
1635
Views & Citations635
Likes & Shares
Epidemiology: Dolichoarteriopathies are relatively common within the general population, with a prevalence ranging from 10% to 45% [6]. However, the reported incidence varies among the different studies [7]. Some studies suggest that kinking is the most frequent dolichoarteriopathy ranging from 5% to 25% [8] although recent research, points tortuosity as the predominant variant [9].
Anatomy and Embryology: The internal carotid arteries develop during embryogenesis on day 24, arising from the union of the third branchial arch and the distal segments of the dorsal aorta. They are the first arteries to develop and serve the critical function of supplying oxygen to the brain [10]. Adjacent to their origin, the ventral segment of the second branchial arch separates from the dorsal aorta and becomes the ventral pharyngeal artery. Later, both arteries fuse to form the common carotid artery, with the distal segment of the ventral pharyngeal artery persisting as the external carotid artery [11]. Disparities in these developmental stages may lead to anatomic variations [10]. In the cervical region, the arteries travel within the carotid sheaths, alongside the internal jugular vein and the vagus nerve, from which they receive innervation [1]. The extracranial portion extends from the bifurcation to its entry through the carotid canal at the base of the skull [1]. In the absence of dolichoarteriopathies, the ICA typically passes approximately 2.5 cm from the tonsils [12] a detail of surgical significance that must be reported, especially when anatomical variants are present.
Etiology: The pathophysiology and natural history of dolichoarteriopathies are not fully understood [8]. It is hypothesized that these anomalies result from an increased arterial length between fixed points at the bifurcation and the petrous bone, caused by a disproportionate growth of the muscular layer relative to the adventitia [2,13,14]. Additional theories attribute these changes to physiological aging processes, added to conditions such as atherosclerosis, vasculitis, or fibromuscular dysplasia, which cause loss of arterial elasticity, which ultimately leads to arterial elongation and tortuosity [6,15]. Some researchers suggest a multifactorial origin, where congenital kinking can change with age, diminishing with growth, and reappearing during aging [16].
Classification: A classification system, developed by Paulsen and collaborators, divides dolichoarteriopathies of the extracranial portion of the internal carotid artery into four types based on the degree of deviation from the vertical axis: straight (less than 15°), curved (15° to 70°), looped (70° to 145°), and coiled types (360° deviation) [2,17]. However, the most widely accepted classification of dolichoarteriopathies was established in 1965 by Weibel and Fields, and they are categorized into three types: tortuosity, coiling, and kinking [18]. Notably, multiple types can coexist within the same artery, and bilaterally has been well described [8] (Figure 1).
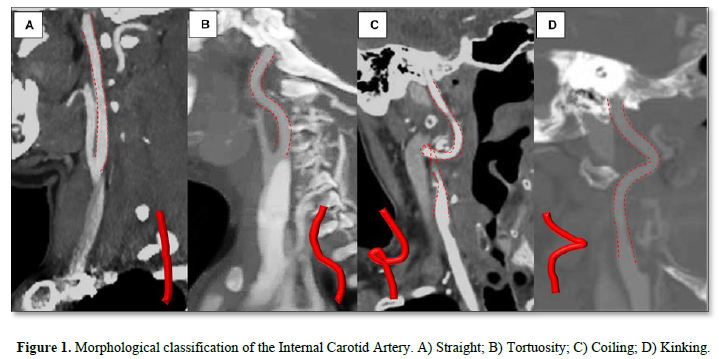
Tortuosity: Tortuosity refers to elongation and C- or S-shaped curvature [6]. It is further subdivided into elongation, redundancy, and undulation [2,8]. For some authors tortuosity may encompass other types of dolichoarteriopathies, such as coiling and kinking [2].
Coiling: Coiling is defined as elongation of the extracranial portion of the internal carotid artery within a confined space, resulting in an exaggerated "C," "U," or "S" shape or a simple or multiple circular configuration [8,18,19] due to a complete 360° rotation of the arterial tract [6].
