
5904
Views & Citations4904
Likes & Shares
Background: The “hearing of voices” has been considered, since ancient times, as something characteristic of human nature, integrated in culture and with a meaning. However, with the medicalization of the phenomenon in the 18th century, this semantic character was lost due to the negative and pathological framing of hallucinations. Since the mid-twentieth century, the rise of the community care and recovery model centered on the person and the demands made by user movements have contributed to a change of direction in the conceptualization and approach to “listening to voices”.
Results: Attention to the hallucinatory experience must consider the personal experiences, previous traumatic events and the social and historical context of each individual.
People listeners attribute different meanings to their voices, and a great deal of cross-cultural variability has been documented with respect to the meanings attributed.
The VHG can provide significant help in identifying and coping with voices and can serve as a turning point in the life history of voice hearers.
Conclusions: The experience of hearing voices should not be considered as an isolated and meaningless psychiatric symptom.
The listening of voices can be approached beyond the symptom.
The contributions made by the Hearing Voices Movement have contributed to recontextualize the conceptualization and approach to the hallucinatory experience.
The Voice Hearers Groups can offer an alternative to current models of recovery and empowerment of users.
However, the HVM has operated outside of traditional psychiatric systems to help, among others, those who suffer from distressing voices, by creating self-help hearing voices groups along with activism. This has had both advantages and disadvantages. One of the disadvantages, by its very nature since the HVM has opposed the traditional thinking of biological psychiatry. And it is that knowledge, thinking, and ability to empower and help people with problematic voices has not been readily accessible within psychiatry. This has been counteracted by a readiness and interest to invite non-voice hearers into its movement which has increasingly inspired professionals and laypeople alike to engage with the HVM. This has allowed movement knowledge to enter mainstream psychiatry and influence traditional disease-based thinking, opening up other possibilities.
The authors of the work have done a theoretical review spanning from ancient times to the present day looking at the phenomenon of hearing voices. By looking through the lens of history, they show how hearing voices has been viewed differently over time, from when it was considered, for example, as a gift or viewed in a spiritual way, to the present day when traditional western psychiatry has chosen to consider this phenomenon as an illness.
In their theoretical review, the authors are able to point out by the evidence collected that it is clear that viewing hearing voices as a “meaningless psychiatric symptom” removes the possibility of unfolding the richness that is part of the human experience of hearing voices. This interest in exploring the multifaceted aspects of voice hearing comes about because of the HVM’s desire to invite non-voice hearers to listen and explore together in dialogue. When this happens as in this article, the knowledge garnered can be disseminated into the psychiatric system inspiring others to move away from a simplified reductionist approach to mental illness and listening to voices. This opens up other possibilities for supporting those with problematic voices who turn to psychiatry in search of help.
The authors show evidence that voice hearing groups are useful, that they can offer an alternative to current models of recovery and empowerment, and that treatment strategies go beyond a biological approach.
The authors’ review makes me think of an experience I had many years ago when I started in a new psychiatric ward as a nurse. I was shown around by the ward nurse who also introduced me to the patients.
She introduced me to a young man whom she said was very ill with severe schizophrenia as he believed he was receiving messages from the dead.
A week passed, maybe two and then one day this same nurse rushed into the office and said today she could absolutely not stay late, and someone asked her why. She said she had booked an appointment with a clairvoyant who was going to get in contact with her dead father. I remember thinking how strange this psychiatric world is. On the ward there was a young man who was considered crazy because he heard the voices of the dead, but outside the hospital the staff was willing to pay money to someone who listened to the dead.
Currently, this blindness to such a discrepancy is increasingly reduced by addressing the nuanced complexities surrounding the phenomenon of voice hearing, as the authors discuss in this work.
They explore the many more holistic approaches that mainstream psychiatry purports to offer to those suffering from hallucinations.
These changes would not occur if HVM had not continued over the years to question current paradigms, insist through activism for change, and offer safe spaces for voice hearers to gather and explore their voices.
THE EXPERIENCE OF LISTENING TO VOICES
The “listening to voices" has its roots in the human being history itself. In mythology and particularly in Greek mythology, rich in images and symbolic references to human existence, there is a mythological reference to listening to voices, the Myth of Asclepius (God of Medicine). According to the myth, Asclepius acquired great skill, and practiced medicine based on healing plants whose success in the “recovery” of the sick, caused many sanctuaries to be erected in his honor in different areas of Greece. In these temples and sanctuaries, patients were allowed to rest and sleep near the gambling halls where prophetic dreams took place. According to the myth, it was believed that, during those stays in the “abaton” of the temples and sanctuaries, patients could feel the presence of Asclepius and "hear" his advice and remedies.
Socrates said: “You have often heard me say, in many places, that I feel the influence of some god and some genius upon me. It is a voice which began to show itself to me in my childhood, and which, whenever it is heard, tries to turn me away from what I want to do” (Daimon).
In ancient times, hallucinations were culturally integrated experiences, possessing great meaning, and their content conveyed messages about the subject or the world [1]. With the medicalization of the phenomenon in the 18th century, this semantic character was lost. The classifications of the time considered hallucinations as independent diseases. The truth is that until the 19th century they were not considered as "symptoms", that is, as behavioral fragments common to various diseases. There are numerous classical references to phenomena that could be included under the term "hallucination". Before Christ, evidence of a limited concept of hallucination can be found in some biblical passages. It has also been pointed out that in the Greek world, hallucinations may have been the norm, as they lacked the concept of “conscience” and attributed their own thoughts to gods and spirits. Reports of hallucinatory experience can be traced back to the earliest religious figures (Moses, Jesus Christ). In the Judeo-Christian culture, listening to voices was considered a normal way of making decisions. Some biblical passages refer to it. Thus, in the Gospel of John, “My sheep hear my voice, I know them and they follow me” (John. 10:14, 27).
The first Christian thinkers studied, in a systematic way, hallucinatory experiences. Authors such as Augustine of Hippone, Thomas of Aquino and Teresa of Avila analyzed the source and content of imaginative and hallucinatory experiences in order to distinguish between those coming from divine influence and those of satanic inspiration.
In more recent historical accounts it has been documented, for example, that Sigmund Freud (18561939) had heard his name being called by “an unmistakable and beloved voice” while living in a foreign city [2].
Jaynes [3] offered an alternative to the medical view of hearing voices. In his work, he described an ancient mental structure called the “bicameral mind”.
He claimed that, until a few thousand years ago, humans had not developed a self-reflective consciousness and were guided by the voices they heard. The voices were attributed to the gods. He compared this mental structure to the experiences of hearing voices in people diagnosed with schizophrenia.
Therefore, the experience of hearing voices has been considered since ancient times as something characteristic of human nature. In some cases, pointing to it as a special quality, in other cases assigning it a deep religious meaning, in others as premonitory tool for decision making, and in others as something that could interfere in the daily life.
Although the experience of hearing voices has been widely described throughout history, in Western cultures it has generally been regarded as “the first sign of madness”.
CONCEPTUAL FRAMES AND EXPLANATORY MODELS
The conceptualization and approach to auditory hallucinations is closely related to the historical evolution of attention and treatment of severe mental disorder (SMD). In order to understand this evolution, a brief description of its historical course seems appropriate.
The treatments carried out in psychiatric institutions from the 14th century onwards (Bethlem Hospital) were characterized by their ineffectiveness and therapeutic aggressiveness. Patients were practically deprived of their “human condition and dignity”. Such a situation was maintained in the following centuries. At the beginning of the 20th century, new formulas were tried, but they maintained the same aggressive therapeutic styles of the past: frontal lobotomy or convulsive treatment with intravenous camphor. Even so, the twentieth century was a definitive turning point in the care of SMD. The change experienced in this attention in the middle of the last century took place at the expense of diverse factors:
Psychiatric deinstitutionalization in the mid-20th century: The return of patients to the community environment required a change in the model of care.
The new model of community attention: Which, even with its varying pace of implementation, it has managed to be incorporated as a model of care in the assistance policies of the different state mental health systems [4].
