
5746
Views & Citations4746
Likes & Shares
There was no further CNS injury through the MS during the two years of CDT. It is unclear whether the degenerative disease MS was cured or only stopped through CDT. To be on the save side, the patient should continue CDT for at least a few years. The movement-based learning therapy CDT is anyway healthy and prolongs life by 10 to 20 years.
Keywords: Human repair-neurophysiology, Electrophysiology, Single-nerve fiber action potentials, Coordination dynamics therapy, System theory of pattern formation, Coordination dynamics, Multiple sclerosis repair, Spinal cord injury
Based on human repair-neurophysiology [1,2], a movement-based learning therapy was developed though neural network learning [3], called Coordination Dynamics Therapy (CDT), with which it is possible to improve or repair central nervous system (CNS) functioning after stroke [4], traumatic brain injury [5,6], spinal cord injury [7-13] (Figure 1A-D), cerebellar injury/atrophy [14,15] (Figure 1E-H), cerebral palsy [16], hypoxic brain injury [17], in Parkinson’s disease [18], spina bifida (myelomeningocele) [19] and scoliosis [20]. Speech had been induced and improved in a patient with severe cerebral palsy [1]. A permanent coma patient could be brought out-of-coma and relearned to speak and move [21-26] and cancer grows could be inhibited through CDT [22,23] by improving cardio-vascular performance [1,21] and building of natural killer cells [24]. Urinary bladder functions [1] could be cured in cerebral palsy [1] and spinal cord injury [7,12,13]. There is indication that general health can be improved via CDT to live longer with a better quality of life [25] and euthanasia avoided in organ donation [26]. Basal ganglia injury was also repaired [27], spinal muscular atrophy stopped [28] and incontinence repaired [29,30].
A further repair step through human repair-neurophysiology is to repair degenerative diseases. It was shown that spinal muscular atrophy could be stopped through continuous training [28]. It will be shown that CDT may also stop multiple sclerosis.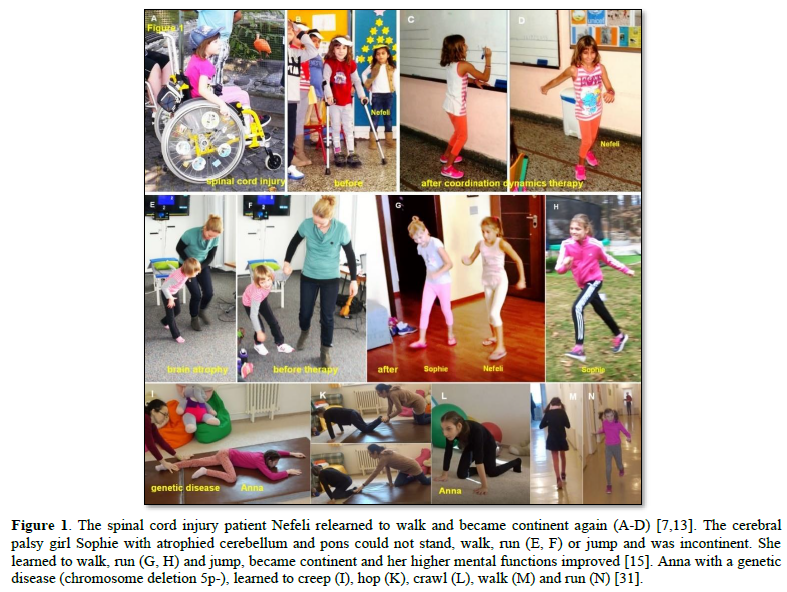
The name "multiple sclerosis" (MS) is short for multiple cerebro-spinal sclerosis, which refers to the numerous glial scars (or sclerae-essentially plaques or lesions) that develop on the white matter of the brain and spinal cord.
A person with MS can have almost any neurological symptom or sign, with autonomic, visual, motor, and sensory problems being the most common. The specific symptoms are determined by the locations of the lesions within the nervous system, and may include loss of sensitivity or changes in sensation, difficulty in moving, difficulties with coordination, and balance (ataxia), visual problems, bladder and bowel difficulties, among others. When multiple sclerosis is more advanced, walking difficulties can occur and the risk of falling increases.
MS is the most common demyelinating disease in which the insulating covers of nerve cells in the brain and spinal cord are damaged. This damage disrupts the ability of parts of the nervous system to transmit signals and impairs the coordination of neuron firing, resulting in a range of sign and symptoms, including physical, mental, and sometimes psychiatric problems.
MS is the most common immune-mediated disorder affecting the CNS and is supposed to be difficult to repair [33-35]. But CDT improves many of the occurring symptoms also the immune system because cancer grows could be inhibited [22,23]. Through movement-based learning NK cells are built [24] and the cardio-vascular performance improved. A fundamental repair step is in work to see whether a gene defect can be repaired (Figure 1, I-N) through movement-induced epigenetic modification for changing gene expression [31]. Whether epigenetic modification for changing gene expression [32] is partly possible can only be found out in human patients when administering optimal therapy. An optimal movement-based therapy is if a therapy is efficient and applied at the limit for a few years.
CDT attempts to improve function after the attacks and prevent new attacks. It will be shown that CDT improved CNS functioning. Whether CDT can prevent new attacks, longer treatment than two years of CDT is needed. In these two years no, further attack occurred.
In the Method it will be shown that CDT is based on human repair-neurophysiology and in the Results, details of the improvements of CNS functioning through therapy are given. In the Discussion the repair of this MS patient will be compared with repair in spinal muscular atrophy, incomplete spinal cord injury, and genetic disease.
METHOD
Coordination dynamics therapy is neurotherapy to repair the human nervous system which is based on human repair-neurophysiology. Since therapists seem not to be familiar with this new development, a short introduction is given.
Movement-based learning strategies to repair the human CNS
To repair the human CNS, several strategies are used. First, to repair the always impaired phase and frequency coordination (a principle of CNS organization) through exercising on a special coordination dynamic therapy (CDT) device (Figure 2). Second, to train important automatisms during ontogenetic development like creeping, crawling, up-righting, walking, running and breathing, because genetic support can be expected and repair shows similarities to ontogenetic development. Third, to repair the especially phylogenetic old CNS structures like the spinal cord, the vermis of the cerebellum and the paleostriatum (globus pallidus) of the basal ganglia, movements must be trained, which phylogenetic ancestors like Tiktaalik, may have used for locomotion. Such movements are creeping, salamander crawling, hopping and others. Fourth, to activate and train important regulation circuits, which, for example, are activated during jumping. Jumping helps to repair urinary bladder and other functions. Fifth,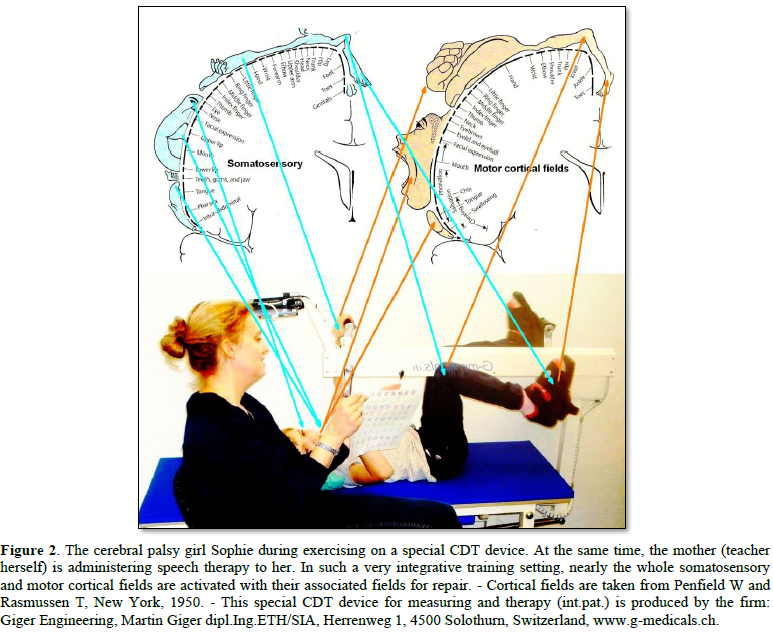
The nervous system must recognize which structures or regulation units are deficient, to repair them by error elimination processes. Movement-based learning in combination with instructive training (1-2-3-.), visual (mirror) and auditive (music) feed-back increases the efficiency of treatment.
Repair of phase and frequency coordination through exercising on special CDT devices
The first and most important movement, to be trained during repair, is the exercising on a special CDT device to repair the coordinated firing of neurons, namely, the phase and frequency coordination (Figure 2). This new repair strategy is based on a new development in human neurophysiology with which it is possible to record the impulse traffic among neurons at the single-neuron level (Figure 3).
Human Neurophysiology
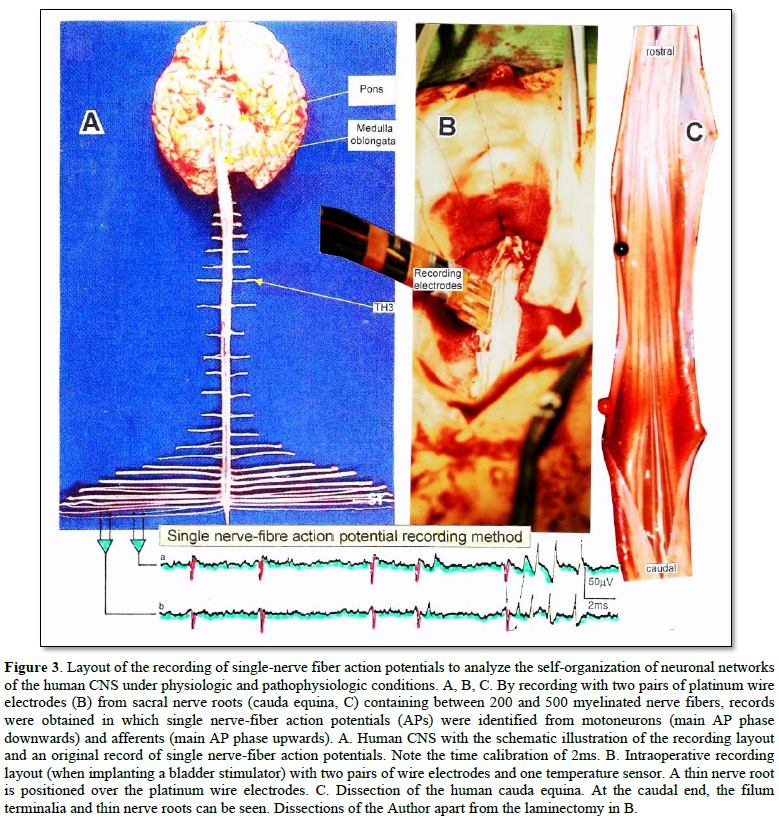
With the single-nerve fiber action potential recording method, single-nerve fiber action potentials can be recorded from sacral nerve roots, running in and out of the spinal cord (Figure 3) [36].