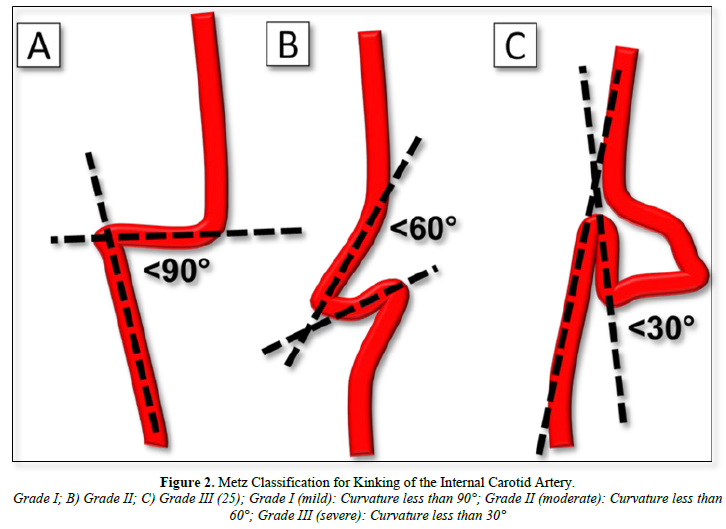
Kinking: Kinking is characterized by an acute angulation of the extracranial portion of the internal carotid artery of less than 90° [6]. Some authors believe kinking as a variation of coiling [8]. Kinking is further classified by the degree of curvature into three grades [8] (Figure 2).
CLINICAL IMPLICATIONS
Clinically, it may be asymptomatic or present as a pulsatile neck mass or pharyngeal bulge [8]. It may have a benign clinical course, or cause reduced cerebral blood flow, particularly in the presence of atheromatous plaques and stenosis [6,20]. Ischemia related to these anomalies is mainly attributed to two mechanisms. These include endothelial injury leading to thromboembolic events and hemodynamic alterations impairing cerebral perfusion [8]. Reported symptoms include pulsatile tinnitus of arterial origin, hemilingual spasm from hypoglossal nerve compression, cognitive decline in adults and children, neurodevelopmental delays, focal or generalized seizures, transient ischemic attacks (TIAs), ischemic strokes, hemiparesis and amaurosis fugax [6,8,21]. The degree of arterial bending correlates with the severity of cerebral hemodynamic impairment, and coiling has been shown to be less likely related to ischemic events than kinking [8]. Among the three types (tortuosity, coiling, and kinking), coiling and kinking are associated with greater hemodynamic abnormalities and reduced blood flow, with kinking carrying the most significant clinical implications [6]. Coiling can reduce the arterial lumen, causing turbulent flow and insufficient cerebral circulation.
 IMAGING EVALUATION
IMAGING EVALUATION
Imaging techniques are constantly evolving, and therefore, the study of these variants must adapt to advancements in technology. Modalities include neck ultrasound, digital subtraction angiography (DSA), CT angiography, and magnetic resonance imaging (MRI), particularly with Time-Of-Flight (TOF) sequences [8]. Reporting the presence of an anatomic variant is critical in a presurgical evaluation, as inadvertent ligation or injury during procedures such as tonsillectomy, adenoidectomy, or peritonsillar abscess drainage can lead to compromised perfusion or massive hemorrhage [8]. Postoperative follow-up can be performed using spectral Doppler ultrasound to evaluate dolichoarteriopathy repair [8].
Ultrasonography
Doppler ultrasonography has become increasingly significant in vascular evaluation due to its advantages as a non-invasive diagnostic technique. It provides both anatomical information and insights into blood flow dynamics, particularly in cases of suspected occlusion [8]. Additionally, it is especially valuable in the context of dolichoarteriopathies, allowing for the assessment of blood flow under varying neck positions. Grayscale imaging and Doppler techniques allow visualization of the arterial trajectories and calculate the Peak Systolic Velocity Kinking Ratio (PSVKR), which compares the peak systolic velocities at the kinking site and two centimeters proximal to the carotid bulb (Figure 3).
