International Journal of Medical and Clinical Imaging (ISSN:2573-1084)

Case Report
Isolated Polycystic Pancreatic Disease: Endoscopic Ultrasound Image
32717
Views & Citations31717
Likes & Shares
Isolated Polycystic Pancreatic Disease is a rare disease. Asymptomatic cystic lesions is the most common presentation but sometimes it presents with mild vague abdominal pain. Diagnostic evaluation includes abdominal ultrasonography, contrast enhanced computed tomography and/or magnetic resonance imaging. There is scarcity of data on endoscopic ultrasound (EUS) features of isolated polycystic pancreatic disease. Here we are presenting EUS features in a patient of isolated polycystic pancreatic disease.
CASE
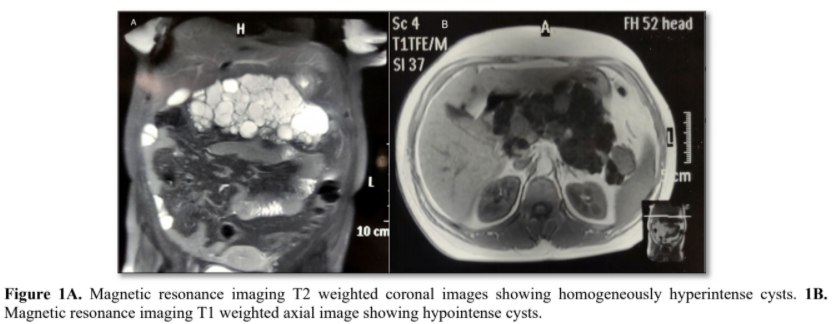
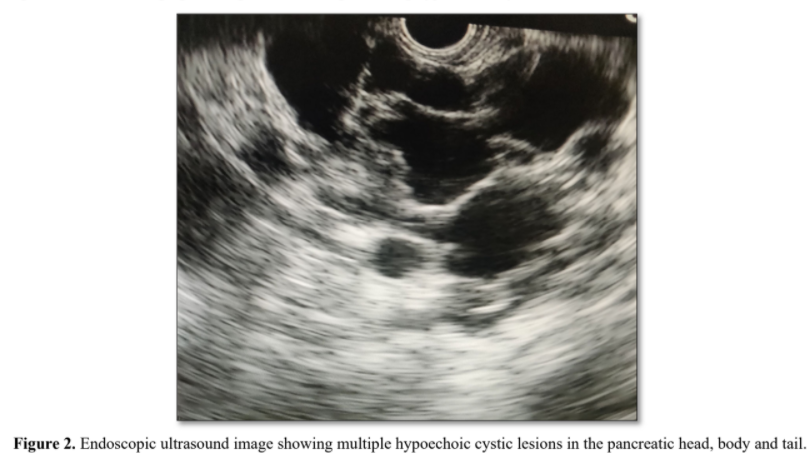
A 36-year-old female presented with mild epigastric pain since last 2 months. Her pain was dull aching, continuous and not radiating to back. There was no history of vomiting, anorexia and weight loss. Her general physical examination was within normal limits. Her laboratory parameters including hemogram, liver function test, renal function test, random blood sugar, serum amylase and lipase levels were also normal. Upper gastrointestinal endoscopy was normal. Abdominal ultrasound revealed multiple hypoechoic cysts diffusely involving the pancreas with no abnormality of other organs. She underwent abdominal magnetic resonance imaging (MRI), which showed multiple cysts of variable sizes occupying the pancreas and replacing the parenchyma. The cysts were homogeneously hyper intense on T2-weighted coronal images (Figure 1A) and hypointense on T1-weighted axial images (Figure 1B). There was no calcification, septations or haemorrhage within the cysts. Endoscopic ultrasound (EUS) showed multiple hypoechoic cystic lesions in the pancreatic head, body and tail, largest being 20x18 mm (Figure 2). Colour flow and doppler study confirmed the nonvascular nature of the cyst. There was no dilatation of the main pancreatic duct and no identifiable communication of the pancreatic duct with the cysts. EUS guided fluid aspirated from the largest lesion revealed normal amylase, CEA, CA19-9 and cytology was negative for malignancy. So, we diagnosed it as isolated polycystic pancreatic disease with no other system involvement. Differential diagnosis includes intraductal papillary mucinous neoplasms, mucinous cystic neoplasms, solid pseudo papillary neoplasms, and cystic pancreatic neuroendocrine tumours, whereas non-neoplastic lesions are pseudocysts, lymphoepithelial cysts, retention cysts, parasitic cysts and congenital-developments cysts. The patient was treated symptomatically with analgesics and supportive treatment. Six months later follow up EUS showed no progression in the cysts size and the patient remained asymptomatic.
DISCUSSION
Isolated polycystic pancreatic disease is a rare disease which is detected incidentally during abdominal imaging for other indications, surgery or autopsy. To date there are only a few cases reported, but none of the study reported EUS findings of isolated polycystic pancreatic disease [1-3]. Endoscopic ultrasound has emerged as an important tool in the diagnosis and risk stratification of pancreatic cystic lesions. Its potential to provides detailed imaging, tissue, cyst fluid for analysis makes it a useful tool for the diagnosis of pancreatic cystic lesions. Distinguishing between congenital and acquired cysts can be difficult. A detailed clinical history, radiological and histopathological features can facilitate this differentiation between congenital and acquired cyst. Symptomatic cysts, advanced age and rapidly increasing cyst size are the indications for surgery and can be managed with segmental pancreatectomy with cystectomy or de-roofing while asymptomatic polycystic pancreatic disease can be followed up with no therapeutic intervention.
CONCLUSIONS
Endoscopic ultrasound is useful in assessment and diagnostic workup of isolated polycystic pancreatic disease.
- Dhar DA, Suchi T, Garg S, Dixit VK (2012) A rare isolated polycystic pancreatic disease: Radiation free diagnostic protocol in selected cases. India J Endocrinol Metab 16 : 1054-1056.
- Jain VK, Jain J, Singh R, Gupta S (2016) Isolated polycystic disease of pancreas. Indian J Gastroenterol 35 : 250-251.
- Katsinelos P, Lazariki G, Anastasiadis S (2018) Isolated polycystic pancreatic disease: A very rare cause of pancreatic insufficiency. Clin Gastroenterol Hepatol 16 : e121.


QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Advance Research on Alzheimers and Parkinsons Disease
- Journal of Pathology and Toxicology Research
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Allergy Research (ISSN:2642-326X)
- Journal of Rheumatology Research (ISSN:2641-6999)
")
")