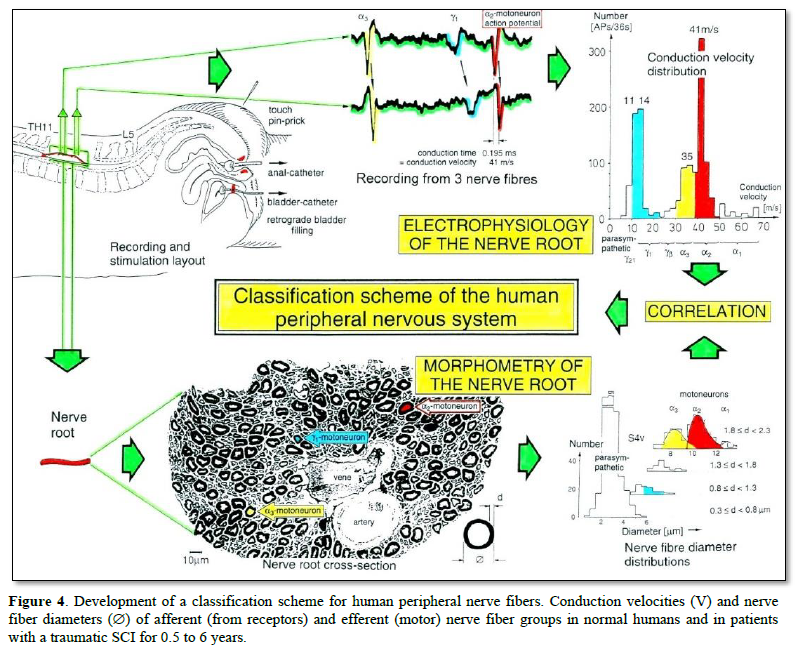
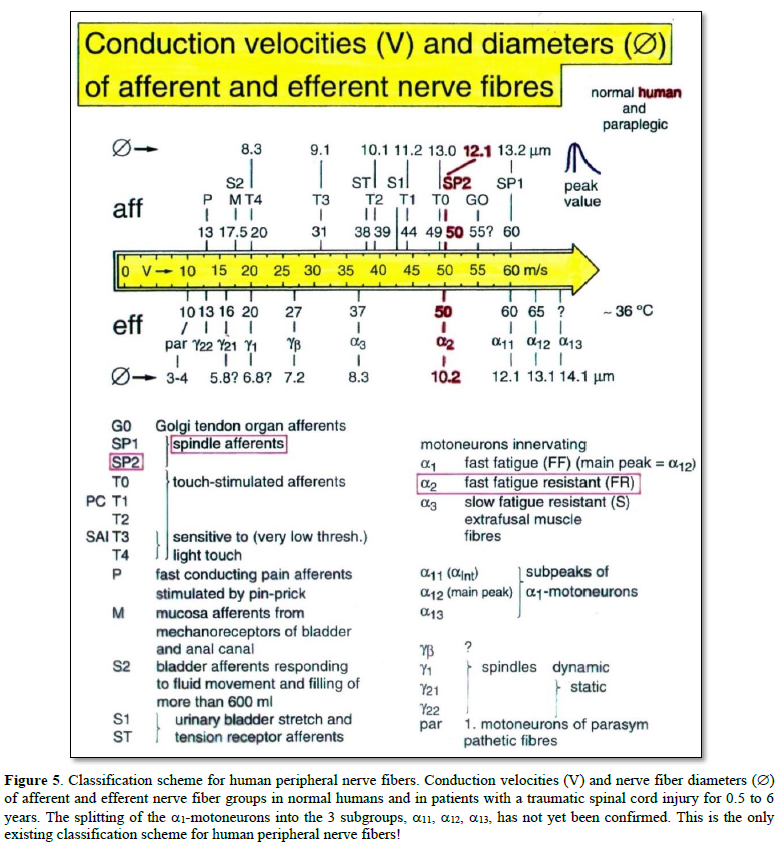
By measuring the conduction times and with the known electrode pair distance of 10 mm, conduction velocity distribution histograms were constructed in which the myelinated nerve fiber groups larger than 4mm could be characterized by group conduction velocity values (Figure 4). After the recording, morphometry was performed. Distributions of nerve fiber diameters were constructed and nerve fiber groups were characterized by the peak values of asymmetrical distributions (Figure 4). By correlating the peak values of the conduction velocity distributions with those of the diameter distributions, obtained for the same root, a classification scheme was constructed for the human peripheral nervous system (Figure 5) [37-39]; the only existing one for human peripheral nerve fibers.
This classification and identification scheme represent a solid basis for classifying and identifying nerve fiber groups in the human peripheral nervous system and analyzing CNS functions at the single-neuron level. It became thus possible to record natural impulse patterns simultaneously from identified single afferent and efferent nerve fibers and analyze self-organizing mechanisms of the human CNS under physiologic and pathologic conditions.
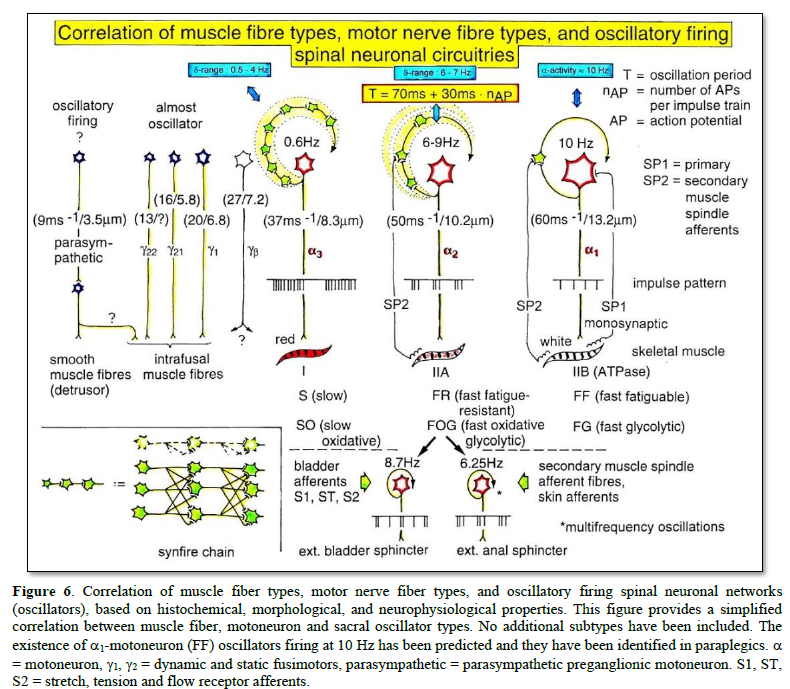
The most important finding with the single-nerve fiber action potential recording method was that nerve cells in the human CNS are organizing themselves through “Phase and Frequency Coordination” [40,41]. In nerve fibers, this phase and frequency coordination can easily be measured, because the three motoneuron types fire for high activation oscillatory [42] and offer in this way a structure to which the timed firing of neurons can be related to. Since the α2-motoneuron oscillations are most stable, firing phases of neurons are related best to the α2-motoneuron firings.
Figure 6 shows schematically the oscillatory firing patterns of the three kinds of motoneurons and the muscle fiber types they innervate.
By comparing CNS functioning in brain-dead humans (where the spinal cord is functioning rather physiologically) and patients with spinal cord injury, injury-induced changes of CNS functioning can be measured and partly repaired. Mainly the phase and frequency coordination of neuron firing becomes impaired following injury. This impaired coordination among neuron firings can efficiently be repaired through exercising on a special CDT device (Figure 2).
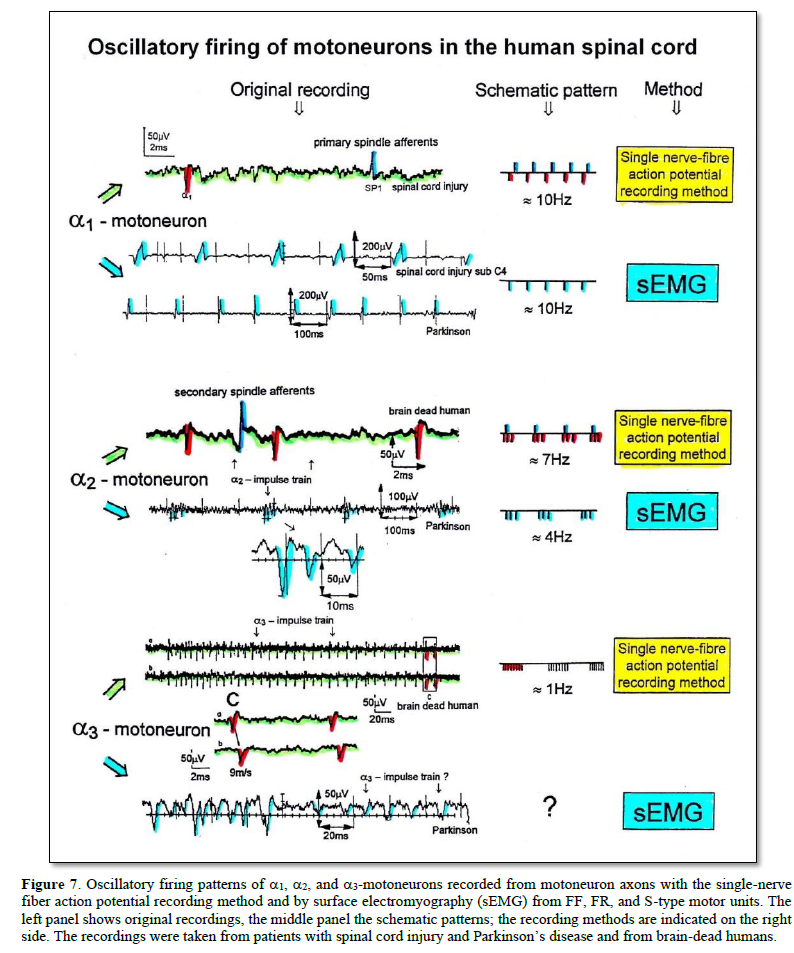
The drawing back of the single-nerve fiber action potential recording method is that it is an invasive recording method. But with the surface electromyography (sEMG) [43] one can record non-invasively coordinated firing among motoneurons via their motor units if one records from suitable patients, like incomplete spinal cord injury patients, when a certain muscle is only innervated by a few motoneurons.