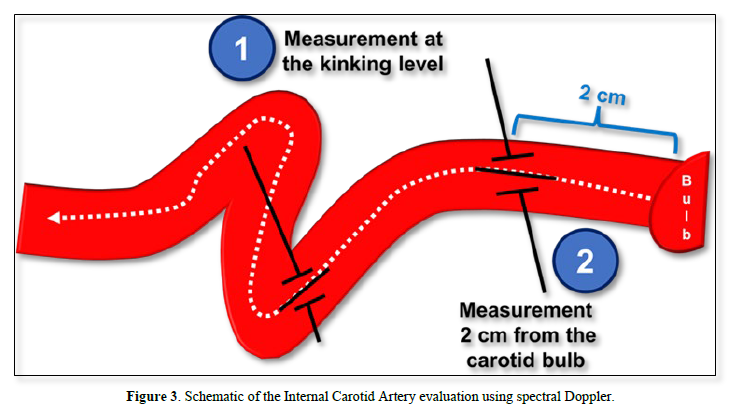
Peak Systolic Velocity is recorded at the kink or coil level and two centimeters proximal to the carotid bulb. The Kinking Ratio (PSVKR) is the ratio between both measurements. Based on Di Pino, 2020. This measurement correlates with the degree of angulation and the severity of obstruction of anatomic variants [6] offering functional insights into affected segments [6]. For instance, kinking severity has been linked to blood flow reductions: 40% in grade II and for grade III in 60% [8]. Additional factors influencing hemodynamic repercussions include intimal hyperplasia, atheromatous plaques, aneurysms, stenosis, and collateral cerebral circulation [8]. Ultrasound is advantageous for dynamic assessments accounting for physiological states such as hypotension during sleep, head hyperextension, and head rotation, which can affect flow dynamics. Also, it is particularly valuable for postoperative evaluation of internal carotid artery (ICA) surgery, aiding in assessment of vessel alignment and flow restoration. Despite its benefits, Doppler ultrasonography has limitations. It is operator-dependent, it requires a steep learning curve, and implies technical challenges that may arise in patients with small necks or certain body compositions [8].
CT angiography
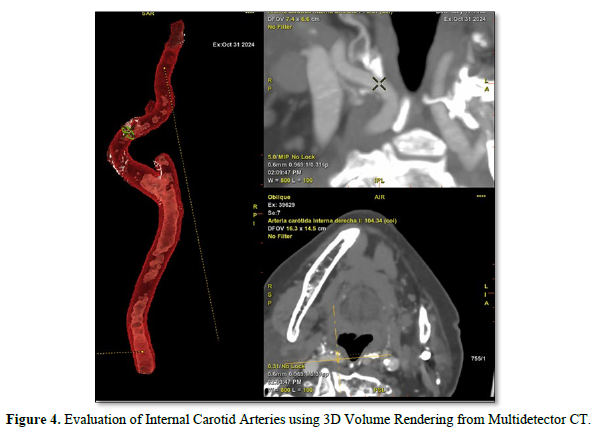
CT angiography with contrast or MRI provides superior anatomical detail and is unaffected by ultrasound limitations [6,9]. CT is particularly useful for evaluating arterial trajectories and detecting alterations such as microaneurysms [8,20]. It enables a comprehensive assessment of supra-aortic trunks and branches, vessel calibers, and atheromatous plaques, aiding in preoperative planning [21]. Sagittal or coronal CT and MRI slices allow measurements based on Metz’s classification and enable three-dimensional reconstructions for a more accurate assessment of tortuosity types [8] (Figure 4).
One recommended protocol, consists in a simple scan that must be obtained from the aortic arch to the cranium vertex, followed by a contrast enhanced phase. 50 to 70 ml of non-ionic intravenous contrast is injected with a flow of 6 ml/s [22]. Measurement of kinking angle is determined by drawing two lines, one along the axis of the internal and common carotid arteries and another along the axis of the cervical segment of the internal carotid artery [8], however, another proposed measurement is drawing one line along the axis of the proximal portion of the vessel and other in the distal portion (Figure 5).