The new psychopharmacological era: Progress in this field contributed to patients being able to maintain longer periods of clinical stability, reduce the adverse effects of the old treatments and improve their general functionality. This led to new demands on the part of patients and their families for their social and occupational integration, which could not be met exclusively by pharmacological treatment.
The impact of the person-centered recovery approach: which globally reconfigures the attention to SMD and is incorporated as a key element in the new design of mental health care policies.
The rise and impulse of patient and family associative movements, which contributed decisively to this reformulation of SMD attention.
It is attributed to Jean-Etienne-Dominique Esquirol (1772-1840) the definition of hallucination as “a perception without object”. Vallejo Ruiloba [5] mentions that this definition was formulated by Benjamin Ball (1833-1893).
Jules Baillarger [6] presented an essay on the relationship between hypnagogic states and hallucinations before the Royal Academy of Medicine of Paris. He summarized that, “the most frequent and complicated hallucinations affect the ear; the number of voices varies, they reach it from all directions and can even be heard in only one ear” [7].
Karl Jaspers [8] in his classic work “General Psychopathology”, and specifically in the section dedicated to the manifestations of the sick psychic life, addresses the subject of hallucinations referring to them as, “deceptive corporeal perceptions which have not arisen from real perceptions by transformation, but which are completely new and which appear alongside real perceptions”.
Therefore, since the beginnings of psychiatric psychopathology, hallucination has been defined from a negative perspective, as Ey [9] quotes, “Indeed, hallucination is defined by the fundamental error that founds it. For to hallucinate is in principle and above all to transgress the law of perception. It is to perceive what does not entail perception at all”. In the work of Alvarez and Estevez [10] a detailed review of the historical conceptualization of hallucinations is made. In the same line, Geekie [11]. The author explores the explanatory models of hallucinatory experience and their historical conceptualization.
At the end of the 20th century, new explanatory models of hallucinatory experiences emerged. Thus, for example, in the work of Chadwick and Birchwood [12] a conceptual approximation is made from a cognitive approach. They point out that in the auditory hallucinatory experience, individual beliefs play a basic role. They indicate that these beliefs are vital for the maintenance of affective and behavioral responses. Reciprocally, behavior and affect strengthen or weaken these beliefs.
They also point out, citing Parkinson and Manstead [13], that it is probably futile to assert the primacy of either cognition or emotion, because the starting points in reciprocal dynamic sequences are arbitrarily defined and because both responses evolve together and are always significantly related.
From this same cognitive-behavioral approach, diverse contributions have been made focused on the conceptualization and approach to hallucinatory experiences. In this regard, it is worth noting the studies by Morrison [14-16] and the work of Waters [17] where it is presented an integrated model of the cognitive mechanisms involved in the auditory hallucinatory experience of schizophrenic and non-schizophrenic population.
In the work of Perona-Garcelán [18] an interesting conceptual approach is made. The author points out that, although there is some agreement on the links between internal mental events and auditory hallucinations, there are still some doubts about the mechanisms involved in the development and maintenance of erroneous attributions about these hallucinations.
The author discusses how the two current lines of research explain these mechanisms. For the first, this inadequate attribution is caused by a deficit in some aspect of the subject's cognitive functioning, citing: Hoffman [19]; Frith [20]; Hemsley [21]; David [22]. For the second, there is a bias in the monitoring of internal events, citing: Slade and Bentall [23]; Morrison [14].
Researchers who defend the hypothesis of a deficit in cognitive functioning claim that there is some failure in the neuropsychological processes of speech planning or internal event tracking.
Researchers defending the bias theory argue that the inability to discriminate real events is caused by top down processes, such as metacognitive beliefs and cognitive dissonance.
According to Perona-Garcelán [18], these theories can only explain why patients experiencing hallucinations attribute their own private events to public ones. However, they do not explain other relevant features of hallucinations, such as:
- Why can't the hallucinator recognize his private events?
- What determines the content or subject matter of the voices?
- Why do the voices speak in second or third person?
- Why do voices acquire particular characteristics such as gender, accent, tone of voice?
- How are beliefs about voices formed?
- How do such beliefs arise?
- How are they maintained and consolidated over time?
In the author's opinion, voice episodes are contextualized in the overall hallucinatory process. Consequently, personal antecedents (metacognitive beliefs, suggestibility and personality traits) influence the process and probably determine its activation and deactivation in the course of time. Once the process is fully formed and consolidated, the traumatic and stressful situations that triggered it are no longer necessary. After the first experiences of the voices, and especially when they have acquired pragmatic and dialogical properties, the subject becomes completely familiar with them and it becomes easier and easier for the voices to appear and reappear on many occasions without the occurrence of a very intense stressful event.
This means that the stressful event may be a sufficient condition for triggering the hallucinations, but it is not a necessary condition. It has also been pointed out that there is a substantial gap in these phenomenological and neuroscientific approaches when they attempt to explain the complexity of psychotic experiences.
In this regard, the work of Humpston [24]. The authors, and as a possible approach to address such a gap, point to computational psychiatry, an emerging field that uses formal mathematical models to attempt to delineate the mechanisms of brain function and pathological states.
Other studies have focused on cultural variability and observed differences in the experience of listening to voices. In this regard, Luhrmann [25]. The authors conduct an interesting work aimed at exploring and comparing the experience of listening to voices in different cultural settings. They investigated the differences between patients from California (USA), Chennai (South India) and Accra (West Africa). They observed the following differences:
- In the California sample, patients tended to describe their voices as intrusive and unrealistic thoughts.
- In India, they were inclined to view the voices as a possible helpful guide to daily life.
- In the African sample, patients considered the voices to be morally good and causally powerful.
For the authors, persons with psychosis pay selective attention to a constant stream of many different auditory and quasi-auditory events, due to diverse “cultural invitations” and variations in ways of thinking.
They point out that this process, which they call “social switching,” is consistent with processes described in cognitive psychology and psychiatric anthropology, but which have not yet been sufficiently described with respect to cultural variations in auditory hallucinations.
The relationship between the meaning that individuals attribute to their voices and the efforts they make to cope with them has also been the subject of attention in other works. In this regard, Knudson and Coyle [26]. On a case study, they perform an interpretative phenomenological analysis of hallucinatory experiences.
The authors highlight the importance of entering the world of meaning making and subjective understanding that patients develop in relation to their voices, particularly in terms of the explanations that they construct. They hypothesize that a focus on the development of the construction of such meaning could help satisfy the patient's need for more convincing explanations. This, in turn, could form a basis for developing appropriate responses to voices that are congruent with individual interpretations of them, thus addressing reservations about the defense of phenomenologically decontextualized “coping mechanisms” in response to life traumas that reduce their ability to interfere with functioning and cause distress. The authors support their hypothesis, on reported findings that, although instruction in behavioral strategies for coping with voices may have clinically significant effects, many patients do not continue to use these strategies after instruction, citing: Allen [27]; Erickson and Gustafson [28]; Nelson [29]. The reason for this is that patients' conceptualizations of their voices are often not consistent with their use of the behavioral coping strategies in which they were instructed [30].
For example, distraction techniques, although they may be effective in reducing the intensity of hallucinations, are unlikely to be used if someone believes that their voices will punish any inattention.
The authors conclude that if the relationship between the meaning individuals attribute to their voices and their coping efforts were more firmly established, its implications for the clinical practice of professionals working with people who hear voices would be very positive.
On the phenomenological characteristics of listening to voices, some studies have focused on the process of “inner speech”. In this regard, Vilhauer [31]. The study examines the phenomenological characteristics of inner speech during the silent reading process (IRV).
A general population survey was conducted to assess the frequency, location, number, identity, control, and auditory qualities of IRV. Of the 570 respondents, 80.7% reported that they sometimes or always heard an inner voice during silent reading, and the remaining 19.3% reported that they always understood the words being read without hearing an inner voice.
