab-9.76%), respectively. For occupation, most of them or 25.6 percent were teacher/ instructor/ professor, while 25.6 percent while the following was self-employed (or 22.9%), professional/ technical position (15.1%) and clerical/ administrative/ secretarial (13.7%). Moreover, most of them or 63 percent had traveled to Thailand for medical treatment for first time. Finally, the majority of them or 41.70 percent has sought for cosmetic/ plastic/ reconstructive surgery, followed by dental surgery, or treatment (21.05%) Table 2.
Measurement model analysis
The values of skewness and kurtosis were examined before proceeding to dataanalysis. The findings found that all constructs presented a normal distribution withskewness and kurtosis values with the range of -2 to +2, as suggested by (Tabachnick &Fidell,2001). This study mainly used SPSS and AMOS 23 to analyze the data.
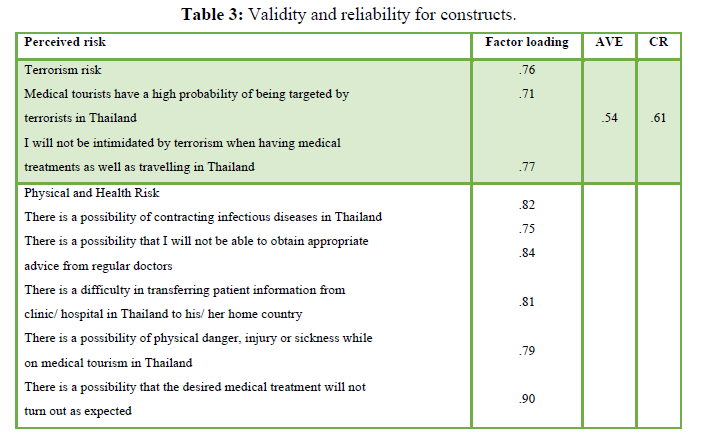
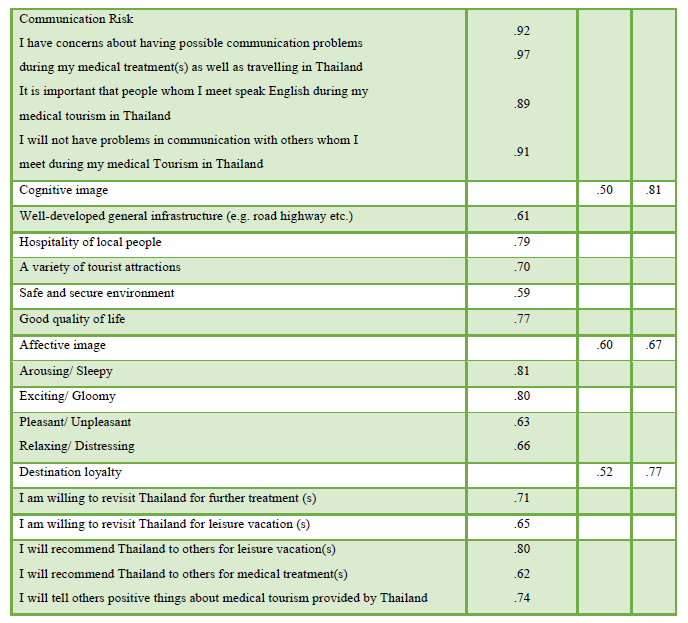
At the initial stage, a measurement model was conducted and then the structural model was estimated using the maximum likelihood estimation method. Thefindings of the Confirmatory Factor Analysis (CFA) on these 22 items showed a good fit to the data (x2 =255, df=160, p<0.001, CFI=0.915, GFI=0.930 RMSEA=0.089). Therefore, the measurement model was used for further analysis. The composite reliability was computed and values were all acceptable, exceeding the suggested cut-off of 0.60 (Bagozzi & Yi, 1988). All standardized factor loadings emerged fairly high and significant, ranging from 0.61 to 0.92. This convergence of the indicators with the appropriate underlying factors is suggested by Anderson & Gerbing (1988). After that, the average variance extracted (AVE) values for each construct were all above 0.50 (Fornell & Larcker, 1981). In overall, the findings presented strong evidence of reliability, and validity of the measures.