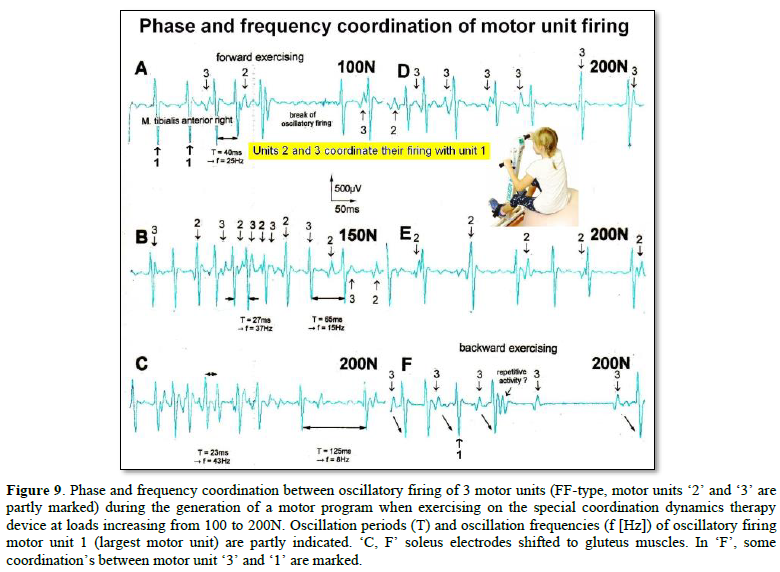
In Figure 7, the recordings from motoneurons and motor units are compared. The firing patterns of α1, α2 and α3-motoneurons can easily recorded with the single-nerve fiber action potential recording method but not with the sEMG (Figure 7). From spinal cord injury patients, on the other hand, single-motor unit APs can be easily recorded from α1 motor units but not from α2 and α3 motor units (Figure 7), because their AP amplitude seems to be too small. Clinical sEMG recordings therefore show mainly the activity of α1 motor units. The phase and frequency coordination among neuron firings can be measured in human with the single-nerve fiber action potential recording method (Figure 8) and with surface EMG (Figure 9).
The neural networks of the human brain organize themselves by phase and frequency coordination among neuron firings and neural subnetworks as for example the network oscillators of which the motoneuron is a part. This coordination is achieved by the organization tendencies of the network, the descending impulse patterns from the brain and the spatiotemporal afferent impulse patterns from the periphery.
If the premotor spinal oscillators would not coordinate their firing and synchronize their firing for longer periods of time, tremor would occur. Such pathologic synchronization can be observed in patients with Parkinson’s disease [41,44].
If the neural networks are damaged by trauma, degeneration or malformation, the coordination between neuron firings becomes impaired and has to be repaired by movement-based learning (CDT). Drugs and operations cannot repair neural network functioning.
The generation of motor patterns of α1-motoneuron firings with increasing load and the phase and frequency coordination among single-motor unit firings can be recorded with sEMG (Figure 9).
Integrative Physiology: System Theory of Pattern Formation
To understand the on-going changes of movement and other patterns in healthy humans and in patients with CNS injury, malformation and degeneration (aging), the System Theory of Pattern Formation is used for understanding neuronal network organization and learning for repair.
In a complex system like the human CNS, patterns are generated by a nervous system which seeks cooperative stability. Stability is what defines collective states. The system has the tendency to slip into the collective states to which it is attracted. When an infant crawl, its arms and legs are strongly attracted to the ‘pace’ and ‘trot’ gait patterns. The attraction is so strong that intermediate crawling patterns seemingly do not exist, as if the patterns are hard-wired. But with the help of the special CDT device the CNS can generate intermediate coordination patterns. A patient with a CNS injury often crawls with intermediate arm and leg coordination patterns and has to re-learn the pace and trot gait coordination’s for CNS repair and shifts in this way the attractors for crawling to the pace and trot gait coordination’s. Attractive states and attractors of CNS organization can be pictured as a ball in a potential well or more generally in an attractor layout (Figure 10). Changes in CNS functioning are characterized as continuous stabilization and destabilization, over time, of preferred attractor states.
If for example a therapist is crawling in interpersonal coordination with a cerebral palsy girl, the learning process is speed up. The visual input from the exact crawling of the therapist into the CNS of the girl improves the performance of the crawling pattern. For this supervised learning the cerebral palsy girl needs not to concentrate to it. It is working automatically. This interpersonal coordination is something like when soldiers march together. Once they got the rhythm among each other, the marching coordination works automatically. It was even reported that soldiers could march together in interpersonal coordination when half sleeping.
This supervised teaching of the therapist, so that the patient learns faster needs a lot of concentration. The therapist has to copy the pattern of the patient and has to drag her then into a better performance. In doing so, the therapist sometimes is also losing the own movement pattern. With the concentration on the patient and adapting partly to the pattern of the patient, the stability of the own movement pattern is reducing strongly and easily lost.
To reduce for understanding the complexity of human neural networks of the many billions of neurons, order parameters or collective variables are introduced for the generation of certain movements. An equation of motion describes the coordination patterns dynamics. However, coordination patterns are not only determined by the task or biological function. Patterns adjust continuously to requirements from the environment (transmitted by impulse patterns from stimulated receptors in the periphery), memory, intention, and support given by a therapist. The specific requirements are captured by the concept of behavioral information and are made part of a vector field that attracts toward the required patterns. The coordination pattern dynamics, characterized by equations of motion of collective variables (the vector X), takes the general following form [45]:

where Fintr designates the intrinsic dynamics of the nervous system. These intrinsic dynamics capture the anatomical (neural network structure), physiological and pathological states of the CNS and its muscular-skeletal elements.
∑cinfFinf(X,t) represents the sum of external influences (Finf(X,t)) with their relative strength (cinf) pertaining to each influence. The so-called behavioral information Finf(X,t) includes cognitive states, emotional states, intentions, motivations, instructions, inter-personal coordination, movement support etc. During motor learning or while applying therapy to a patient these extrinsic influences become extremely important, because the intrinsic (pattern) dynamics can be changed with these extrinsic influences by altering the equation of motion. By modulating the behavioral information, the intrinsic dynamics of the neuronal networks can be influenced further, that is if CDT is no longer efficient in repairing the injured CNS, the therapy has to be updated. With respect to a healthy athlete, the movement performance can be improved by modulating the behavioral information by for example including in the training program the exercising on a special CDT device to improve CNS functioning.
If the behavioral information includes the exercising of extremely coordinated, integrative movements, like exercising on the special CDT device, the quality of CNS self-organization can be enhanced by improving the exactness of self-organization, namely the precision of phase and frequency coordination between neuron and neural assembly firings. By improving the precision of organization of the intrinsic dynamics, that is the specific variability of the injured networks, certain patterns do eventually re-appear in the case of repairing the injured CNS by movement-based learning.
Learning implications for treatment derived from the equations of motion of the collective variables in the framework of System Theory of Pattern Formation
- Behavioral requirements Finf (like intention, support, and instruction) affect the whole coordination dynamics, including stability, rather than only certain coordination patterns. The change of the whole coordination pattern dynamics of the CNS by the behavioral information is one scientific basis for learning transfer between different patterns and stability changes of patterns (as for example the reduction of spasticity). The other scientific basis for learning transfer is followed from human neurophysiology, namely that nerve cells or neural sub-networks are involved in different neural network organizations [1-3].
- Intrinsic coordination tendencies captured by the intrinsic dynamics influence the performed pattern systematically because the degree to which intrinsic tendencies conflict or agree with the required patterns determines the variability of the performed coordination pattern.
- A reduction in stability of movements and other patterns when intrinsic and informational requirements conflict, may lead to loss of stability and abrupt change while behavioral information is changing smoothly.
- The intrinsic dynamics Fintr include vegetative and higher mental functions (these are also patterning of the coordination dynamics), which indicate that via exercising coordinated movements with support and/or instructions (Finf), urinary bladder function, intelligence and speech may be partly repaired or improved following CNS injury or malformation.
- When in an injured CNS with a certain set of behavioral information (∑cinfFinf) the intrinsic coordination dynamics (Fintr) can no longer be influenced during coordination dynamics therapy, then this set of behavioral information has to be changed (using different Finf), or balanced differently (using different cinf), to further improve CNS organization dynamics.
- However, the equations of motion of the coordination pattern dynamics (formula 2) provide no information about the specific behavioral information (Finf) and training intensity (cinf) with which the CNS can be efficiently repaired by learning in the patient. We need to have detailed knowledge of the human CNS at the single neuron and neural assembly level [1-3], as well as knowledge at the integrative level, to find the specific behavioral information for the repair by learning of the human CNS.
A first novel step in coordination dynamics therapy is the inference derived from the formula 2 of the equation of motion. It suggests that the movement learning not only improves the performance of that movement, but also improves other non-trainable functions by learning transfer [46]. These functions include vegetative functions like urinary bladder control, speech (if the patient cannot speak) and higher mental functions.
Furthermore, we have means by which the stability of physiological network states can be increased (e.g., movements, continence, continuous concentration in performing certain tasks, speech etc.) and simultaneously the stability of pathological network states, like spasticity, decreased. The coordination (pattern) dynamics therapy, partly based on the System Theory of Pattern Formation in combination with human neurophysiology (including neuro-urology), thus offers us an important theoretical basis and a practical tool to diagnose, quantify and repair/improve the functioning of the human nervous system at the macroscopic level. Through neural network learning we can reach for repair the whole CNS, including the sacral and pontine micturition centers and the plexuses outside the CNS.