The results indicated that IRV are a routine experience for many people. Most respondents reported IRV with specific auditory qualities, such as gender, accent, pitch, loudness, and emotional tone. IRV were reported in participants' own voices as well as in the voices of others. Some respondents reported that they could not control any aspect of their IRV, while others could control one or several aspects. The authors conclude that there is considerable individual variability in inner speech during the silent reading process.
Other more recent studies have been aimed at exploring the difficulties of voice listeners in processing another persons' speech. In this regard, the contribution of Richards [32]. The authors present the main findings of empirical research on the processing of external speech in people who hear voices. They point out, that these processing difficulties are observed even in the absence of hearing voices.
They conclude that a better understanding of these processing deficits by health care professionals may help them to communicate more effectively with affected individuals.
Regarding the use of phenomenology for the approach to hallucinatory experience, some more conceptual contributions have focused on establishing the differences between the phenomenological and the cognitive approach. In this regard, Larøi [33].
The study notes that, the empirical-rationalist approach adopted by the cognitive sciences considers a hallucination to be both a perception and a voice, however, the phenomenological approach emphasizes the primordial transformation of self-awareness and personal experience.
Some work has explored how anxiety can induce hallucinations. In this regard, Ratcliffe and Wilkinson [34]. They point out that, anxious anticipation of one's own thought content is what generates the hallucination.
According to the authors, this is related to what Stephens and Graham [35] called the “alien quality” of auditory hallucinations defined as something that neither always originates in the external environment nor always has sensory properties similar to veridical perceptions.
Anxiety induces auditory hallucinations in the following way: anxious anticipation of thought contents as they become increasingly determined results in a quasiperceptual experience of the thought content. When the person is confronted with something he or she seeks to avoid and feels unable to resist, the resulting experience is more like an affectively charged perception than a common thought episode. In the authors' view, this fits with subjective reports that anxiety triggers or aggravates the hallucinatory experience, that the voices confirm negative self-evaluations, and that the voices are somewhere in between the experiences of hearing and thinking.
There has also been research on the relationship between attachment anxiety and the distress generated by hearing voices. In this regard, Berry [36]. The authors found modest but significant positive associations between attachment anxiety and severity and distress in relation to hearing voices, but found no associations between attachment avoidance and these dimensions. The associations between anxious attachment and distress elicited by voices are consistent with previous research showing relationships between attachment anxiety and subclinical hallucinations.
Despite some limitations noted by the authors, the study findings are consistent with the emerging literature on associations between individuals' psychological characteristics and the experience of hearing voices.
In the qualitative study conducted by Fenekou and Georgaca [37], the importance of conducting a detailed evaluation of the hallucinatory experience is addressed. As a starting point, the authors point out that asking psychiatric patients for a detailed description of their voices does not seem to be part of routine clinical practice, mainly due to the reduction of voice hearing by conventional psychiatry to a meaningless psychiatric symptom. The study highlights that hearing voices is a complex experience that voice listeners cope with in a variety of ways, developing sophisticated frameworks to make sense of that experience. For the authors, there is an established relationship between the listener and their voices, which is characterized by stability and consistency. The crucial parameters of this experience appear to be the time spent listening to voices, which is related to; the stabilization of the voices, the listener's acceptance of the voices, the reality testing strategies used, and the extent to which the voices are perceived as positive or negative.
On this same aspect of the stability and consistency of voices and their permanence over time, the work of Hartigan [38].
The first aim of this study was to attempt to replicate a previous finding that beliefs about voices were enduring and stable, regardless of changes in voice severity, and that they did not change without specific intervention.
The second aim was to examine whether listeners' interrelationships with their voices changed over time, without specific intervention.
The results were that beliefs about the omnipotence and malevolence of voices remained stable over a 12-month period, as did voice-listener interpersonal styles, despite a trend toward reduced voice-related distress and disruption. However, there was a tendency for beliefs about the benevolence of voices to decline over time.
The authors conclude, that styles of voice-listener interrelationships appear relatively stable and enduring, as do beliefs about the malevolent intent and power of voices.
THE HEARING VOICES MOVEMENT (HVM)
In the set of worldwide initiatives related to current approaches to recovery and empowerment of users, it has been precisely the organized collectives of these users who have set the course with their valuable contributions and perspectives.
Some of these contributions have the added value of having been recounted in first person, but other collective contributions have managed to be linked to proposals that have become part of state and international policies, and have been embodied in different projects, agreements and strategies of broad consensus. These movements and user groups have opened their own space in this global context of empowerment.
Among them, it is worth mentioning the Voice Hearers Groups (VHG) that, after their first experiences in Northern Europe and the creation of their first organizations: “Foundation Resonance” in Holland (1987) and “Hearing Voices Network” in the United Kingdom (1988), have managed to disseminate their work worldwide.
Since then, networks have been established in more than 30 countries. In 1997, the “Intervoice Network”, an international organization that provides coordination and support to the Hearing Voices Movement, was formed.
In our area (Spain), the movement of voice hearers has also been spreading. To highlight the movement “Entrevoces”, organizer of the 7th World Congress of Hearing Voices, held in Alcalá de Henares (2015).
Notable influence has also been exerted by the Mutual Help Groups and Peer Support Groups of users organized at different levels, both in supranational organizations and at the state and local levels.
ORIGIN OF THE HEARING VOICES MOVEMENT
It is obligatory at this point to recall the experience of Patsy Hage (1955-2015). Patsy Hage began hearing voices at the age of eight. Initially she thought the voices were her “protectors”, and intense personal or family situations the voices helped her.
She heard about 20 voices and liked to talk to them. But as he grew older, the voices became his “enemies”. At the age of 16 she ran away from home, but the voices followed her. Later, she dropped out of university, struggled to keep her job, was diagnosed with schizophrenia and spent adulthood in and out of hospitals. At the age of 60, she requested assisted suicide under the euthanasia legislation allowed in the Netherlands.
Patsy Hage was critical of her psychiatrist Marius Romme's clinical approach to the hallucinatory experience. She pointed out to him that instead of using the voices only to make a diagnosis, he should help her cope with the experience.
Together they read and discussed the aforementioned work by Julian Jaynes [3]: The Origins of Consciousness in the Breakdown of the Bicameral Mind.
Jaynes argued that in ancient times humans lacked consciousness as we know it today and instead experienced thought as a series of auditory hallucinations and commands that they attributed to their leaders or gods. These voices, Jaynes speculated, may have been similar to those heard by people with schizophrenia. Patsy Hage contributed a chapter to Romme and Escher's, “Accepting Voices” [39], in which she described Jaynes's theory of the bicameral mind.
Romme related that Hage had found it very “reassuring” to consider that three or four thousand years earlier, his experiences might have been normal. The experience of Patsy Hage and the pioneering work of Romme and Escher [39,40] were of great importance in the origin and subsequent impetus of the Hearing Voices movement.
CURRENT POSITIONING OF THE HVM A PARADIGM CHANGE
In order to understand the current position of the HVM and the paradigm shift that it has brought about in the care of SMD, it is useful to briefly describe some of the studies and theoretical contributions that served as a framework.
Romme and Escher [39,40] pointed out that the voices had meaning and made sense if they were analyzed jointly with the traumatic life events that motivated their appearance.
They supported their assertion, after conducting multiple interviews with people who heard voices and found that up to 75% of them had suffered some traumatic experience related to those voices.
The authors report these experiences in the third of a series of texts dealing with such experiences [41].
The three books refer to the list of Maastricht Interviews. Romme and Escher distinguished three phases in the process of hearing voices: (1) Startle: Occurs with the first appearances of voices. It is the stage where persons may be overcome by fear and anxiety when they hear their first voices; (2) Stabilization: It occurs when people accept hearing voices as part of their lives; (3) Organization: When persons accept that they hear voices, have taken responsibility for them, have learned to live more comfortably with them and can live without them dominating them.
For the authors, the expectation of recovery should not relate to the extinction of the voices, but to how the person relates to those voices. The philosophy is that, "recovery is only possible when the voices are accepted". In the same vein, Baker [42]. Exploring in detail the subjective experience of psychosis and the traumatic life events suffered by the affected person from an early age is therefore a key task. Some works have been directed to this end. Of note are: Escher [43]; Read [44]; Geekie and Read [45]; Parry [46].