Cronbach’salpha values of the constructs in the study ranged from .74-.91, exceeding the minimumthreshold of .70 (Hair et al., 1988). Thus, it indicated internal consistency in measurementitems. Additionally, construct reliability (CR) and average variance extracted (AVE) were calculated in order toinvestigate the convergent validity. The square root of the AVE valueswas greater than the correlation coefficients among the research constructs. Thus, thediscriminant validity was evident in this study, as suggested by Fornell and Larcker (1981).
Finally, the multicollinearity was checked and a variance inflation factor (VIF) determines how the independent variables are related to one another. The present study presented the VIF values ranging from 1.46 to 1.73. Therefore, the regression model is acceptable to determine the effect of independent variables on the dependent variables, as suggested by the cutoff threshold of VIF values at 10 (maximum) as the acceptability of multicollinearity (Hair et al., 2006) Table 3.
Hypothesis testing
The structural model was tested though a structural equation modelling (SEM) usingAMOS. The overall model fit statistics show that the model was satisfied to represent the hypothesized constructs (X2 = 285, p<0.001, CFI=0.951, GFI=0.910, RMSEA=0.039). The structural results of the proposed model are depicted in Figure 2.
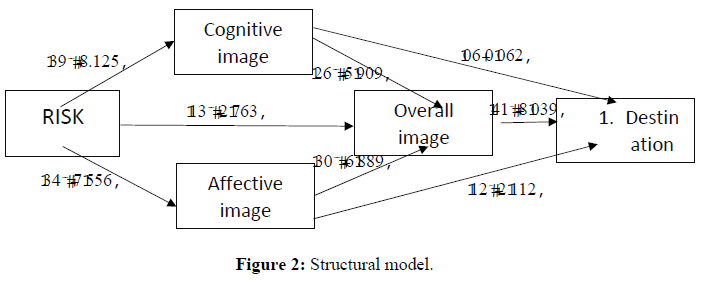
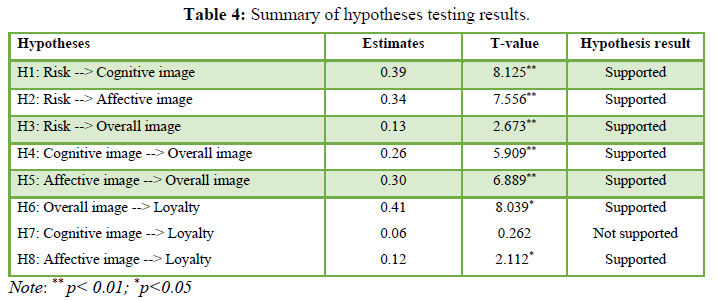
Then, the hypothesized relationships were tested and were presented the empirical findings from theSEM. Almost the paths proposed in the structural model were statistically significant and ofthe expected positive direction. Therefore, sevenhypotheses were supported.More specifically, Hypothesis 1 and 2 were tested and the finding indicated that risk perceived by medical tourists significantly and positively affected their perceived destination image including cognitive (B=.39, p<0.01), affective (B=.34, p<0.01) and overall (B=.13, p<0.01) dimensions. The resultstherefore supported Hypothesis 1, 2 and 3.Perceived risk accounted for 53.4%, 56.0% and 48.0% of the total variance in cognitive, affective and overall dimensions of image.Subsequently, Hypothesis 4 and 5 were tested and the results revealed that both cognitive (B=.26, p<0.01) and affective (B=.30, p<0.01) dimensions of destination image perceived by medical tourists significantly and positively affected overall image perceived by medical tourists. Thus,this finding supported Hypothesis 4 and 5. Cognitive and affective dimensions of image explained about 52.7% and 54.3% of the variance in overall image. Consequently, Hypothesis 6, 7 and 8 were tested. The finding presented that two dimensions of destination image including affective (B=.12, p<0.05) and overall (B=.41, p<0.05) image exerted a significant influence on medical tourist loyalty and thus Hypothesis 6 and 8 were supported.Affective and overall dimensions of image accounted for 51.5% and 50.7% of the total variance in destination loyalty including intention to revisit and intention to recommend to others. However, the result showed that cognitive image was not significantly and positively affect medical tourist loyalty. Thus, Hypothesis 7was not supported. The summary of the results is presented in Table 4.