From the repair by learning in the severely injured CNS we can learn about learning in the healthy CNS.
Geographical landscape of attractors
The drawback of the equation of motion of the order parameters (formula 2) is that it is normally not possible to find a mathematical solution to it. But by defining a potential function and by picturing the attractive states and attractors by a ball in a potential well or rather by a ball moving in a geographical landscape of attractors (Figure 6), we form a theoretical basis to understand and measure stability of certain coordinated movement patterns (i.e., the deepness of the potential well of an attractor) in patients with CNS injury who receive on-going therapy.
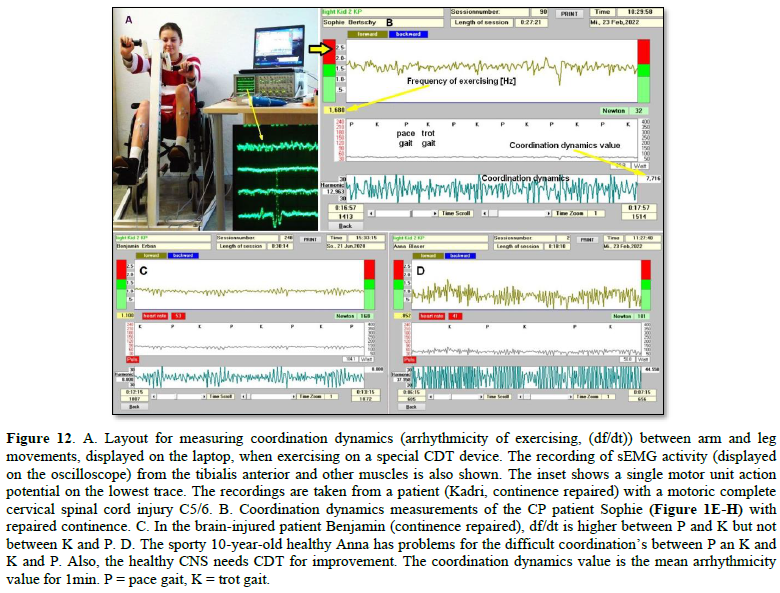
By studying the pattern change of certain highly coordinated arm and leg movements, while a subject is exercising on a special coordination dynamics therapy device (Figure 8A), pattern stability can be made visible and the mean stability per one minute can be measured by the arrhythmicity of exercising (see below). Such value, so-called coordination dynamics value, quantifies CNS functioning objectively, integrative, and non-invasively. The assessment of quality of CNS organization by pattern change is a second novel step in CDT.
To make the strategy of pattern formation, pattern stability, pattern assessment, and pattern picturing understandable, the procedure is demonstrated for the simple movement ‘jumping on springboard’, which is used during CDT, especially for the repair of the urinary bladder and training in the up-right weight-bearing posture (very important in patients with SCI).
Equation of motion, potential function and attractor layout for the movement ‘jumping on springboard’
For the special movement ‘jumping on springboard’ with no behavioral information ( = 0) the equations of motion (formula 2) take the form:
Where φ is the relative phase between the two moving legs and is the only collective variable of this special movement.
The mathematical solution of in the Haken-Kelso-Bunz model [45,47] (for the approximations being made) gives the equation of motion for jumping on springboard for the space-time symmetry:
The so-called potential function is defined by
By integration we obtain the potential function for jumping on a springboard:
For an easy understanding, the potential function can be developed approximately as follows. With the space-time symmetry V(φ+2π) = V(φ) (time symmetry) and V(φ) = V(-φ) (space symmetry) and using the first two terms of the Fourier series with sines and cosines we obtain by regarding that only cosines are invariant when φ is replace by – φ. The minus signs allow to interpret the function, V, as a landscape with attractor states for positive values of a and b [45].
The potential function can be plotted for different φ and certain ratios of the parameters a and b and is shown in Figure 6. The variability of the pattern state jumping, caused by phase and frequency variability, is made visible by arrows in Figure 10.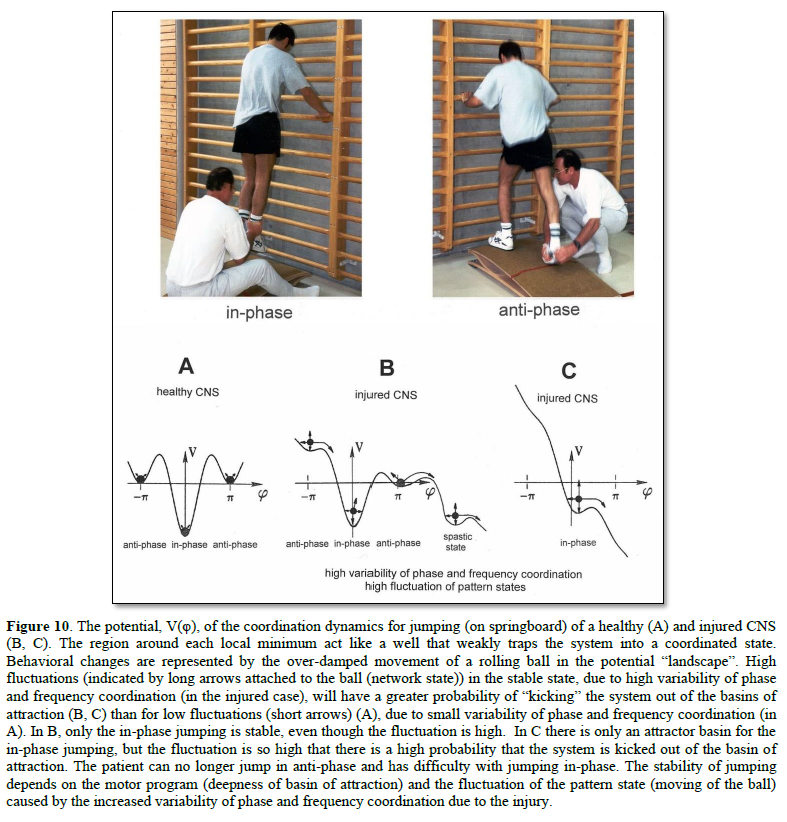
In the healthy CNS, the phase and frequency variability are small (short arrows) and the jumping in-phase and anti-phase is stable (Figure 10A). Following injury, the potential landscape is deformed and the fluctuation of the network states, generating jumping, is high (Figure 10B). The in-phase jumping is still stable despite the increased fluctuation, because the basin of attraction is deep. The jumping anti-phase became unstable because the basin of attraction is shallow and the increased fluctuation in the state has a greater probability of “kicking” the system out of the basin. A switch into a spastic state is also possible. In severe CNS injury or malformation, the patient cannot jump any more in anti-phase because of the missing of attractors for anti-phase jumping (Figure 10C). Support is needed for anti-phase jumping (Figure 10, upper right). The jumping in-phase is still possible but unstable (Figure 10, upper left).
Upon performing very exact coordinated movements, imposed by devices, the nervous system of the patient learns to reduce the variability of phase and frequency coordination and achieves in this way a small fluctuation of the network states again as shown in Figure 10A. The progress in treatment (learning) is that the in-phase jumping in Figure 10C and the anti-phase jumping in Figure 10B become stable (Figure 10A) again. Also, the potential landscape will change due to the reduction of the phase and frequency variability. The important consequence for treatment is that when exercising on special CDT devices and reducing in this way the variability of phase and frequency coordination, the patient can induce the formation of patterns again, without having trained them (learning transfer). Through improving the coordinated firing of neurons, a cerebral palsy child will become continent and my become able to speak or may develop social behaviors.
In conclusion, the impairment of phase and frequency coordination, measured at the neuron level in human, can be included in the coordination dynamics at the collective variable level. The decrease of the variability of phase and frequency coordination (one kind of coordination repair) is an essential part of CNS development and repair by movement-based learning (neural network repair).
Movements to be trained
Movements have to be trained which improve the coordinated firing of neurons, the phase and frequency coordination, and which make it possible that other parts of the brain/CNS take function over through plasticity. The phase and frequency coordination can be improved when patients exercise on a special coordination dynamics therapy device (Figure 11). The nervous system learns from the device to function more physiologically, including the sacral and the pontine micturition centers. With the repair of the phase and frequency coordination, some patterns, including continence patterns, already re-appear.

In severe central nervous system injury or lost brain parts, other parts of the nervous system have to take function over by plasticity. Therefore, also other arm, leg and trunk movements have to be trained as the automatisms creeping, crawling, walking, running and jumping with or without support. For bladder repair the exercising on the special device and the jumping on springboard are most important (Figures 10 & 11). The jumping on springboard activates the pelvic floor muscles rhythmically, of which the external bladder and anal sphincters are a part. When exercising on a special device, the neural networks of the central nervous system are activated and repaired in the deep complexity of neural network organization. This is achieved because arm and leg movements change their coordination between the pace and trot gait patterns. Through this pattern change, according to the system theory of pattern formation, the quality of CNS functioning can be measured through pattern change by a single value (see below). The movement-based learning process is optimal by training 15 to 20 hours per week.
Unique properties of special CDT devices
The special CDT device has four important properties.
First, the patient performs coordinated arm, leg and trunk movements when exercising on it. The training of integrative patterns takes care of that the pathologic organization cannot escape from repair by shifting to another part of the CNS and the whole CNS, including the injured parts, is reorganized so that other CNS parts can take function over through plasticity.
Second, neurons are coordination detectors. Because the mechanical coordination between arm handles and leg pedals is extremely exact, the generated time-coordinated afferent input endplate potentials onto a neuron in the neural networks (approximately 5ms long) overlap more. The excitation threshold of the neuron is reached earlier. In this way, the efficiency of organization is improved. In spinal cord injury, for example, the transmission over the injury site will increase. If the mechanical coordination between arm handles and leg pedals of the device is not extremely exact any more, then the turning is only a muscle training and not a training through which the nervous system can learn from the device to function better. Maintenance of the device and supervision by an educated therapist is necessary.