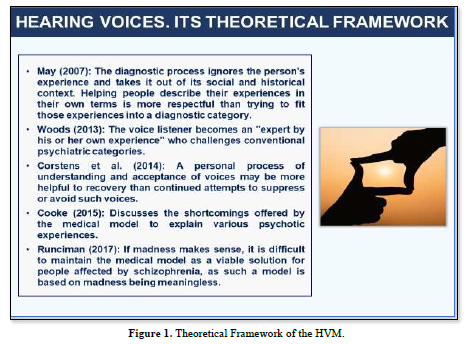
For Woods [47], the listener of voices becomes an "expert by his or her own experience" who defies conventional psychiatric categories. Voices can be understood as a natural part of the human experience. There may be various explanations for the origins of voices. In this way, voices can be interpreted and understood in the context of life events and interpersonal narratives. A personal process of understanding and acceptance of voices can be more helpful to recovery than continued attempts at suppression or avoidance. Peer support and collaboration can be very empowering and beneficial in the recovery of affected individuals. In this regard, Corstens [48].
From some more critical contributions, although without providing clear evidence, it has been questioned whether the Voice Listeners Movement has meant a real change and new paradigm in the approach to the hallucinatory experience. In this regard, Evrard and Le Malefan [49]. For these authors, the approach advocated by Romme and Escher [43] is a “return to neurosis” that is not fully recognized, because it conceals part of the knowledge about the compatibility of neurosis and verbal hallucinations.
Linking the voices to the traumas and working through the emotions associated with those experiences would return the person to the right direction, as long as the change itself does not seem too threatening. However, the authors question whether this reversal of clinical bias actually leads to a valid clinical differential.
They conclude, that the Voice Hearers Movement has offered a competitive clinical practice, but that it has failed to provide a true clinical differential practice.
Other contributions have focused on the secondary effects of the diagnostic process, and how this process converts the distress experienced by an individual affected by a psychosocial problem into a personal problem.
In this regard, it is worth noting the work of May [50]. For the author, and despite the recognized problems with the validity and reliability of diagnostic categories, the diagnostic process does not consider the experience of the person and removes him from his social and historical context. The author points out that a much-neglected issue is how mental health service users experience the news of the diagnosis.
Thus, for example, when a person is diagnosed with schizophrenia, they and the people around them may acquire and develop a “learned hopelessness”. He concludes that helping people describe their experiences in their own terms is more respectful than trying to fit those experiences into a diagnostic category.
In the extensive and valuable work by Cooke [51], all these aspects are explored in depth and the deficiencies offered by the medical model to explain the different psychotic experiences are analyzed. This is noted, in the continuous expansion of diagnostic categories and systems. However, psychotic experiences are situated on a “continuum” and do not fit into precise categories. In the contribution of Runciman [52], it is pointed out that, if madness becomes meaningful, it is difficult to maintain the medical model as a viable solution for people affected by schizophrenia, as such a model is based on madness being meaningless. She concludes that, by listening to the stories of affected people, helping them to contextualize their symptoms and find meaning in their experiences, it is possible to profoundly change not only the patient's life, but also the professional's own role.
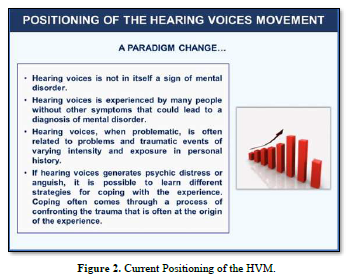
These frames and new perspectives for the explanation of psychotic experiences have marked the path and current positioning of the voice hearers' movement, which can be summarized as follows:
- Hearing voices is not in itself a sign of mental disorder.
- Hearing voices is experienced by many people without other symptoms that would lead to a diagnosis of mental disorder.
- The hearing of voices, when problematic, is often related to problems and traumatic experiences of varying intensity and exposure in personal history.
- If hearing voices generates psychic suffering or distress, it is possible to learn different strategies to cope with the experience. This coping often comes through a process of confrontation of the traumatic experience that is often at the origin of the voices.
For some authors, this experience of hearing voices has suffered a certain subversion, having been replaced by what we currently call knowledge or consciousness. In this regard, the work cited by Jaynes [3].
It could also have contributed to this subversion, the conceptualization of psychosis made by classical psychiatry and by the prevailing biologists’ model until psychiatric deinstitutionalization, and by the reductionist eagerness of diagnostic systems.
As noted, the pioneering works of Romme and Escher [39-41] contributed to the initial theoretical framing of HVM.
More recent contributions of the literature have continued to contribute elements to this initial theoretical framing, and to the current positioning of the voice hearers' movement.
A summary of this is provided in Figures 1 & 2 below:
To some extent, the HVM comes to rescue and recontextualize the old consideration about listening to voices.
Therefore, the paradigm shift does not seem to be related to listening to voices per se, but to their attention by the care services.
VOICE HEARERS GROUPS
The following will be broken down in this section:
- Main characteristics of VHGs.
- Experiences realized with VHGs.
CHARACTERISTICS OF THE VHG
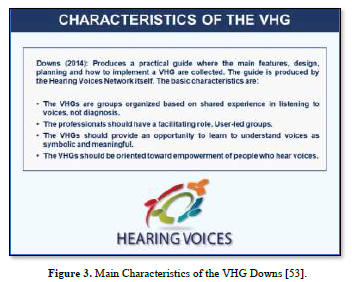
On the nature, main characteristics, design and form of implementation of a group of voice listeners, it is worth noting the practical guidance produced by Downs [53].
This guide was promoted and developed by the Hearing Voices Network. In Figure 3, it summarizes the main characteristics indicated in this guide.
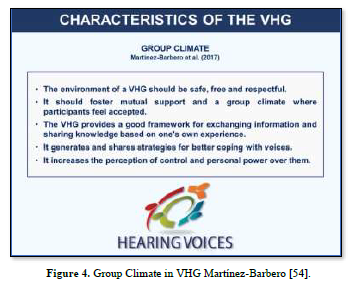
It has been pointed out, the special importance of the "climate" that should surround a VHG. Martínez-Barbero [54] indicate that the environment should be safe, free and respectful, in a group space that fosters mutual support and where participants feel accepted. The authors point out that these groups provide a suitable framework for exchanging information and sharing knowledge based on one's own experience, generating and sharing strategies for better coping with voices.
This, in turn, increases the perception of control and personal power over voices. The first-person testimonies and the subjective experience of the affected persons are fundamental to achieve a better understanding of psychic suffering and of those aspects that help to alleviate it. It is summarizing below, the main elements of the group climate that should surround a VHG, as pointed out by Martínez-Barbero [54] (Figure 4).
The orientation and framing of the role of professionals in VHGs are determined by the very nature of this type of groups.
In the valuable work of Downs [53], a practical framing of the criteria that should guide the role of a VHG professional facilitator is offered.
The author warns that facilitators must be very careful not to impose their beliefs. Each listener may have a different explanation for listening to their voices. She highlights honesty as the main element and quality of a facilitator, and says: “There is no substitute for honest feedback. The facilitator should not become obsessed with getting the group right and end up with cold or rigid responses”.
Functions
As central elements to be considered in the role of professionals, the following should be pointed out:
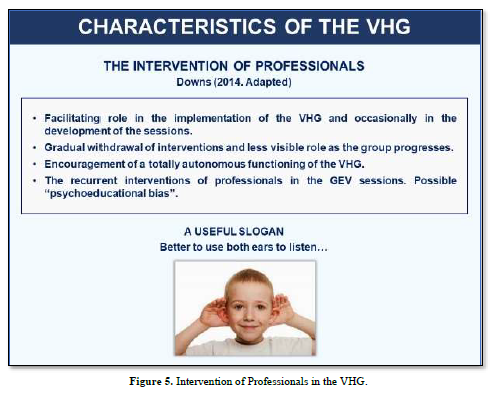
Their role as facilitator in the implementation of the VHG and occasionally in the development of the sessions.