The kinking angle is measured by drawing two lines: one along the axis of the cephalic portion of the kink and another along the caudal portion, following the typical direction of blood flow.

Magnetic resonance imaging
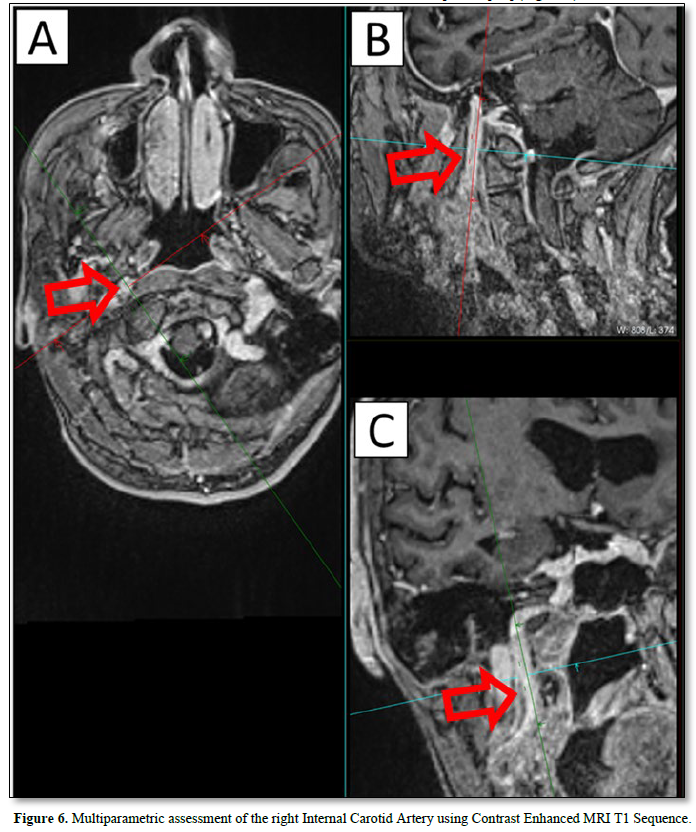
Magnetic resonance imaging (MRI) is particularly indicated in dolichoarteriopathies when there is an impairment of blood flow, as MR perfusion studies can provide valuable insights [8]. This non- invasive method offers multiple sequences to evaluate both the vessel pathway and its hemodynamic implications. Contrast-enhanced MRI is considered more effective for diagnosing dolichoarteriopathies [3,8] (Figure 6).
Alternatively, non-contrast Angio-MRI using Time-of-Flight (TOF) sequences is a viable option (Figure 7).

Digital subtraction angiography
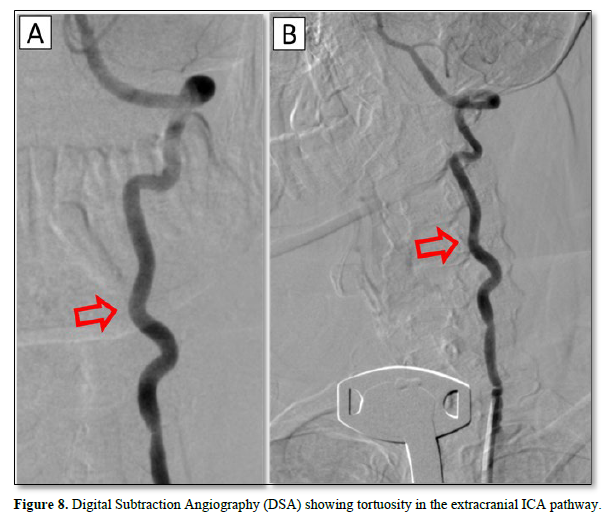
Digital subtraction Angiography (DSA) is a fluoroscopic technique for the visualization of blood vessels. It provides detailed arterial morphology, useful distinguishing morphologic subtypes [3] particularly through 3D reconstructions, and also has the advantage of providing real-time hemodynamic data concerning brain flow. Also, postprocessing, such as in the PACS system, can provide valuable tools for the measurement of dolichoarteriopathies [23]. However, it does not evaluate the arterial wall, unlike CT and MRI [8].