The author examined the indirect impact of study variables. Findings revealed that risk significantly and indirectly affected overall image through cognitive (β risk -->cognitive image --> overall image = .31, p <.05) and affective (β risk -->affective image --> overall image = .21, p <.01) dimensions of image. Additionally, results from the SEM presented that risk has a significant and positive indirect impact on destination loyalty (β risk -->affective image --> destination loyalty = .58, p <.01; β risk -->overall image --> destination loyalty = .54, p <.01) through affective and overall dimensions of destination image but not through cognitive image. Thus, affective and overall dimensions of destination image played a significant mediating role in the conceptual model.
CONCLUSION AND IMPLICATIONS
Despite the rapid growth in medical tourism, limited studies mentioned about the role of risk and destination image in explaining international medical tourists’ loyalty. The purpose of this study was to develop and evaluate a theoretical structural model for establishing medical tourists’ loyalty by integrating two main factors, namely risk and destination image affecting medical tourists’ intention to revisit the destination as well as intention to recommend the destination to others. The findings of this study went on to successfully incorporate risk and destination image into the model explicating medical tourists’ loyalty in terms of intention to repurchase and intention to recommend to others.
To begin with, this study contributes to the very limited literature on the relationship between risk and destination image in the context of medical tourism. The findings supported the hypotheses that risk perceived by international medical tourists was negatively related to destination image including affective, cognitive and overall dimensions that perceived by them. This was consistent with several previous studies. The literature indicated that the lower the perceived risk by tourists the more the destination will be perceived as familiar and attractive to tourists (San Martin & Del Bosque, 2008). Some scholars also asserted that insecurity and perceived risk directly affect destination image (Georges, 2010; Qi, Gibson & Zhang, 2009; Sonmez & Graefe, 1998). Other studies attempted to investigate the relationship between each of perceived risk (e.g. disaster risk, socio- psychological risk, health risk, financial risk) and destination image in both cognitive and affective dimensions. For example, several (Hsu & Lin, 2006). physical risk perceived by tourists as a serious consequence during their traveling can significantly influence tourists’ subjective perception of the destination leading to confer higher overall perceived travel risk. Subsequently, the perceived risk would create a negative image of the destination. Moreover, (Lehto et al. 2008). pointed out that events of natural disaster, or perceived disaster risk, have a significant influence on tourists’ affective (feeling) responses and in turn develop negative destination image. A more recent study by (Chew & Jahari, 2014). has confirmed the relationship between perceived travel risk and destination image. Therefore, it can be indicated that perceived risk has a negative correlation on all dimensions of destination image including affective, cognitive and overall dimensions in the context of medical tourism.
The following findings confirmed the existing body of knowledge in the context of tourism. The subsequent hypotheses were supported on a direct positive relationship between the cognitive image as well as affective image, and overall image of a destination perceived by international medical tourists. These results are consistent with previous studies stating that destination image consists of a holistic image component (overall image), and an attribute component (cognitive and affective image) dominantly draws upon attributes through the formation of cognitive and affective images, while the combination of these images form the overall image, as noted by (Tasci & Gartner,2007). Moreover, it has for a long time been supported that cognitive and affective image are strongly associated in forming the overall image of the destination (Baloglu & McClearly, 1999; Beerli & Martin, 2004; Hosany & Uysal, 2006). Therefore, the researcher stated that both cognitive and affective image have a positive correlation on an overall image in the field of the medical tourism industry.