Gradual withdrawal of interventions and less visible role as the group progresses.
Try to take care of the possible “psychoeducational emphasis” in interventions. To this end, a useful slogan is, “better to use both ears to listen”.
Encourage the totally autonomous functioning of the group.
All in all, the role of the facilitator, in the words of Downs [53] “is complex and very demanding”. The professional must have certain skills and at the same time provide good support. It is common that some of the contents dealt with in a VHG, following the experiences, stories or requests of the users, come up against the professional's own knowledge, beliefs or personal attitudes. Thus, for example, when a user comments that the voices are very intense and annoying lately, and that he believes it is related to a specific consumption of cannabis with his friends. The professional facilitator may consider that his role is to remember at that moment the negative impact of the consumption of toxic substances, the influence of stress in the clinical evolution or even resort to explanatory models of vulnerability-stress. Such seemingly useful strategies may not bring real benefits to the user's current need and suffering.
Therefore, it is not advisable for professionals to strive to explain everything. Hence, the importance of avoiding “psychoeducational emphasis”. It is likely that the user's only intention is to be listened to and not to have everything explained to it.
NUMBER OF PROFESSIONALS
In the VHGs implemented in the health care setting where the authors of this work carry out their professional activity, the following criteria have been considered:
As a rule, 2 professionals: 1 main facilitator and 1 support facilitator. This favors the distribution of tasks, the proper planning of the sessions and, in addition, can provide the main facilitator with “moments of respite” in their work.
The professionals in training will not participate in the VHG unless the group of users has been previously informed and has authorized their participation. It will be necessary for these professionals to have a specific function previously agreed with the group. The participation of professionals who are exclusively "listeners" in a group of these characteristics is discouraged.
By way of summary, the main elements to be considered in the intervention of professionals are presented below, following the proposal made by Downs [53], which is adopted partially adapted (Figure 5).
For the implementation of a GEV, the following basic criteria are considered:
- Agreement of confidentiality of users and professionals, on what was discussed in the sessions.
- Autonomous functioning of users.
- Professionals play a merely facilitating role.
Other elements to consider are:
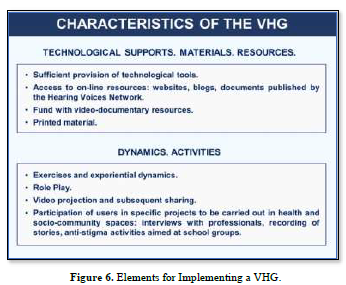
- Means and equipment.
- The structure of the sessions.
- The “setting” prior to the session.
- The frequency of the sessions.
- The support material and technological supports.
- The dynamics used.
- The recording of the sessions: agreements, user requests, etc.
By way of summary, the basic elements to be considered in the implementation of a VHG are presented below (Figure 6).
In VHG sessions, it will often be necessary to support users in improving their skills and strategies for coping with their voices. The professionals, along the lines pointed out by Downs [53], will have to be very careful with their interventions.
It is very convenient to rely on the resources and materials developed by the network of voice hearers themselves. They are the real experts.
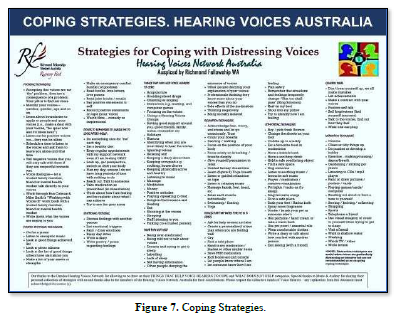
The Intervoice Network currently brings together more than 30 statewide voice hearers' organizations. The production of material produced by the HVM at the global level is extensive and can be very useful for the development of the facilitating role of professionals. Some national networks have produced very practical documents with recommendations and strategies for coping with voices. In Figure 7 is shown a document produced by the Hearing Voices Network of Australia.
Likewise, facilitating professionals should pay special attention to very young users participating in a VHG. It has been pointed out that if early psychosis is not successfully treated, this can have a very detrimental impact on the long-term prospects of the young people affected. As exemplified by repeated hospitalizations, high unemployment rates, poor quality of life, and high suicide rates [55].
The life impact produced by an early psychotic debut can be very important. It affects the young person, cutting off many of their expectations (academic, social, sentimental). It usually causes hopelessness, frustration, self-stigma. And all this in an evolutionary period that has not concluded. In fact, pharmacological treatment with young psychotics is complex and must observe everything concerning the maturation and brain plasticity of the young person. To the initial bewilderment after the news of the diagnosis is added the difficulty for family members to understand and cope with the patient's symptoms and behaviors. Many young people, and also their families, have expectations and interests that may seem inappropriate or not adjusted to their clinical situation.
The professionals must be very cautious with this subject. It should not be forgotten that young patients, precisely because they are young, have a long life ahead of them, and what in professional criteria may seem inappropriate or unfeasible at present, may be possible in time.
For all these reasons, close collaboration and information exchange between users, families and professionals is fundamental.
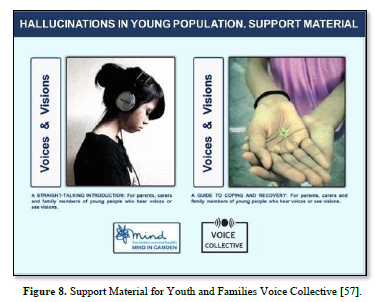
In some settings, it has been given special attention to this aspect, complementing the interventions with psychoeducational material to support users and their families. Voice Collective is a UK national project to support young people with psychotic disorders and their families.
In 2021, Voice Collective developed specific material aimed at users and caregivers of young people with visual or auditory hallucinations, which may be useful to improve knowledge of the disease and their coping with it. In VHGs, this material can also be useful [56] (Figure 8).
EXPERIENCES REALIZED WITH VHG
It should be noted that the VHGs are not characterized by a predefined structure and timing. They are not groups with a beginning and an end, since it is the users who set the course.
Their implementation has a start date, but not a closure date. However, some recent experiences with VHG have been carried out in a more structured way.
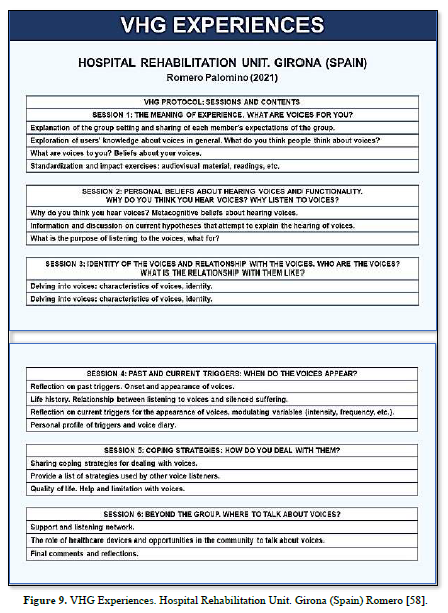
In the work of Romero [58] a VHG is implemented in the Subacute Unit of the Hospital Rehabilitation Unit of Girona (Spain). This experience could be useful in other healthcare contexts with the necessary adaptations.
One of the interesting aspects of this experience is the protocol offered for the sessions and contents to be treated in a VHG.
The author has developed a protocol for VHG, with various contents distributed in 6 sequential sessions (Figure 9).
In other recent experiences, the distinctive element is not the structure of the VHG, but the "informal space" in which it takes place.
The "Hearing Voices Coffee” experience is a good example of this. This “voices coffee” could be the name of any trendy coffee shop. But also, the phenomenon of hearing inner voices is called “voices”.
Playing with this ambiguity, Dora García has launched a meeting place for people who hear voices. Her experience is described in the journalistic report made by Camarzana [59].
This is a project that revolves mainly around exchange, research and destigmatization.
Functions as an inclusive space where voice hearers and their friends, people interested in the phenomenon, and accidental clients meet (Figure 10).