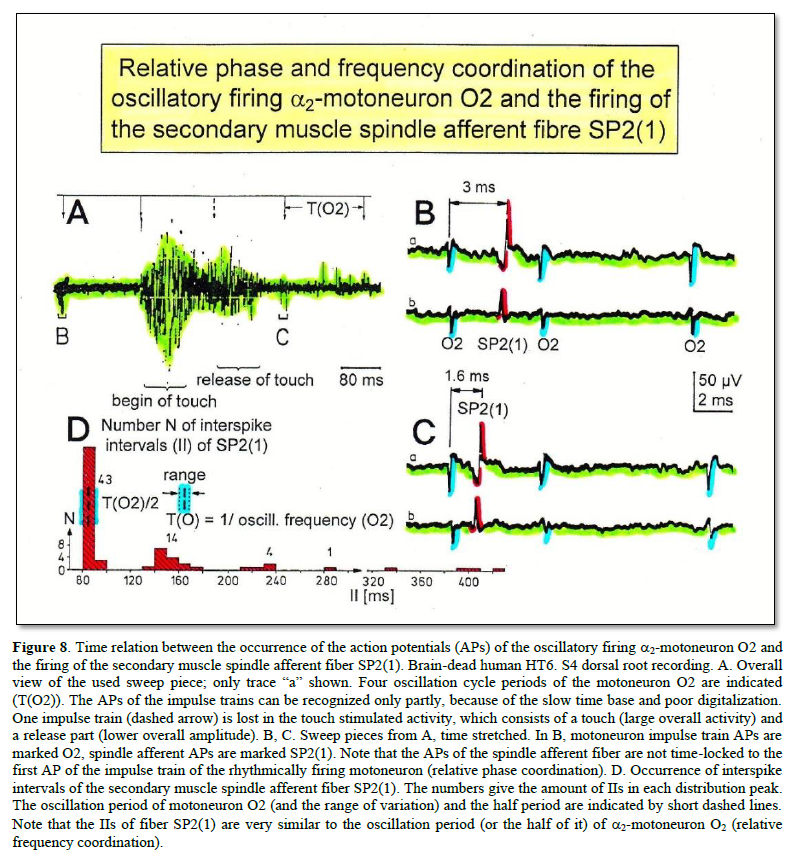
Third, the coordination between arm and leg movements changes from pace to trot gait, imposed by the device. The intermediate coordination patterns between pace and trot gait are difficult to generate for the CNS neural networks. If the patients CNS learns to generate these intermediate patterns, imposed by the device, then the neural networks have learned to function better (more precise) in the deep complexity of CNS organization. The patient’s nervous system learns by turning from the device, to function more physiologic through improving especially the phase and frequency coordination among neuron firings. This phase and frequency coordination can be measured by single-motor unit surface electromyography non-invasively (Figure 9) and by the single-nerve fiber action potential recording method invasively (Figure 8). In Figure 8 the coordinated firing between a motoneuron and spindle afferent fiber was recorded and measured. This spindle afferent fiber contributed to the drive of the motoneuron, because of the constant phase drive. In Figures 8B & C, the phase variation was 1.4ms (3-1.6ms).
Fourth, the practical assessment of quality of CNS organization by pattern change, when exercising on the special CDT device, is a third novel step in coordination dynamics therapy.
Measuring CNS functioning by the arrhythmicity of exercising (coordination dynamics value)
The impaired phase and frequency coordination at the single neuron level, the assembly level and the macroscopic level can be measured macroscopically when the patient is exercising on a special coordination dynamics therapy device (Figure 12) on which arms and legs turn with a slightly different frequency (transmission 19 (arms): 18 (legs)). The phase coordination between arms and legs is imposed by the device. The loss of phase and frequency coordination between arm and leg movements becomes visible and measurable by the arrhythmicity of turning. During a turning cycle, the coordination between arms and legs changes between pace (P) and trot gait (K). According to the difficulty of the coordination, the turning frequency increases and decreases. This frequency variation (df/dt; f = frequency) can be recorded, quantified and displayed on a computer screen (Figure 12A) and is called coordination dynamics value. CNS functioning is therefore measured though pattern change (continuous pattern changes from trot gait to pace gait) according to the System Theory of Pattern Formation.
Brain-injured and healthy persons have problems with this difficult intermediate coordination’s between pace and trot gait, especially for higher loads (Newton) (Figures 12C & D), because the deep complexity of CNS organization is needed to generate these movement patterns. In reverse, if brain-injured patients learned to generate these difficult coordination’s, then their CNS improved in its functioning in the deep complexity of CNS organization.
During the functional reorganization of the injured CNS of patients, the relative phase and frequency coordination among neuron firings has to be entrained as exactly as possible by the movement induced afferent impulse patterns from the receptors (learning through feedback information) to restore coordination in the range between 3 to 5 milliseconds (approximate lengths of postsynaptic potentials).
The device has therefore to impose the exercising patient a coordination in the millisecond range for the different coordination’s of arm and leg movements between pace gait and trot gait. The easy pace and trot gait coordination’s, but not the difficult intermediate coordination’s, can often be performed by the patient easily. Therefore, the continuous change from the easy to the difficult coordination’s diagnoses the capability of the CNS to organize easy and difficult organizational states. If the movement states can be easily generated by the neuronal networks of the CNS, then the frequency variation of turning is small during the turning cycle, and if the movement state is difficult to be organized by the CNS, then the frequency variation is large (the coordination dynamics value is large).
Repair strategies at the neuron membrane and genetic level
For the repair of the neural networks of the CNS it is likely that excitation-neurogenesis coupling [48-50] contributes, stimulated through CDT.
- Repair depends on learning and memory formation, mediated or supported by epigenetic mechanisms. Epigenetics is the interplay between genes and the environment resulting in phenotype and epigenetic landscape.
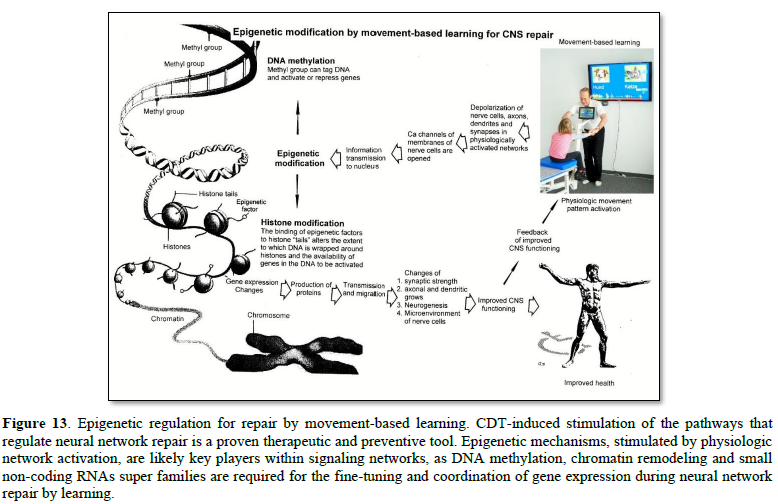
- Epigenetic mechanisms, like DNA methylation, are probably sensors for movement-based learning and memory formation and fine modulators of neurogenesis though CDT (Figure 13).
- The epigenome consists of non-coding RNA and chromatin, a proteinaceous matrix surrounding DNA. The dynamic interactions of post-translationally modified chromatin proteins, covalently modified cytosines inside DNA and non-coding RNA define the complex pattern of gene expression beyond the four bases of DNA.
- The hippocampus plays an essential role in learning and memory. In the hippocampus there exists a specialized form of neural plasticity, which is the generation of new functional neurons from stem cells occurring throughout life. Adult hippocampal neurogenesis contributes to learning and memory formation.
- New neurons are important for learning and memory formation (besides functional reorganization), i.e., for increasing the rate of repair, for the following reasons:
- The insertion of new neurons helps to store the memory of the same activity that led to the creation of the neuron.
- Activity-dependent neurogenesis enhances the learning of new memories and degradation and clearance of previously stored unwanted memories like spasticity, because the synapses, dendrites and axons can be devoted more fully to the newer memories. The old neurons with large and complex axon and dendritic trees are difficult to change. They can only be changed with sustained effort.
- New neurons seem to improve the accuracy of relearned patterns (from model study [48]). This means that new neurons help to improve phase and frequency coordination of neuron firing and pattern stability.
- The advantage of new neurons seems to be dramatically greater in networks that had been more active and had been required to store more memories [48]. The advantage of neurogenesis for memory storage in heavily active networks is that it provides an increased rate of repair if movement-based learning is administered aggressively and if different movements are trained.
- Specific natural network activity is required for multiple aspects of repair. Specific activity is essential for correct migration of interneurons and it also controls the development and repair of their axons and dendrites. During repair there is a specific requirement of network activity in shaping the cortical integration of specific neural subtypes. Newly build neurons are likely electrically active shortly after their birth and participate in the early network activity that contribute to circuit maturation during repair by CDT.
- Specific activity is required for migration and maturation at several stages of repair. A break in CDT may invalidate the whole chain of repair events. Specific interneuron subtypes require activity for migration and morphological maturation at two distinct stages of development [48]. Newly built neurons may even require specific activity for migration and maturation at several distinct stages of repair. During a break in CDT, the specific activity, required for neuron migration, maturation and network integration may not be supplied at one of these stages so that the chain of repair events is severed and the whole repair chain has to be started anew.
- Drug application may undermine repair. Altering the level of neuronal excitability within genetically targeted neurons from drug application, for example antiepileptic drugs may have profound consequences on multiple aspects of the repair of select types of neurons within a population of neurons, as well as their associated gene expression. The pain-killer ‘Contergan’, taken during pregnancy, changed gene expression and the babies were born without arms.
- Excitation-neurogenesis coupling [48]:
- Excitation increases or decreases neuron production directly by excitation-neurogenesis coupling.
- The excitation acts indirectly on the surrounding mature (hippocampal) cells through depolarization-induced release of growth factors.
- Adult neurogenesis is enhanced by excitatory stimuli and involves Ca2+ channels and NMDA receptors.
- The Ca2+ influx pathways are located on the proliferating stem/progenitor cells (NPCs), allowing them to directly sense and process excitatory stimuli. The Ca2+ signal in NPCs leads to rapid induction of a proneural gene expression pattern.