Finally, the findings between destination image in terms of affective, cognitive and overall dimensions were analyzed. Determining visitors’ intentions to revisit and to recommend the destination has been regarded as the important relationship in the literature (Bigné et al., 2001; Cai et al., 2004; Yoon & Uysal, 2005). Several studies have asserted for the significant role of destination image in forming customers’ loyalty (Ramseook-Munhurruna & Naidooa 2015; Chen & Tsai 2007; Prayag & Ryan 2012). The results supported the hypothesis in the fact that image perceived by international medical tourists positively related to their loyalty. This is in line with several previous studies confirming the effect of destination image on consumer loyalty. The image seems to be a crucial factor deciding whether consumers will revisit a destination. Additionally, (Bosque & Martin,2008). have noted that the influence of image on customer loyalty must be noticed because a positive image of the destination is the main cause of tourists’ revisiting or recommending the destination to others. Numerous studies have indicated that the destination image with more attractive results in consumers’ revisits in the same destination. For example, (Li, 2013). revealed that if the image is more positive, tourists are more likely to visit or revisit the 28 destination. The positive relationship between image and loyalty has been highlighted in the study of (Bosque & Martin, 2008). (Yoon & Uysal, 2005). The research by (Mohamed, et al. 2011), (Yossamorn & Phokha, 2012). (Bigne et al. (2001) have also demonstrated the positive destination image perceived by consumers positively influence the willingness of travelers to revisit or recommend the destination. Moreover, the empirical studies presenting the positive relationship between destination image and consumer loyalty have suggested by many researchers (Hunt, 1975; Pearce, 1982; Tasci & Gartner, 2007; Um et al., 2006; Prayag & Ryan, 2012; Yosamorn & Phokha, 2012). For these reasons, the researcher has confirmed that there was a direct positive relationship between overall image and loyalty in the context of medical tourism.
An understanding of how medical tourism destination loyalty can be sustained and enhanced in successful destination planning and management in an increasingly saturated market. The findings of this study may contribute to integrating as well as creating value-added medical tourism destinations to achieve greater destination competitiveness. This section provided several useful implications drawn from the results of the study in both theoretical and practical implications for medical tourism industry.
From a theoretical standpoint, loyalty is of considerable interest to both practitioners and academics in the field of hospitality management. The findinds of this study has contributed to the body of knowledge on perceived risk, image and destination loyalty in several ways. Although a number of studies have acknowledged the model of medical tourism destination loyalty, no studies has been done to integrate perceived risk as a main construct. The present study confirmed a proposed model which integrated three mentioned constructs based on a review of previous studies. Therefore, the result of this study is expected to be extending the understanding of perceived risk, image and destination loyalty in the context of medial tourism industry. Additionally, the results of relationships between variables in the study add new knowledge to the body of literature on medical tourism industry. The relationship between each of perceived risk and destination image has been found in the literature of tourism industry, however studies less investigated in existing literature on medical tourism. The current study thus proposed and confirmed the significant impact of perceived risk on image in terms of cognitive, affective and overall dimensions. Finally, the results of this study provided evidence that two dimensions of image including affective and overall image have a positive impact on destination loyalty. In other words, while medical tourists hold the higher evaluation of the affective and overall image, their level of loyalty in both intentions to revisit and intention to recommend to others will be high.
From a practical standpoint, the stakeholders in any destination need a better understand of factors influencing international medical tourists in building their loyalty in terms of intention to revisit and intention to recommend destination to others. The findings of this study provide useful information for medical tourism destination marketers to develop more effective strategies related to reduce consumer’ perceived risk as well as to develop destination image, and loyalty. More specifically, a destination with a positive perceived risk has a great chance of being positive perceived image by medical tourists which in turn leads to return to the destination as well as to recommend the destination to others. Additionally, the finding of this presented that affective image and overall image positively affected medical tourists’ destination loyalty. Destination marketers should reinforce the feeling and emotional experiences of medical tourists or affective image rather than cognitive dimension or the attributes of the destination in their promotion efforts. Finally, destinations can develop a highly effective advertising campaign in order to reduce risk perceived by medical tourists. As the findings of this study, risk had a significant impact on destination image. Likewise, medical tourists’ perception of risk significantly affected their perceived destination image.