RESEARCH AND STUDIES ON VHG
In recent decades, there has been a growing focus of interest in the scientific literature on the impact and effectiveness of VHG and their implications for clinical practice. The following are some of the contributions. The study by Oakland and Berry [60] explored the individual experiences of users participating in VHG. Semi-structured interviews were conducted. Interviews were transcribed and analyzed using thematic analysis.
Five themes emerged:
- Discovery, related to initial group attendance.
- Group structure, consisting of the key ingredients of the group.
- Acceptance, reflecting an acceptance of their experiences.
- Hope, exploring hope in the group.
- Benefits of the group.
The study extends previous research on the role of peer facilitation in hearing voices and supports existing research on the importance of hope, acceptance, and coping with such experience. Along similar lines, Rácz [61].
The authors made an interpretative phenomenological analysis of the individual hallucinatory experiences of users participating in self-help groups and the role of such groups in improving outcomes. As a starting point, they point out the change of perspective that has occurred in the approach to the hallucinatory experience due to:
- Epidemiological data indicating incidence of the experience in the general population.
- Influence of new cognitive-social therapeutic models in the approach to the hallucinatory experience.
- Influence of the user-centered recovery model and the crucial role it has played in the integration of personal hallucinatory experiences and their understanding.
As results of their analysis, the authors identify four main categories:
- The role of the voice.
- The relationship between the voice and the "I", with these two subcategories: symmetrical relationships, asymmetrical relationships, and voice position.
- The role of the self-help group.
- The role of the coping method in listening to voices.
Regarding the coping method in listening to voices, the authors emphasize its connection with the change in the patients' relationship with their voices and with the change in their social relationships. In Figure 11, these connections and changes are shown.
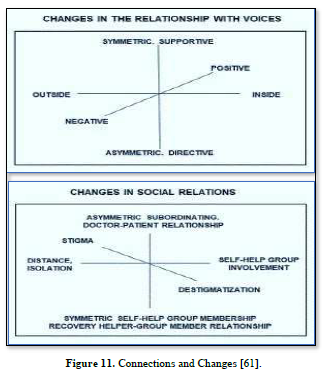
The authors conclude that:
- The self-help group provides significant help in the identification and treatment of voices. Thus, it serves as a turning point in the life history of voice hearers.
- The application of the self-help group in the clinical setting contributes to improved treatment outcomes for affected individuals.
Some contributions have focused on the positive aspects of listening to voices. Of note is the work of Jackson [62].
The study revealed three explanatory factors for the positive relationship between the affected person and the voices: the reduction of fear, the recognition of positive feelings, and the establishment of control.
These factors were based on different processes: personalization of the voices, personal connection to the voices, sense of independence, connection to community, and a personal and meaningful narrative about hearing the voice in the life story.
Along similar lines, the recent contribution by Valavanis [63]. This review explored and synthesized the qualitative literature related to the positive aspects of listening to voices, identifying several thematic areas in which voices made a beneficial contribution to listeners' lives. In conclusion, the authors suggest that practitioners carefully consider these positive aspects in their clinical practice and try to open exploratory and collaborative dialogues to facilitate understanding of listeners' beliefs in a way that is most helpful to them.
Other studies, have addressed the inquiry into individual narratives and experiences in coping with distressing voices, and the different typologies of recovery (de Jager et al. 2016) [64]. In the study, the recovery experiences of 11 distressed voice listeners are explored over time. The authors observed two typologies of recovery:
Turning toward/empowerment: which involved the development of a standardized description of voices, the building of specific skills, the integration of voices into daily life, and a transformation of identity.
Moving away / protective hibernation: Which involved drawing on all available resources to survive the experience, highlighting the importance of medication in recovery. Participants who "walked away" had also recovered in terms of symptoms, quality of life, and psychological distress.
The authors point out that the recovery style of individuals may vary over time. Therefore, care services must be sensitive and responsive to the individual's recovery style and readiness to change at any given time.
From the research field, some contributions have been made to explore the effectiveness of group interventions on psychotic symptomatology and hallucinatory experiences. The study by Wykes [65] is worth noting in this regard. The authors present a group treatment format for auditory hallucinations based on cognitive-behavioral therapy (CBT), and offer results of its implementation. As a preliminary hypothesis, they propose that the group format could add value to the intervention, given the potential of group processes and synergies.
They select three main outcome measures assessed using the instruments: PSYRATS. Haddock [66]; BPRS. Ventura [67]; IS. Insight Scale. Birchwood [68]. They also assess levels of depression, anxiety and self-esteem: BDI Inventory. Beck [69]; BAI Inventory. Beck [70]; Self-Esteem Scale. Rosenberg [71].
Wykes [65] document significant changes in the three main outcome measures after treatment. These changes were maintained at follow-up. Specifically, there were changes in perceived power and distress, as well as a significant increase in the number and effectiveness of coping strategies.
They note that group psychological treatment for distressing auditory hallucinations can reduce symptoms and increase understanding of such hallucinations. Patients experiencing distressing voices expressed high levels of satisfaction with treatment. The treatment effect was similar to that obtained in individual therapy, but temporarily less costly. They indicate that the group format is possibly less effective in the long term than individual CBT.
Alternatively, group treatment could be considered as a supplement to individual CBT, inducing users into individual work, reducing the duration of treatments or even increasing the efficacy of individual CBT. They conclude that group treatment for hallucinations may improve the prognosis of many people with treatment resistant psychotic symptoms. In the same vein, Goodliffe [72]. The authors point out that the use of cognitive group therapy for the management of distressing voices offers a promising outlook.
On the use of the group format for addressing auditory hallucinations and its potential benefits in coping strategies, it is also worth noting: Perron and Munson [73]; May [50].
In recent decades, there has been a growing focus of interest on the use of new technologies and digital tools for coping with the hallucinatory experience of affected individuals. In this regard, Barros and Domont [74]. The study explored the various ways in which voice hearers can create strategies to share their experiences in a virtual environment. The authors note the frequent migration of users, which often occurs from the Inter voice Network to virtual settings.
The Netnography, as an online research method inspired by ethnography to understand social interaction in current digital communication contexts, proved to be an appropriate tool to explore exchanges of experiences between voice listeners and explore their coping strategies. The authors point out that the use of virtual environments also allows voice listeners to create social bonds and contributes to the development of a new vision of their "way of existing in the world". In the same vein, the recent contribution of Thomas [75]. The authors conclude that the use of digital technologies presents a promising outlook and significant potential.
In the study by Longden [76] a systematic assessment of the impact and effectiveness of self-help groups in the Hearing Voices Network (HVN) is conducted. The authors developed a survey that they applied to 62 groups affiliated to the network. They select different categories of analysis and offer the comparative results of the statistical analysis carried out. Among them:
Differences in the level of overall satisfaction:
Gender differences: There were no significant differences in total scores.
Group differences with respect to facilitator conduction: There were no significant differences in satisfaction between groups that had only voice listeners as facilitators, only mental health professionals as facilitators, or voice hearers and professional facilitators.
Differences regarding length of time attending groups: There were no significant differences in satisfaction between respondents who had been attending the group for one-six months, six months-one year, one two years, or more than two years.
Correlations between in-group experiences and social/occupational outcomes:
There were significant positive correlations between in-group experiences and positive out-group social/occupational outcomes. The strongest specific associations were between: (1) Perception of the group as a safe place to talk about difficult things and cope with voices, with safety in asking for help (p =.0001); (2) Perceived usefulness of the group in making sense of and coping with voices, with increased safety in social situations (p =.0001).
Correlations between group experiences and clinical variables: There were no significant positive associations between group experiences and clinical variables.
For the authors, this qualitative research on HVN groups suggests that acceptance of the experience of hearing voices can facilitate social acceptance and self-acceptance, along the lines described by: Hendry [2]; Oakland and Berry [60]; Romme [41].
They note finally, that the study data do not allow firm conclusions to be made about the exact nature of the associations found between group attendance and improved quality of life, but serve to highlight the importance of holistic approaches to recovery, which recognize and utilize domains beyond the purely clinical and symptomatic [77-83].