Nuclear imaging
Nuclear imaging with intravenous technetium-99m (99mTc) pertechnetate can provide perfusion data in symptomatic patients, this is useful, especially in the context of kinking for its association with blood flow reduction [8] (Figure 8).
MANAGEMENT AND PROGNOSIS
Surgical intervention may be considered in cases where significant hemodynamic impairment is documented, although the optimal treatment remains controversial [8]. Procedures include resection of redundant segments with vascular reconstruction [24] end-to-end anastomosis to a lower internal carotid segment or at the bifurcation, end-to-side anastomosis with the external or common carotid artery, endarterectomy with patching or imbrication of the common carotid artery, bypass grafting or eversion endarterectomy with excision of excess arterial length. The aim is to shorten the vascular trajectory, restore perfusion, and prevent recurrence [8,25]. For cerebrovascular insufficiency caused by kinking, surgical intervention can prevent further deterioration of perfusion. In cases of tortuosity, surgery is recommended only when atherosclerosis causes stenosis [8,26-30]. Post-surgical outcomes are generally favorable, with low morbidity and mortality rates. Follow-up studies have shown no recurrences over six years [8] and cognitive function and symptoms, such as ocular disturbances, often improve significantly after treatment [8].
CONCLUSION
Vascular anomalies of the extracranial internal carotid artery have elicited attention due to their potential association with brain hypoxemia, and the increased surgical procedures they pose. As imaging techniques continue to evolve, the study of these variants must adapt to advancements. Accurate detection and routine reporting in imaging are crucial for improving patient care, facilitating surgical planning, preventing complications, and enhancing knowledge in these entities. This article provides a comprehensive review of the current state of imaging techniques used to evaluate dolichoarteriopathies and serves as a foundation for further studies.
- Charlick M, Das J (2023) National Library of Medicine. Available onilne at: www.ncbi.njm.nih.gov/books/NBK556061
- Rocha-Remón P, Fonseca-Pisch AJ (2019) Dolicoarteriopatías de la carótida interna cervical. An Orl Mex pp: 96-101.
- Lomini PA, Beigelman R, Ambrosio G, Izaguirre A, Milei J (2024) Dolicoarteriopatías carotídeas: un enfoque global. Revista Argentina de Cardiología 92(3): 10-20.
- Beigelman R, Izaguirre A, Milei J (2009) Are Kinking and Coiling of Carotid Artery Congenital or Acquired? Angiology 61(1): 107-112.
- Kelly A (1925) Tortuosity of the internal carotid in relation to the pharynx. J Laring pp: 251-260.
- Di Pino L, Franchina A, Costa S, Gangi S, Strano F, et al. (2021) Prevalence and morphological changes of carotid kinking and coiling in growth: an echo-color Doppler study of 2856 subjects between aged 0 to 96 years. Int J Cardiovasc Imaging 37: 479-484.
- Pellegrino L, Prencipe G, Vairo F (1998) Dolicoarteriopatie (kinking, coiling, tortuosità) delle arterie carotidi: studio con esame eco color Doppler [Dolicho-arteriopathies (kinking, coiling, tortuoosity) of the carotid arteries: study by color Doppler ultrasonography]. Minerva Cardioangiol 46(3): 69-76.
- Yu J (2027) Current Understanding of Dolichoarteriopathies of the Internal Carotid Artery: A Review. Int J Med Sci 14(8): 772-784.
- Barfzadeh A, Saba M, Pourzand P (2024) Anatomical variations of the extracranial internal carotid artery: Prevalence , risk factors, and imaging insights from CT-angiography. Surg Radiol Anat 46: 1295-1299.
- Menshawi K (2015) A Functional Perspective on the Embryology and Anatomy of the Cerebral Blood Supply. J Stroke 17(2): 144-158.
- Kathuria S, Gregg L, Chen J, Gandhi D (2011) Normal cerebral arterial development and variations. Semin Ultrasound CT MR 32(3): 242-251.