LIMITATIONS AND FUTURE RESEARCH RECOMMENDATIONS
This study integrated the concepts of risk and image in the model of medical tourist loyalty.
There are several limitations in this study in order to consider in future research. The sample of this study was international medical tourists from multiple countries around the world. To get better understand of medical tourists’ loyalty in each country, future research should focus on medical tourists from a specific country or continent. Moreover, generalizations cannot be made from the findings ofthe present study to other geographic areas or locations because the data were collected innclinics that located in Phuket in Thailand. For future research, a more research design according to a wider sampling should be uncluded so as to minimize sampling limitations. Furthermore, the proposed model in this study was not designed to include other important variables in influencing international medical tourists’ loyalty. Future research should integrate other important variables into the conceptual model in order to provide more information in the context of medical tourism.
- Archer, B., Cooper, C., & Ruhanen, L. (2005). The positive and negative impacts of tourism. In Theobald WF Global Tourism 79-102.
- Awadzi, W. & Panda, D. (2005). Medical Tourism Globalization and Marketing of Medical Services. The Consortium Journal of Hospitality and Tourism 11(1), 75-80.
- Bagozzi, R. and Yi, Y. (1988). On the Evaluation of Structural Equation Models. Journal of the Academy of Marketing Sciences 16, 74-94.
- Baloglu, S. & McCleary, K.W. (1999). A model of destination image formation. Annals of Tourism Research 26, 868-897.
- Baloglu, S., & Mangaloglu, M. (2001). Tourism destination images of Turkey. Egypt Greece and Italy as perceived by USbased tour operators and travel agents. Tourism Management 22, 1-9.
- Beerli, A., & Martin, J.D. (2004). Tourists’ characteristics and the perceived image of tourist destinations: A quantitative analysis A case study of Lanzarote Spain. Tourism Management 25, 623-636.
- Bigne, J.E., Sanchez, M. I., & Sanchez, J. (2001). Tourism image evaluation variables and after purchase behavior Interrelationship. Tourism Management 22, 607-616.
- Bookman, M.Z., & Bookman, K.R. (2007). Medical Tourism in Developing Countries New York Palgrave Macmillan.
- Caballero Danell, S., & Mugomba, C. (2006). Medical Tourism and its Entrepreneurial Opportunities A conceptual framework for entry into the industry. Goteborg University.
- Calderon, J. & Gonzales, E.C. (1993). Methods of Research and Thesis Writing. Manila National Bookstore Inc.
- Carr, N. (2001). An exploratory study of gendered differences in young tourists’ perception of danger within London. Tourism Management 22, 565-570.
- Carrera, P., & Lunt, N. (2010). A European perspective on medical tourism the need for a knowledge base. International Journal of Health Services 40(3), 469-484.
- Carrera, P.M. & Bridges, J.F.P. (2006). Globalization and healthcare Understanding health and medical tourism. Expert Review of Pharmacoeconomics & Outcomes Research 6(4), 447- 454.
- Chen, J.S., Prebensen, N., & Huan, T.C. (2008). Determining the motivation of wellness Travelers. Anatolia An International Journal of Tourism and Hospitality Research 19(1), 103-115.
- Chen, C.F., & Tsai, D.C. (2007). How destination image and evaluative factors affect behavioral intentions. Tourism management 28(4), 1115-1122.
- Chew, E.Y.T., & Aqilah, J.S. (2014). Destination image as a mediator between perceived risks and revisit intention A case of postdisaster Japan. Tourism Management 40, 382-393.
- Chi, C.G., & Qu, H. (2008). Examining the structural relationships of destination image tourist satisfaction and destination loyalty An integrated approach. Tourism Management 29, 624-636.