RESULTS
The main results are as follows:
The experience of "hearing voices" has not been a static issue throughout history and has been conceptualized in a variety of ways.
Hearers attribute different meanings to their voices, and a great deal of cross-cultural variability has been documented with respect to the meanings attributed.
Attention to the hallucinatory experience must take careful consideration of each individual's personal experiences, previous traumatic events, and social and historical context.
The styles of interrelationship between voice and listener appear relatively stable and enduring over time, as do beliefs about the intent and malevolent power of voices.
The HVG can provide significant assistance in identifying and coping with voices and can serve as a turning point in the life history of voice hearers.
The care services should be sensitive and responsive to the individual's recovery style and readiness for change at any given time.
The use of strategies outlined by current more holistic models (Contextual Therapies, ACT, CBT) can be integrated into clinical practice for the care (individual or group) of persons hearers and coping with their voices.
The use of digital tools and virtual environments is emerging as a promising strategy for group intervention with voice hearers.
CONCLUSION
The main conclusions are as follows:
The experience of hearing voices should not be considered as an isolated and meaningless psychiatric symptom.
The usual attention to the hallucinatory experience in care settings and organizational paradigms must be reoriented.
The contributions made by the Hearing Voices Movement have contributed to recontextualize the conceptualization and approach to the hallucinatory experience.
The Voice Hearers Groups can offer an alternative to current models of recovery and empowerment of users.- Luque R (2007) Alucinaciones: Revisión histórica y clínica. Informaciones Psiquiátricas. pp: 189.
- Hendry GL (2011) What are the experiences of those attending a self-help hearing voices group: an interpretative phenomenological approach. [TD. Clin. Psychol.]. The University of Leeds. Academic Unit of Psychiatry and Behavioral Sciences. School of Medicine.
- Jaynes J (1976) The Origin of Consciousness in the Breakdown of the Bicameral Mind. Houghton Mifflin, Mariner Books.
- Gutiérrez-Colosía MR, Salvador-Carulla L, Salinas-Pérez JA, García-Alonso CR, Cid J, et al. (2017) Standard comparison of local mental health care systems in eight European countries. Epidemiol Psychiatr Sci 28(2):210-223.
- Ruiloba VJ (2011) Introducción a la psicopatología y la psiquiatría. 7ª edición. Elsevier Masson. Barcelona. ISBN: 978-84-458-2034-6.
- Baillarger J (1842) Des alucinaciones, des causes qui les produisent et des maladies caractérisent, Mémoires de l' Académie de Médecine. Paris.
- Berrios G (2014) Historia de los síntomas de los trastornos mentales. Editorial Fondo de Cultura Económica. ISBN: 978-968-16-8299-6.
- Jaspers K (1993, publicación original 1913) Psicopatología General. Editorial Fondo de Cultura Económica. ISBN: 978-968-16-3765-8.
- Ey H (1973) Traité des hallucinations, París, Masson 1: 47.
- Álvarez JM, Estevez F (2001) Las Alucinaciones: Historia y Clínica. Frenia. Revista de Historia de la Psiquiatría Vol. 1: 1
- Geekie J (2006) Escuchar las voces que oímos. La comprensión de los clientes de las experiencias psicóticas.
- Chadwick P, Birchwood M (1994) The omnipotence of voices: A cognitive approach to auditory hallucinations. Br J Psychiatr 164: 190-201.
- Parkinson B, Manstead AS (1992) Appraisal as a cause of emotion. In: Emotion (Ed. M. Clarke). London: Sage.
- Morrison AP, Haddock G, Tarrier N (1995) Intrusive thoughts and auditory hallucinations: A cognitive approach. Behav Cogn Psychother 23: 265-280.
- Morrison AP, Baker CA (2000) Intrusive thoughts and auditory hallucinations: A comparative study of intrusions in psychosis. Behav Res Ther 38(11): 1097-1106.
- Morrison AP, Nothard S, Bowe SE, Wells A (2004) Interpretations of voices in patients with hallucinations and non-patient controls: A comparison and predictors of distress in patients. Behav Res Ther 42: 1315-1323.
- Waters F, Allen P, Aleman A, Fernyhough C, Woodward TS, et al. (2012) Auditory hallucinations in schizophrenia and nonschizophrenia populations: A review and integrated model of cognitive mechanisms. Schizophrenia Bull 38(4): 683-693.
- Perona-Garcelán S (2004) A Psychological Model for Verbal Auditory Hallucinations. Int J Psychol Psychol Ther 4 (1): 129-153.
- Hoffman RE (1986) Verbal hallucinations and language production processes in schizophrenia. Behav Brain Sci 9: 503-548.
- Frith CD (1992) The cognitive neuropsychology of schizophrenia. Hove: Erlbaum.
- Hemsley DR (1993) A simple (o simplistic?) cognitive model for schizophrenia. Behav Res Ther 31: 633-645.
- David AS (1994) The neuropsychological origin of auditory hallucinations. In: A.S. David & J.C. Cutting (Eds.), The neuropsychology of schizophrenia. Hove: Erlbaum.
- Slade PD, Bentall RP (1988) Sensory deception: A scientific analysis of hallucination. London: Croom Helm.
- Humpston CS, Adams RA, Benrimoh D, Broome MR, Corlett PR, et al. (2019) From Computation to the First-Person: Auditory-Verbal Hallucinations and Delusions of Thought Interference in Schizophrenia-Spectrum Psychoses. Schizophrenia Bull 45: 56-66.
- Luhrmann TM, Padmavati R, Tharoor H, Osei A (2015) Hearing Voices in Different Cultures: A Social Kindling Hypothesis. Topics Cogn Sci 7(4): 646-663.
- Knudson B, Coyle A (2002) The experience of hearing voices: An interpretative phenomenological analysis. Existential Anal 13(1): 117-134.
- Allen HA, Halperin J, Friend R (1985) Removal and diversion tactics and the control of auditory hallucinations. Behav Res Ther 23(5): 601-605.
- Erickson GD, Gustafson GJ (1968) Controlling auditory hallucinations.
- Nelson HE, Thrasher S, Barnes TR (1991) Practical ways of alleviating auditory hallucinations. BMJ (Clinical research ed.) 302(6772): 327.
- Fowler D, Garety P, Kuipers E (1995) Cognitive Behavior Therapy for Psychosis: Theory and Practice. Chichester: Wiley.
- Vilhauer RP (2017) Characteristics of inner reading voices. Scand J Psychol 58(4): 269-274.
- Richards SE, Carruthers SP, Castle DJ, Rossell SL (2021) Speech processing in voice-hearers: Bridging the gap between empirical research and clinical implications. Aust N Z J Psychiatry 57(3): 322-327.
- Larøi F, de Haan, S, Jones S, Raballo A (2010) Auditory verbal hallucinations: Dialoguing between the cognitive sciences and phenomenology. Phenomenol Cogn Sci 9(2): 225-240.
- Ratcliffe M, Wilkinson S (2016) How anxiety induces verbal hallucinations. Conscious Cogn 39: 48-58.
- Stephens GL, Graham G (2000) When self-consciousness breaks: Alien voices and inserted thoughts. The MIT Press.
- Berry K, Wearden A, Barrowclough C, Oakland L, Bradley J (2012) An investigation of adult attachment and the nature of relationships with voices. Br J Clin Psychol 51(3): 280-291.
- Fenekou V, Georgaca E (2010) Exploring the experience of hearing voices: A qualitative study. Psych Psychol Soc Integrat Appr 2(2): 134-143.
- Hartigan N, McCarthy-Jones S, Hayward M (2014) Hear today, not gone tomorrow? An exploratory longitudinal study of auditory verbal hallucinations (hearing voices). Behav Cogn Psychother 42(1): 117-123.
- Romme MA, Escher S (1993) Accepting Voices. London, UK: Mind.
- Romme MA, Escher AD (1989) Hearing voices. Schizophrenia Bull 15(2): 209-216.
- Romme MA, Escher S, Dillon J, Corstens D, Morris M (2009) Living with voices: 50 stories of recovery. PCCS Books.