- Integrative coordinated movements have to be trained to allow functional reorganization and new nerve cell integration across very large distances. CDT has to activate injured and uninjured networks to enhance physiologic CNS functioning and learning transfer.
- Conclusion for optimal therapy according to the present stage of knowledge. If there is similarity between development and repair, animal (mice) data also hold in human and the principles of neurogenesis of the hippocampus also hold in other parts of the brain, albeit to a much lesser extent, then the patient has to be trained at his limits (1) to induce substantial building of new nerve cells [51]. The treatment has to be continuously administered (2) to support all stages of repair at the progenitor level as migration, maturation and integration. The networks requiring repair have to be activated specifically (3) to generate repair-friendly, micro-environmental properties in the neural networks. No drugs should be administered that change neuron excitability (4). The exercises have to include coordinated arm, leg and trunk movements (if possible) to improve the impaired phase and frequency coordination for CNS self-organization (5). The performed movements have to be as integrative as possible to reconnect distant brain parts and to induce learning transfer.
RESULTS
Locations of the injuries at the beginning of therapy
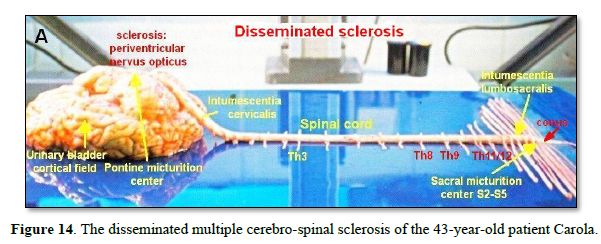
At an age of 43 a relapsing remitting multiple sclerosis (RRMS) was diagnosed in the female patient Carola. She had two attacks of the CNS with disseminated sclerosis at thoracic spinal cord levels 8/9 and 11/12, at the conus medullaris, periventricular and in the nervus opticus. The disseminated multiple cerebro-spinal sclerosis is marked in Figure 14.
To understand more clearly the symptoms from the disseminations of the different sclerosis, Figure 15 shows schematically some CNS places of attack.
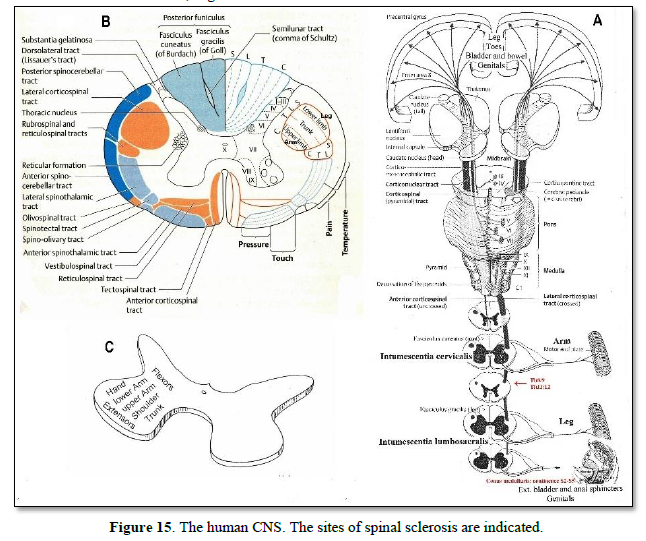
In Figure 15A the levels of spinal cord injuries are indicated. As the spinal cord cross section shows (Figure 15B), there are many different up- and downstream pathways and it is difficult to deduct impaired functions from the patient’s behavior. As will be shown below there was some power weakness in the legs and some dysfunction of sensitivity. She had no continence problems (sclerosis in the conus medullaris) and no strong impairment of vision (sclerosis of nervus opticus). May be the parasympathic innervation of the eyes was impaired because of enlarged pupillae.
Generally, the patient was well up and started at an early stage of disease with CDT to stop the progress of the MS.
MS repair within 2 years of CDT
At an age of 44 coordination dynamics therapy (CDT) was started. Figure 16 shows the improvement of CNS functioning after 2 years of CDT, measured by the coordination dynamics. The frequency variation and the arrhythmicity of turning improved (got smaller) for high load (136N) from 39.1 (Figure 16A) to 29.5 (Figure 16C) for forward exercising and from 23.4 (Figure16B) to 17.1 (Figure 16D) for backward exercising. For a low load of 20N the patient could exercise much better (2.0 and 2.5 (Figures 16E & F)) similarly as in the healthy case.
From Figures 16A-D it can further be seen that the patient could exercise quite good for the pace and trot gait coordination’s and had big problems for the intermediate coordination’s between pace and trot gait. It can further be seen that the patient could turn much better in the backward direction than in the forward direction. Maybe the flexor functions were less impaired than the extensor functions in the spinal cord (Figure 15C).
When comparing the coordination dynamics for high load of the patient with those of the Author for similar high load (Figure 17), the Author had much lower (better) values and that he could manage much better with the difficult intermediate coordination’s. No rhythmic changes can be seen in the Authors coordination dynamics. It is obvious that the cerebro-spinal sclerosis injured the CNS quite much, even though the patient was still well up.
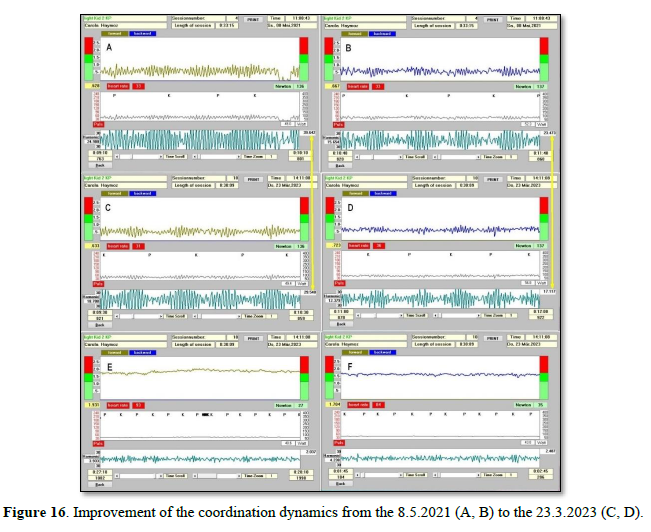
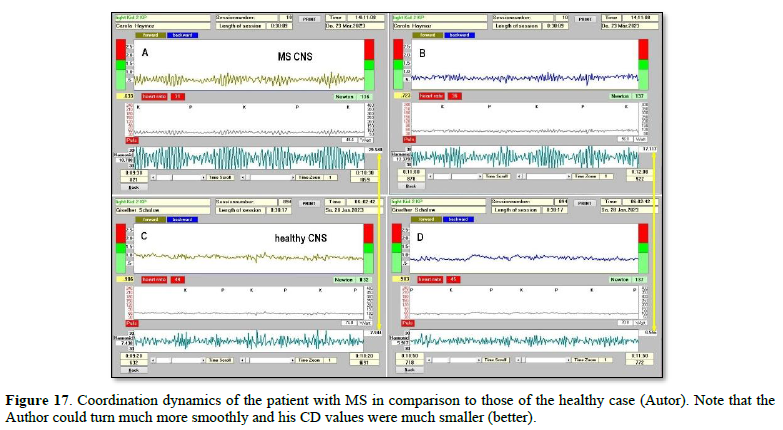
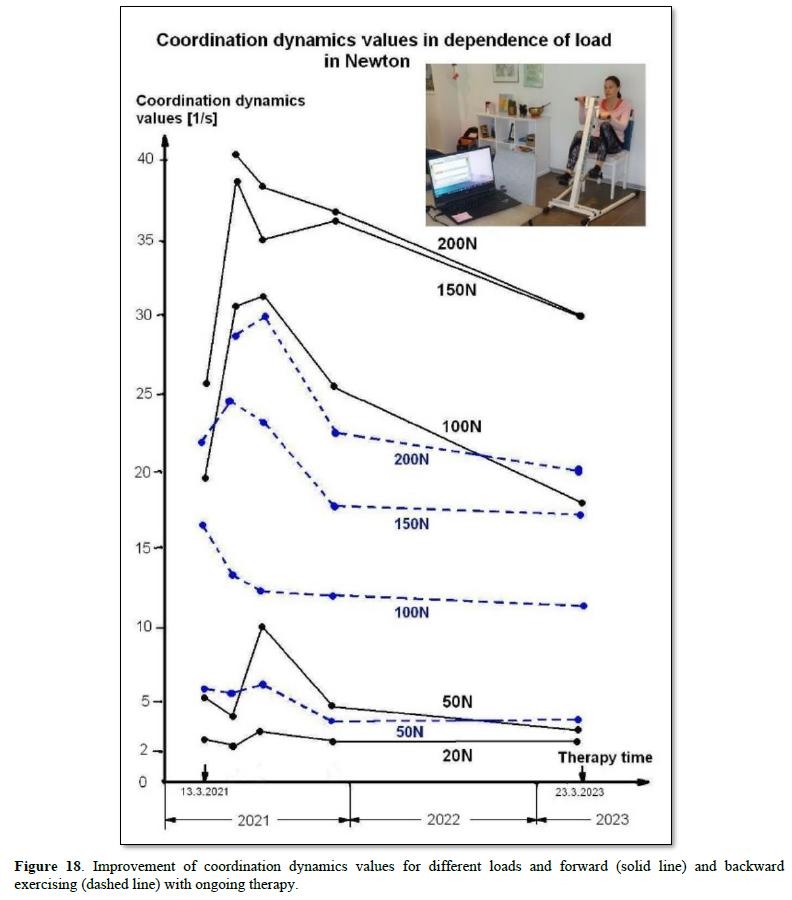
Figure 18 shows the coordination dynamics values for different loads for forward and backward exercising. After a first increase, the CD values got smaller better with therapy. The values for forward exercising improved more than those for backward exercising. But the values for forward exercising were also much worse than those for backward exercising.
The severance of CNS functioning through the MS can also be seen well when comparing the trained MS CNS of the patient with the trained healthy case of the Author (Figure 19). Most likely, the high-load coordination dynamics will further improve with further CDT including the higher loads, that means the training at 100, 150 and 200N (Figure 19), unless of no further attack of the immune system. A recurrence of the MS would be possible to see in Figure 18 or 19, because with every injury/sclerosis the coordination dynamics values get higher (worse). Probably the CD measurements are more sensitive to injury and cheaper to perform than an MRI.