- Chon, K.S. (1990). The role of destination image in tourism A review and discussion. TourismManagement 45(2), 2-9.
- Chon, K.S. (1989). The understanding recreational traveler’s motivation, attitude and satisfaction. Tourism Review 44(1), 3-7.
- Churchill, G.A., & Brown, T.J. (2004). Basic Marketing Research. Mason OH Thompson SouthWestern.
- Connell, J. (2006). Medical tourism Sea sun sand and surgery. Tourism Management 27, 1093-1100.
- Coshall, J.T. (2003). The threat of terrorism as an intervention of international travel flows. Journal of Travel Research 42(1), 4-12.
- Connell, J. (2006). Medical tourism Sea sun sand and surgery. Tourism Management 27(6), 1093-1100.
- Creswell, J.W. (2014). Research design international student edition Los AngelesSage.
- Crooks, V.A., Turner, L., Snyder, J., Johnston, R., & Kingsbury, P. (2011). Promoting medical tourism to India messages images and the marketing of international patient travel. Research Support NonUSGovt. Social Science Media 72(5), 726-732,
- Crooks V., Kigsbury P., Snyder J. and Jonston R., (2010). What is known about the patients experience of medical tourism A scoping review. Journal of health services research 10, 266.
- del Bosque, I.R. & Martin, H.S. (2008). Tourist Satisfaction a CognitiveAffective Model. Annals of Tourism Research 35, 551-573.
- Dimitriades, Z.S. (2006). Customer satisfaction, loyalty and commitment in service organizations Some evidence from Greece. Management Research News 29(12), 782 - 800.
- Dowling, G.R. & Staelin, R. (1994). A model of perceived risk and intended riskhandling activity. Journal of consumer research 21, 119-134.
- Echtner, C.M., & Ritchie, J.R.B. (1993). The measurement of destination image an empirical assessment. Journal of Travel Research 31, 21-64.
- El Taguri, A. (2007). Medical tourism and the Libyan national health services. Libyan Journal of Medicine 2, 1-4.
- Ettinger, W. H. (1998). Consumer perceived value the key to a successful business startegy in the healthcare market place. Journal of American Geriatrics Society 46(1), 111-113.
- Fakeye, P.C., & Crompton, J.L. (1991). Image differences between prospective, first- time, and repeat visitors to the lower Rio Grande Valley. Journal of Travel Research 30, 10-16
- Forgione, D. A., & Smith, P. C. (2007). Medical tourism and its impact on the US health care system. Journal of Health Care Finance 34(1), 27-35.
- Fornell, C., & Larcker, D.F. (1981). Evaluating structural equation models with unobservable variables and measurement error. Journal of Marketing Research 18(1), 39-50.
- Gahlinger, P.M. (2008). The Medical Tourism Travel Guide Your Complete Reference to Top-Quality Low-Cost Dental Cosmetic Medical Care & Surgery Overseas. Sunrise River Press.
- Gallarza, M. G., & Saura, I. G. (2006). Value dimensions, perceived value, satisfaction and loyalty an investigation of university students travel Behavior. Tourism Management 28, 437-452.
- GarciaAltes, A. (2005). The development of health tourism services. Annals of Tourism Research 32(1), 262-266.
- Gupta, A., & Chen, I. (1995). Service quality Implications for management development. International Journal of Quality & Reliability Management 12(7), 28-35.
- Gupta, H.D. (2004). Medical tourism and public health. People s Democracy. 27(19). Available online at: http://pd.cpim.org/2004/05092004_snd.htm.
- Gunn, C.A., & Var, T. (2002). Tourism Planning London Routledge.
- Hall, C.M. (2005). Tourism Rethinking the social science of mobility. Harlow Pearson.
- Hall M. & James M., (2011). Medical tourism Emerging biosecurity and nosocomial issues Tourism review 66(12), 118-126.
- Hansen, F. (2008). A revolution in healthcare medicine meets the marketplace. Public Affairs Review 59(4), 43-45.