- Baker P (1995) The Voice Inside. Chester: Handsell Publications. Available online at: http://sindominio.net/versus/paginas/activida des/Textos_jor/text/Baker.htm
- Escher S, Romme M, Buiks A, Delespaul P, Van Os J (2002) Independent course of childhood auditory hallucinations: A sequential 3-year follow up study. Br J Psychiatry 181(43): s10-s18.
- Read J, Goodman L, Morrison AP, Ross CA, Aderhold V (2006) Trauma infantil, pérdida y estrés. In: Read J, Mosher L, Bentall R (eds.). Modelos de locura. Aproximaciones psicológicas, sociales y biológicas a la esquizofrenia. Barcelona: Herder pp: 271-306.
- Geekie J, Read J (2012) El sentido de la locura. Barcelona: Herder.
- Parry S, Loren E, Varese F (2021) Young people's narratives of hearing voices: Systemic influences and conceptual challenges. Clin Psychol Psychother 28(3): 715-726.
- Woods A (2013) The voice-hearer. J Mental Health 22(3): 263-270.
- Corstens D, Longden E, McCarthy-Jones S, Waddingham R, Thomas N (2014) Emerging Perspectives from the Hearing Voices Movement: Implications for Research and Practice. Schizophrenia Bull 40: S285-S294.
- Evrard R, Le Malefan P (2013) Que changent les “entendeurs de voix” à l'écoute des hallucinations? II.
- May R (2007) Working outside the diagnostic frame. Psychologist 20(5): 300-301.
- Cooke A (2015) Comprender la Psicosis y la Esquizofrenia. (Ed: Anne Cooke). División of Clinical Psychology (The British Psychological Society). Available online at: http://www.infocop.es/pdf/comprenderpsicosis.pdf
- Runciman O (2016) Escuchadores de voces: Un cambio de paradigma para la esquizofrenia. Revista de enfermería y salud mental 5: 22-26.
- Downs J (2014) Creación y Apoyo de los Grupos de Escucha de Voces. Guía para crear y facilitar los grupos de escucha de voces. (Ed: Julie Downs). Hearing Voices Network. Available online at: https://primeravocal.org/wpcontent/uploads/2013/11/grupos-de-escuchadores-de-voces_primera-vocal.pdf
- Martínez-Barbero MA, Coca MC, Pérez G, Martínez MV (2017) Escuchando la voz de las personas que escuchan voces. Rev. Asoc. Esp. Neuropsiq 37 (131): 39-61.
- Norman RM, Manchanda R (2016) Prevention and Early Intervention Program for Psychoses (PEPP). Healthcare Quart (Toronto, Ont.) 18: 37-41.
- Voice Collective (2021) A straight talking introduction: for parents, careers and family members of young people who hear voices or see visions. Available online at: https://www.voicecollective.co.uk
- Romero-Palomino S (2021) Alternativas al silencio. Experiencia con un grupo de escuchadores de voces en una unidad de rehabilitación hospitalaria. Revista de la Federación Española de Asociaciones de Rehabilitación Psicosocial (FEARP) 17: 1.
- Camarzana S (2016) The Hearing Voices Coffee (The experience of Dora García). In; El Cultural (Journalistic report).
- Oakland L, Berry K (2015) “Lifting the veil”: A qualitative analysis of experiences in Hearing Voices Network groups. Psychosis 7(2): 119-129.
- Rácz J, Kaló Z, Kassai S, Kiss M, Pintér JN (2017) The experience of voice hearing and the role of self-help group: An interpretative phenomenological analysis. Int J Soc Psychiatry 63(4): 307-313.
- Jackson LJ, Hayward M, Cooke A (2011) Developing positive relationships with voices: A preliminary Grounded Theory. Int J Soc Psychiatry 57(5): 487-495.
- Valavanis S, Thompson C, Murray CD (2019) Positive aspects of voice-hearing: A qualitative meta synthesis. Ment Health Relig Cult 22(2): 208-225.
- de Jager A, Rhodes P, Beavan V, Holmes D, McCabe K, et al. (2016) Investigating the Lived Experience of Recovery in People Who Hear Voices. Qual Health Res 26: 1409-1423.
- Wykes T, Parr A, Landau S (1999) Group treatment of auditory hallucinations: Exploratory study of effectiveness. Br J Psychiatry 175: 180-185.
- Haddock G, McCarron J, Tarrier N, Faragher EB (1999) Scales to measure dimensions of hallucinations and delusions: The psychotic symptom rating scales (PSYRATS). Psychol Med 29(4): 879-889.
- Ventura J, Green MF, Shaner A, Liberman RP (1993) Training and quality assurance with the Brief Psychiatric Rating Scale: “The drift busters”. Int J Method Psychiatr Res 3(4): 221-244.
- Birchwood M, Smith J, Drury V, Healy J, Macmillan F, et al. (1994) A self-report Insight Scale for psychosis: reliability, validity and sensitivity to change. Acta Psychiatrica Scandinavica 89(1): 62-67.
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J (1961) An inventory for measuring depression. Arch General Psychiatry 4: 561-571.
- Beck AT, Epstein N, Brown G, Steer RA (1988) An inventory for measuring clinical anxiety: Psychometric properties. J Consult Clin Psychol 56(6): 893-897.
- Rosenberg M (1965) Rosenberg Self-Esteem Scale (RSES). APA PsycTests.
- Goodliffe L, Hayward M, Brown D, Turton W, Dannahy L (2010) Group person-based cognitive therapy for distressing voices: views from the hearers. Psychother Res J Soc Psychother Res 20(4): 447-461.
- Perron B, Munson M (2006) Coping with voices: A group approach for managing auditory hallucinations. Am J Psychiatr Rehabil 9(3): 241-258.
- Barros C, Domont O (2014) Hearing voices: A study on exchanges of experiences in a virtual environment. Interface Commun Health Educ 18 (50): 557-569.
- Thomas N, Bless JJ, Alderson-Day B, Bell IH, Cella M, et al. (2019). Potential Applications of Digital Technology in Assessment, Treatment, and Self-help for Hallucinations. Schizophrenia Bull 45(45 Suppl 1): 32-42.
- Longden E, Read J, Dillon J (2018) Assessing the Impact and Effectiveness of Hearing Voices Network Self Help Groups. Commun Mental Health J 54(2): 184-188.
- Atienza FL, Moreno Y, Balaguer I (2000) Análisis de la dimensionalidad de la Escala de Autoestima de Rosenberg en una muestra de adolescentes valencianos. Rev Psicol Universitas Tarraconensis 22: 29-42.
- Escher S, Romme M (1998) Entrevista con una persona que escucha voces. Universidad de Maastricht. Holanda. Versión española (2005) Fundación para la Investigación y Tratamiento de la Esquizofrenia y otros Trastornos Psicóticos.
- Recherches sur l'entente de voix. Annales MédicoPsychologiques, Revue Psychiatrique, Elsevier Masson 171(9): 629-634.
- García Montes JM, Pérez Álvarez M (2001) ACT como tratamiento de síntomas psicóticos. El caso de las alucinaciones auditivas. Análisis y modificación de conducta 27 (113): 455-472.
- In: Read J, Mosher LR, Bentall RP (editores). Modelos de Locura. Barcelona: Herder pp: 181-195.
- Jenner JA (2017) Terapia integradora focalizada en las alucinaciones (Jenner JA. Ed.). Madrid: Fundación para la Investigación y el Tratamiento de la Esquizofrenia y Otros Trastornos Psicóticos.
- Murgieri M (2010) Versión adaptada de la Escala WHOQOL-BREF. The World Health Organization Quality of Life. World Health Organization. (Original version 2004). Servicio Andaluz de Salud.
- Touriño R, Acosta F, Giráldez A, Álvarez J, González J, et al. (2018) Riesgo suicida, desesperanza y depresión en pacientes con esquizofrenia y autoestigma. Actas Españolas de Psiquiatría 46(2): 33-41.











QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Allergy Research (ISSN:2642-326X)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)