- Alsini YA, Alsheikhi I (2017) Pulsating Tonsil due to Medial Displacement of the Internal Carotid Artery. Am J Case Rep 18: 502-506.
- Pfeiffer J, Ridder G (2008) A clinical classification system for aberrant internal carotid arteries. Laryngoscope 118(11): 1931-1936.
- Vannix R, Joergenson E, Carter R (1997) Kinking of the internal carotid artery. Clinical significance and surgical management. Am J Surg 134(1): 82-89.
- Radak D, Babic S, Tanaskovic S, Matic P, Sotirovic V, et al. (2012) Are the carotid kinking and coiling understimated entities? Vojnosanit Pregl 69(7): 616-619.
- Benes V, Mohapl M (2021) Alternative surgery for the kinked internal carotid artery. Acta Neurochir 143(12): 267-1272.
- Paulsen F, Tillmann B, Christofides C, Richter W, Koebke J (2000) Curving and looping of the internal carotid artery in relation to the pharynx: frequency, embriology and clinical implications. J Anat 197(3): 373-381.
- Weibel J, Fields W (1965) Tortuosity, coliling and kinking of the internal carotdis artery. Etiology and radiographic anatomy. Neurology 15: 7-18.
- Quijano Y, García D (2020) Variantes Anatómicas Del Círculo Arterial Cerebral En Un Anfiteatro Universitario en Bogotá (Colombia). Revista Ciencias de La Salud 18: 01-08.
- Mamedov F, Arutiunov N, Usachev D, Lukshin D, Beliaev A (2011) Neuroradiological diagnostics of atherosclerotic lesions and kinking of rhe carotid arteries in determination of indications to surgical treatment. Zh Vopr Nirokhiir IM N Burdenko 75(2): 3-10.
- Baz R, Apostol E, Niscoveanu C, Bordei P (2021) Course variations of the cervical internal carotid artery. Revista Română de Anatomie funcţională şi clinică, macro- şi microscopică şi de Antropologie 20(4): 265-269.
- Van Rooij J (2020) Coiling of the Internal Carotid Artery is Associated with Hypertension in Patients Suspected of Stroke. Clin Neuroradiol 31: 425-430.
- Wang HF (2017) Extracranial Internal Carotid Artery Tortuosity and Body Mass Index. Front Neurol 8(508): 01-09.
- Ramírez-Pérez E (2020) Reconstrucción Quirúrgica de Dolicoartiopatía Sintomática En La Arteria Carótida Interna Y Predictores de Correción Hemodinámica. Rev Mex Angiol 48(1): 01-10.
- Illuminati G, Calio F, Papaspyropoulos V, Montesano G (2003) Revascularization of the interna carotid artery kinking- case report. Arch Surg 138(2): 192-197.
- Ilic M, Tanaskovic S, Ilijevski N, Radak D (2011) Acute reversible ischaemic neurological deficit induced by internal carotid artery kinking-case report. Srp Arh Celok Lek 139(1-2): 92-94.
- Gavrilenko A, Kuklin A, Khripkov A, Abramian A (2014) Assessment of efficacy of reconstructive operations on carotid arteries in combination of stenosis and pathological tortuosity. Angiol Sosud Khir 20: 116-122.
- Metz H, Murray L, Bannister R, Bull J, Marshall J (1961) Kinking of the internal carotid artery. Lancet 1(7174): 424-426.
- Beigelman R, Izaguirre A, Azzato F, Milei J (2014) Carotid Artery-Patholoy, Plaque Structure - Relationship between Histological Asssessment, Color Doppler Ultrasonography and Magnetic Resonance Imaging - Dolichoarteriopathies - Barorreceptors. Intech Open 14: 31-83.
- Takkar A, Khurana D, Khandelwal N (2016) Kinked carotids: The "python" in neck. Ann Indian Acad Neurol 19(3): 409-410.








QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Advance Research on Alzheimers and Parkinsons Disease
- Chemotherapy Research Journal (ISSN:2642-0236)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)