- Hair, J., Black, W., Babin, B., Anderson, R., & Tatham, R. (2006). Multivariate data analysis Uppersaddle River NJ Pearson Prentice Hall.
- Hair, J.F., Anderson, R.E., Tatham, R.L., & Black, W.C. (1988). Multivariate data analysis Upper Saddle River Prentice Hall.
- Henderson, J.C. (2004). Paradigm shifts National tourism organizations and education and healthcare tourism: The case of Singapore. Tourism and Hospitality Research 5(2), 170-180.
- Hu, Y., & Ritchie, J.R.B. (1993). Measuring destination attractiveness, A contexual approach. Journal of travel Research, 32, 25 - 32.
- Huff-Rousselle, M.C., Shepherd, R., Cushman, Imrie, J., & Lalta, S. (1995). Prospects for HealthTourism Exports for the English-Speaking Caribbean Washington DC World Bank.
- Heung, V.C.S., Kucukusta, D., & Song, H. (2010). A Conceptual Model of Medical Tourism Implications for Future Research. Journal of Travel & Tourism Marketing 27(3), 236-251.
- Hosany, S, Ekinci, Y & Uysal, M. (2007). Destination image and destination personality International Journal of Culture. Tourism and Hospitality Research 1(1), 62-81.
- Hosany, S., &Prayag, G. (2013). Patterns of tourist’s emotional responses satisfaction and intention to recommend. Journal of Business Research 66(6), 730-737.
- Hsu, T.H., & Lin, L.Z. (2006). Using fuzzy set theoretic techniques to analyze travel risk an empirical study. Tourism Management 27(5), 968-981.
- Hurley, J.A. (1988). The hotels of Rome Meeting the marketing challenge of terrorism. The Cornell Quarterly 29, 71-79.
- Hutchinson, M., Vickers, M., Jackson, D., & Wilkes, L. (2005). Like wolves in a pack Stories of predatory alliances of bullies in nursing. Health Care Management Review 30, 331-336.
- Keckley, P. H. & Underwood, H. R. (2008), Medical Tourism Consumers in Search of Value Washington Deloitte Center for Health Solutions.
- Lee, J.W., & Brahmasrene, T. (2013). Investigating the influence of tourism on economic growth and carbon emissions Evidence from panel analysis of the European Union. Tourism Management 38, 69-76.
- Lee, J., Graefe, A.R., & Burns, R. C. (2004). Service quality, satisfaction and behavioral Intention among forest visitors. Journal of Travel & Tourism Marketing 17(1), 73 -82.
- Lepp, A., & Gibson, H. (2003). Tourist roles perceived risk and international tourism. Annals of Tourism Research 30,606-624.
- Lunt, N., & Carrera, P. (2010). Medical tourism Assessing the evidence on treatment abroad. Maturitas 66(1), 27-32.
- Mitchell, V.W. (1999). Consumer perceived risk conceptualizations and models. European Journal of Marketing 33(1)163-196.
- Newman, B. Y. (2006). Medical tourism. Journal of the American Optometric Association 77(12), 581.
- O'Brien, L. & Jones, C. (1995). Do rewards really create loyalty? Harvard Business Review, MayJune, 5-82.
- Oliver, R. L., & DeSarbo, W.S. (1988). Response determinants in satisfaction judgments. Journal of Consumer Research 14, 495-508.
- Oliver, R.L. (1997). Satisfaction: A Behavioral Perspective on the Consumer. Boston McGrawHill.
- Olsen, S.O. (2002). Comparative evaluation and the relationship between quality satisfaction, and repurchase loyalty. Journal of the Academy of Marketing Science 30(3), 240-249.
- Parasuraman, A. Zeithaml, V.A. & Berry, L.L. (1985). A conceptual model of service quality for future research. Journal of Marketing 49(4), 41-50.
- Parasuraman, A. Zeithaml, V.A. & Berry, L.L. (1988). SERVQUAL A multi-item scale for measuring consumer perception of service quality. Journal of Retailing 64, 12-40.