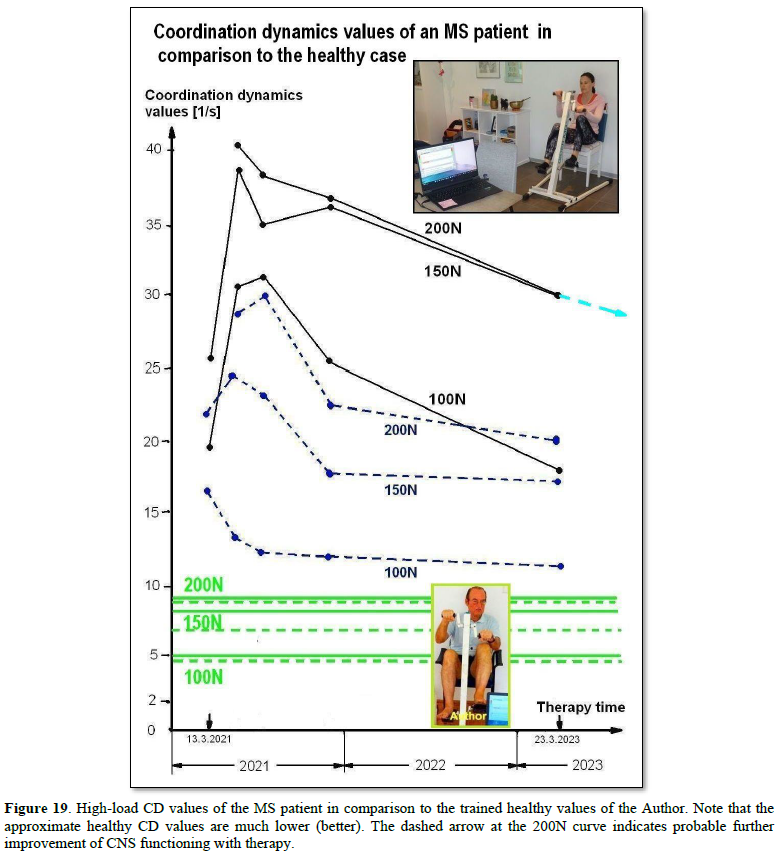
Most importantly, the patient had no further attack!
There are three possibilities for the arrest of the MS:
- The MS was cured, which is unlikely (see Discussion).
- The immune system was not attacking the CNS anymore because the treatment generated protective-friendly micro-repair environmental properties of the nerve cells in the neural networks (see Discussion).
- Accidently, the immune system did not attack the neural networks so far, which is unlikely.
Further treatment will show whether CDT can really stop or cure MS on the long-term.
DISCUSSION
Possible reason for the arrest of the MS
The coordinated movement-based learning therapy CDT for two years stimulated the coordination of pathways that regulate epigenetic mechanism through fine-tuning and coordination of gene expression, as DNA methylation, chromatin remodeling and small non-coding RNAs super families’, to generate in this way repair/protective-friendly, micro-environmental properties in the neural networks in the way that the immune system was not attacking the neural networks anymore.
Repair-comparison with spinal muscular atrophy
It was shown that CDT, administered for 8 months, could stop spinal muscular atrophy in a 43-year-old patient [28]. But when stopping CDT, the muscular atrophy started again in the way that the patient lost further muscle power. When the patient realized the situation, he started to train again.
It could therefore be that the multiple sclerosis patient would get further attacks from the immune system again when stopping CDT because of losing the repair and protective-friendly micro-environmental properties. The MS patient did not stop therapy and but intended to increase the intensity. Her motivation for more intensive training enhanced when seeing the improvement of her nervous system functioning in Figure 18.
Comparison of coordination dynamics value improvements of patients with multiple sclerosis and incomplete spinal cord injury
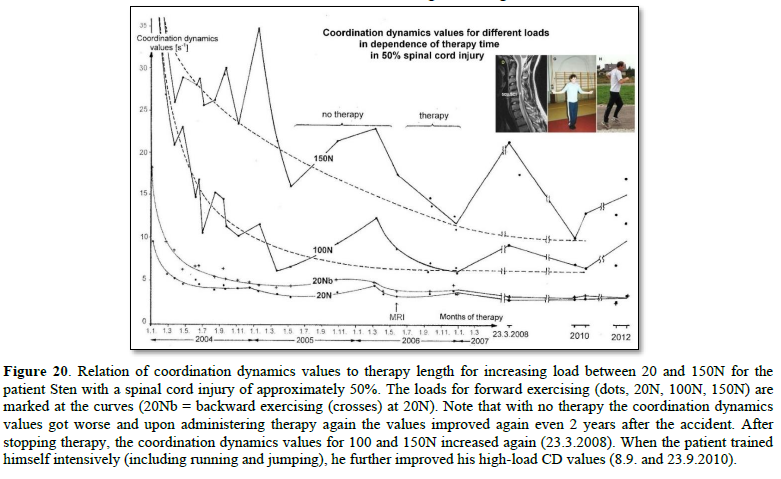
Figure 18 shows for the multiple sclerosis patient the therapy-induced improvement of the coordination dynamics values for increasing load. A patient with an incomplete spinal cord injury showed a similar improvement of the coordination dynamics values for different loads (Figure 20). For a more direct comparison of therapy-induced improvement of CNS functioning, the values for turning loads of 150 and 100N are displayed together in Figure 21.
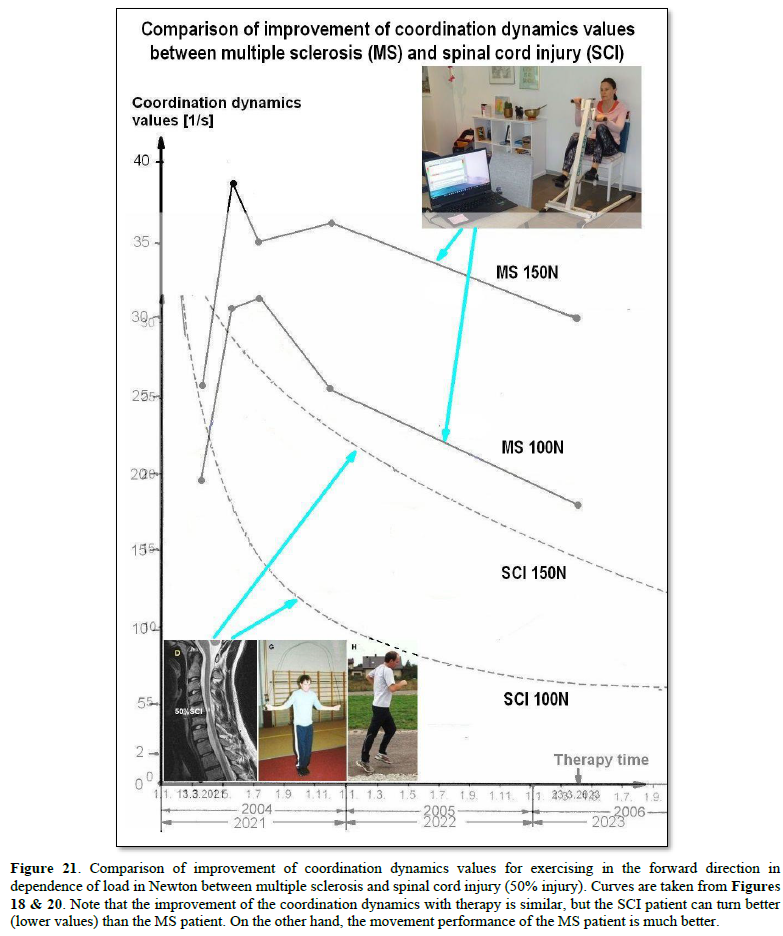
Even though the SCI patient could exercise more coordinated (lower values) than the MS patient (Figure 21), the movement performance of walking and running of the MS patient was still better. The multiple cerebro-spinal sclerosis seemed to have injured the general phase and frequency coordination of neural network organization more than the 50% spinal cord injury. Since the repair in spinal cord injury is mainly due to a neural network reorganization of supraspinal centers and not of a pyramidal or other tract fiber growing, MS and SCI are comparable with respect to neural network repair. It is the human brain with its natural intelligence (NI) which is the genius organ for repair, adaptation, and learning. Artificial intelligence (AI) is so far not able to repair its damaged artificial neural networks.
Importance of genetic disease repair
Many diseases are due to small genetic impairments. Also, MS could be due to a genome impairment. Human research is in progress to clarify to what extent genetic repair is possible [31]. It would change the world, if it would be possible to partly repair the human genome. The patient Anna with a severe cri-du-chat syndrome, is a suitable patient with her clear genetic disease to find out to what extent a genome repair is possible.
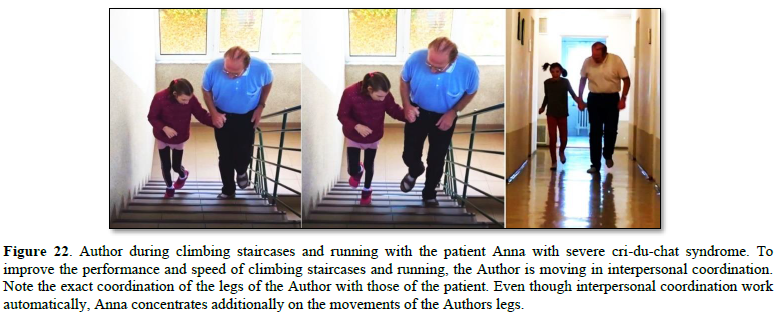
The 9.5-year-old patient Anna with severe cri-du-chat syndrome learned creeping, crawling, up righting, walking, running (Figure 1, I-N), jumping, and climbing staircases (Figure 22) through 4.1 months of rather optimal coordination dynamics therapy (CDT). The emotional pattern crying and laughing became operational. It is the first time that a real progress through therapy is published in this genetic disease. The lost piece of chromosome 5 included 5p15.1 through 5p15.33. Vojta, Bobath, and exercising on the “Locomat” did not improve Anna. Only low-intensity CDT at an age between 5.5 to 9.5 years made her walking a few steps. It cannot be excluded that with this optimal 4.1-months CDT at an age of 9.5 years, genetic plasticity started to take place and not only a repair of the malformed CNS caused by pathologic development due to the genetic disease.
The coordinated-movement-based learning therapy seemed to be capable of targeting the epigenome and altering gene expression and hence to repair the CNS in Anna, especially in the phase of super-coordination. The possibility of repair through gene expression changes is supported by CNS repair through CDT in traumatic brain injury, spinal cord injury, stroke, Parkinson, spina bifida, cerebral palsy, coma patients, bladder incontinence, basal ganglia injury, spinal muscular atrophy and cancer growth inhibition. Even though cognitive functions improved, Anna did not learn so far to speak, apart from the three words mama, tata and baba, and to read, write or calculate.
- Schalow G (2013) Human Neurophysiology: Development and Repair of the Human Central Nervous System. Nova Science Publishers, Inc, Hauppauge NY, USA, pp: 734.
- Schalow G (2015) Repair of the Human Brain and Spinal Cord. Nova Science Publishers, Inc, Hauppauge NY, USA, pp: 525.
- Schalow G (2015) Neural network learning in human. Nova Science Publishers, Inc, Hauppauge NY, USA, pp: 324.
- Schalow G (2002) Stroke recovery induced by coordination dynamic therapy and quantified by the coordination dynamic recording method. Electromyogr Clin Neurophysiol 42: 85-104.
- Schalow G (2002) Improvement after traumatic brain injury achieved by coordination dynamic therapy. Electromyogr Clin Neurophysiol 42: 195-203.
- Schalow G, Jaigma P (2006) Improvement in severe traumatic brain injury induced by coordination dynamics therapy in comparison to physiologic CNS development. Electromyogr Clin Neurophysiol 46: 195-209.
- Schalow G (2019) Regeneration of the human spinal cord via coordination dynamics therapy. Peertechz Publications, pp: 97.
- Schalow G (2009) Partial cure achieved in a patient with near-complete cervical spinal cord injury (95% injury) after 3 years of coordination dynamics therapy. Electromyogr Clin Neurophysiol 49: 199-221.
- Schalow G (2002) Recovery from spinal cord injury achieved by 3 months of coordination dynamic therapy. Electromyogr Clin Neurophysiol 42: 367-376.
- Schalow G (2003) Partial cure of spinal cord injury achieved by 6 to 13 months of coordination dynamic therapy. Electromyogr Clin Neurophysiol 43: 281-292.
- Schalow G, Jaigma P, Belle VK (2009) Near-total functional recovery achieved in partial spinal cord injury (50% injury) after 3 years of coordination dynamics therapy. Electromyogr Clin Neurophysiol 49: 67-91.
- Schalow G (2010) Cure of urinary bladder functions in severe (95%) motoric complete cervical spinal cord injury in human. Electromyogr Clin Neurophysiol 50: 155-179.
- Schalow G (2021) CNS Repair in a Girl with a Spinal Cord Injury. Adv Pub Health Com Trop Med 121: 201-226.
- Schalow G (2006) Cerebellar injury improvement achieved by coordination dynamics therapy. Electromyogr Clin Neurophysiol 46: 433-439.
- Schalow G (2021) Cure-like brain-repair in a girl with atrophied cerebellum and pons through Coordination Dynamics Therapy. Adv Pub Health Com Trop Med 123: 1-47.
- Schalow G, Jaigma P (2005) Cerebral palsy improvement achieved by coordination dynamics therapy. Electromyogr Clin Neurophysiol 45: 433-445.
- Schalow G (2006) Hypoxic brain injury improvement induced by coordination dynamics therapy in comparison to CNS development. Electromyogr Clin Neurophysiol 46: 171-183.
- Schalow G, Pääsuke M, Ereline J, Gapeyeva H (2004) Improvement in Parkinson’s disease patients achieved by coordination dynamics therapy. Electromyogr Clin Neurophysiol 44: 67-73.
- Schalow G, Nyffeler T (2001) Koordinationsdynamik-Therapie: Myelomeningozele (Spina bifida). Physiotherapie.
- Schalow G, Nyffeler T (2000) Koordinatiosdynamik-Therapie: Skoliose. Physiotherapy.
- Schalow G (2019) Permanent coma patient re-learned to speak via Coordination Dynamics Therapy. Arch Clin Med Case Rep 3(2): 33-50.
- Schalow G (2017) Breast cancer growth inhibition via Coordination Dynamics Therapy. In: “Horizons in Cancer Research. Editor: Hiroto S. Watanabe. Nova Science Publishers, Inc, Hauppauge NY, USA, Vol: 68; pp: 125-151.
- Schalow G (2020) Anaplastic oligodendroglioma WHO III brain cancer-patient recovered following operation, radiation and chemotherapy through Coordination Dynamics Therapy, which is also a Covid-19 treatment without ventilator. Int J Med Clin Imaging 5(2): 165-210.
- Christensen JF, Jones LW, Andersen JL, Daugaard G, Rorth M, et al. (2014) Muscle dysfunction in cancer patients. Ann Oncol 25: 947-958.
- Schalow G (2020) To live longer with a better quality of life through coordination dynamics therapy especially in patients with severe brain injury and brain-cancer. Int J Med Clin Imaging 5(2): 118-155.
- Schalow G (2021) Euthanasia in organ donation can be avoided through Coordination dynamics therapy. Adv Pub Health Com Trop Med 3: 1-34.
- Schalow G (2023) Basal ganglia and cortex repair through human-repair neurophysiology 12 years after hypoxia during birth. Adv Ortho Sports Med 02: 1-52.
- Schalow G (2022) Spinal muscular atrophy repair through Coordination dynamics therapy and Translation of frog neuromuscular innervation pattern changes caused by neurotrophins to human. Adv Ortho Sports Med 2022(2): 1-81.
- Schalow G (2022) Continence Repair Through Coordination Dynamics Therapy. Adv Pub Health Com Trop Med pp: 163.
- Schalow G (2023) Continence Repair through Neural Network Learning. Int J Med Clin Imaging 8(1): 433-476.
- Schalow G (2023) Genetic disease repair (5p-) through Coordination Dynamics Therapy. Int J Med Clin Imaging 9(1): 477-611.
- Colvis CM, Pollok JD, Goodman RH, Impey S, Dunn J, et al. (2005) Epigenetic mechanisms and gene networks in the nervous system. J Neurscience 25(45): 10379-10379.
- Compston A, Coles A (2008) Multiple sclerosis. Lancet 372(9648): 1502-1517.
- Milo R, Kahana E (2010) Multiple sclerosis: Geoepidemiology, genetics and the environment. Autoimmun Rev 9(5): A387-A394.
- Liu Z, Liao Q, Wen H, Zhang Y (2021) Disease modifying therapies in relapsing-remitting multiple sclerosis: A systematic review and network meta-analysis. Autoimmun Rev 20(6): 102826.
- Schalow G, Lang G (1987) Recording of Single Unit Potentials in Human Spinal Nerve Roots: A New Diagnostic Tool. Acta Neurochir 86: 25-29.
- Schalow G, Zäch GA, Warzock R (1995) Classification of human peripheral nerve fiber groups by conduction velocity and nerve fiber diameter is preserved following spinal cord lesion. J Auton Nerv Syst 52: 125-150.
- Schalow G (2009) The classification and identification of human somatic and parasympathetic nerve fibers including urinary bladder afferents is preserved following spinal cord injury. Electromyogr Clin Neurophysiol 49: 263-286.
- Schalow G (2020) Classification and Identification of Human Peripheral Nerve Fibers by Conduction Velocity, Nerve Fiber Diameter and Natural Firing Patterns with Consequences for CNS Repair and Covid-19 Infection Treatment. Int J Med Clin Imaging 5(3): 231-314.
- Schalow G (2005) Phase and frequency coordination between neuron firing as an integrative mechanism of human CNS self-organization. Electromyogr Clin Neurophysiol 45: 369-383.
- Schalow G (2021) Phase and frequency coordination improvement among neuron firing for improved CNS self-organization and neural repair in Parkinson and spinal cord injury. Int J Med Clin Imaging 6(1): 350-425.
- Schalow G (1993) Spinal oscillators in man under normal and pathologic conditions. Electromyogr Clin Neurophysiol 33: 409-426.
- Schalow G (2006) Surface EMG- and coordination dynamics measurements-assisted cerebellar diagnosis in a patient with cerebellar injury. Electromyogr Clin Neurophysiol 46: 371-384.
- Schalow G (2005) Tremor in Parkinson’s disease patients can be induced by uncontrolled activation and uninhibited synchronization of α2-motoneuron firing to which α1-motoneuron firing synchronizes. Electromyogr Clin Neurophysiol 45: 393-406.
- Kelso JAS (1995) Dynamic Patterns. The Self-Organization of Brain and Behavior. MIT Press, Cambridge.
- Schalow G (2010) Scientific basis for learning transfer from movements to urinary bladder functions for bladder repair in patients with spinal cord injury. Electromyogr Clin Neurophysiol 50: 339-395.
- Haken H, Kelso JA, Bunz H (1985) A theoretical model of phase transitions in human hand movements. Biol Cybern 39: 139-156.
- Deisseroth K, Singla S, Toda H, Monje M, Palmer TD, et al. (2004) Excitation-neurogenesis coupling in adult neural stem/progenitor cells. Neuron 42: 535-552.
- Eriksson PS, Perfilieva E, Björk-Eriksson T, Alborn AM, Nordborg C, et al. (1998) Neurogenesis in the adult human hippocampus. Nat Med 4: 1313-1317.
- Praag van H, Kempermann G, Gage H (1999) Running increases cell proliferation and neurogenesis in the adult mouse dentate gyrus. Nat Neurosci 2(3): 266-270.
- Schalow G (2009) Building of New Motoneurons in the Human Spinal Cord upon Coordination Dynamics Therapy to Improve Finger Functions in Motoric Complete Cervical Spinal Cord Injury. In: Berkovsky, T.C. (Ed.), Handbook of Spinal Cord Injuries, Chapter 4. Nova Science Publishers, pp: 231-264.




















QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- International Journal of Diabetes (ISSN: 2644-3031)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
")
")