- Phillips, W. & Jang, S. (2008). Destination image and tourist attitude. Tourism Analysis 13, 401-11.
- Prayag, G., & Ryan, C. (2010). The relationship between the push and pull factors of a tourist destination the role of nationality an analytical qualitative research approach. Current Issues in Tourism, 14(2), 121-143.
- Reichheld, F.F. & Sasser, E. (1990) Zero Defections Quality Comes to Services. Harvard Business Review 68, 105-111.
- Roehl, W., & Fesenmaier, D. (1992). Risk perceptions and pleasure travel an exploratory analysis. Journal of Travel Research 2, 17–26.
- Ramirez de Arellano, A. (2007). Patients without borders the emergence of medical tourism. International Journal of Health Services Planning Administration Evaluation 37(1),193-198.
- Singh, P.K. (2008). Medical tourism. New Delhi India Kanishka Publishers.
- Roselius, T. (1971). Consumer rankings of risk reduction methods. Journal of Marketing 35, 56-61.
- So ̈nmez, S. (1998). Tourism, terrorism and political instability. Annals of Tourism Research 25, 416-456.
- Tam, J. L. M. (2000). The effect of service quality, perceived value and customer satisfaction on behavioral intentions. Journal of Hospitality & Leisure Marketing 6(4), 31-43.
- Tasci, A. D. A. (2006). Visit impact on destination image. Tourism Analysis 11, 297-309.
- Tasci, A. D. A. & Gartner, W. C. (2007). Destination Image and Its Functional Relationship. Journal of Travel Research 45, 413-425.
- Tasci, A. D. A. & Kozak, M. (2006) Destination brands vs destination image Do you know what we mean. Journal of Vacation Marketing 12, 299-317.
- Tremblay, P. (1989). Pooling international tourism in Western Europe. Annals of Tourism Research 16, 477-491.
- Turner, L. (2007). First World Health Care at Third World Prices Globalization. Bioethics & Medical Tourism BioSocieties 2(3), 303-325.
- Turner, L. (2008). Crossborder dental care Dental tourism and patient mobility. British Dental Journal 204(10), 553-554.
- Teh, I., & Chu, C. (2005). Supplementing growth with medical tourism. Asia Pacific Biotech News 9 (8), 306-311.
- Qi, C. X., Gibson, H. J., & Zhang, J. J. (2009). Perceptions of risk and travel intentions the case of China and the Beijing Olympic Games. Journal of Sport & Tourism 14(1)43-67.
- UNWTO. (2016). UNWTO tourism highlights World Tourism Organization. Available online at: http://fac.ksu.edu.sa/sites/default/files/tourism_highlights_2016-_unwto.pdf
- Um, S., Chon, K., & Ro, Y. H. (2006). Antecedents of revisit intention. Annals of tourism research 33(4), 1141-1158.
- Weaver, C. (2008) Boom times for Asia plastic surgery trips. The Sunday Mail Gold Coast Australia.
- White, C. (2005). Destination Image To see or not to see Part II. International Journal of Contemporary Hospitality Management 17, 191-196.
- WTTC. (2015). Global talent trends and issues for the travel & tourism sector. London United Kingdom World Travel & Tourism Council. Available online at: https://www.wttc.org/-/media/382bb1e90c374262bc951226a6618201.ashx
- Wu, C.W. (2016). Destination loyalty modeling of the global tourism. Journal of Business Research 69(6), 2213-2219.
- Yoon, Y. & Uysal, M. (2005). An Examination of the Effects of Motivation and Satisfaction on Destination Loyalty A Structural Model.Tourism Management 26, 45-56.
- York, D. (2008). Medical tourism the trend toward outsourcing medical procedures to foreign countries. The Journal of Continuing Education in the Health Professions 28, 99-102.
- Youngman, I. (2007). Medical Tourism. The Worldwide Business Guide. Available online at: http://www.researchandmarkets.com/reports/569409/medical_tourism
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6
-
Table 7
-
Table 8












