Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)

Case Report
Complex Case Report-Learning Disabilities and Incidental Discovery of Dandy-Walker Syndrome, DiGeorge Syndrome Phenotype and Premature Thelarche
4683
Views & Citations3683
Likes & Shares
Dandy-Walker syndrome is a rare cerebral posterior fossa malformation that could manifest with learning disabilities, intellectual disability, developmental delay. DiGeorge syndrome is associated with dysmorphic features, low IQ scores, learning disabilities, language delay. Premature thelarche occurs in girls prior to age of 8 years, it could be linked to central nervous system abnormalities. We report a case of a 7-year-old-girl who has presented with cognitive symptoms and further investigation revealed Dandy-Walker syndrome, DiGeorge syndrome and premature thelarche. The following case presentation illustrates an extremely rare association and has never been described in literature.
Keywords: Dandy-Walker syndrome, DiGeorge syndrome, Premature thelarche Learning disabilities, Development delay
INTRODUCTION
Learning disabilities are problems in school related tasks, for instance writing (dysgraphia), reading (reading comprehension, dyslexia), calculus (dyscalculia). These were discriminated from behavior disorders and intellectual disabilities, but could overlap with attention difficulties and language and cognitive disorders due to developmental delay. Neurological and genetic determinants are recently better studied [1]. Dandy-Walker syndrome (DWS) is a rare cerebral malformation involving posterior fossa mainly portrayed by vermis hypoplasia and dilatation of fourth ventricle and cerebellomedullary cistern, but multiple variants could occur. It is associated with hydrocephalus and abnormal corpus callosum. Other systems could be affected, such as heart or urogenital malformations, toes and fingers-polydactyly or syndactyly and face particularities. Usually diagnosed in the first year of life, children present macrocephaly due to fluid accumulation, delayed motor development-coordination, walking, crawling, intellectual disability, learning difficulties in those with normal intelligence, mental and behavior problems, rare seizures. DWS was associated with genetic defects, most common 13, 18 and 21 trisomy and triploid [2-4]. DiGeorge syndrome is a 22q11 chromosome deletion that may produce congenital heart defect, thymus underdevelopment, otolaryngeal anomalies and cleft palate, genitourinary anomalies, endocrine dysfunction (hypocalcemia, hypothyroidism and hyperthyroidism). Phenotype is represented by long face, small eye openings, ptosis, small head, high and wide nose bridge and dimple on nose, asymmetrical crying face, low insertion and round ears, cleft palate. Clinical features include growth retardation, decreased IQ scores with speech delay-until 3 years of age the child uses few phrases and sentences, mild and moderate learning disabilities [5,6]. Premature thelarche is breast enlargement before the age of 8. It could manifest following premature activation of hypothalamus-pituitary-gonadal (HPG) axis, thus dependent to gonadotropin-releasing hormone (GnRH). Although most cases are idiopathic, a small degree could be caused by central nervous system anomaly, furthermore magnetic resonance imaging is recommended in girls under 6 years and in rapid evolution of puberty or neurological disorders [6].
CASE PRESENTATION
We report the case of 7-year, 6-month-old girl admitted to Pediatric Psychiatry ward for learning difficulties, mild attention difficulties and slight developmental delay. She could not understand certain words and concepts, the language and thinking process were assessed at being below the corresponding level for her chronological age.
Family medical history
Both parents aged 34 (mother) and 37 years old (father) were healthy, without any significant family medical history. At the time of admission, the mother was seven-and-a half months into pregnancy with second child.
Physiological personal history
The patient is the first child, from pregnancy with physiological evolution, vaginal birth at 38 weeks, cephalic presentation, Apgar Score 9, birth weight: 2910 g, cranial perimeter: 32 cm and appropriate postnatal adaptation. It was observed a delayed psychomotor development thus the patient sat upright at 7-8 months, she walked independently at the age of 1 year and 4 months, she first babbled at 10 months and until 2 years old she spoke few words.
Life conditions
The patient lived with her parents and maternal grandparents and at the time of admission was a first-grade student with school results below average.
Pathological personal history
At 4 months the patient was examined neurologically because she presented microcephaly without any improvement, but the tests did not conclude any particularities.
At 2 years old she was diagnosed with expressive language disorder and described as using combined types of nonverbal communication; neurotrophic treatment and speech therapy were recommended with good results.
1 year before admission optical correction for hyperopia was prescribed.
Mental examination
Mental evaluation revealed further details about the language: receptive language apparently less developed compared to expressive speech, certain words and directions needed to be repeated multiple times before the patient understood. The vocabulary was limited and inadequate for her chronological age, she used mostly simple sentences and presented bradylalia and mild dyslexia. Cognitive assessment showed increased latency of response to the tasks given-bradypsychia, the patient could not mention the seasons, she said week has 5 days and had difficulties of making the rhombus according to the model. Hyperkinetic behavior and spontaneous and voluntary hyperpiesia were also noticed during admission.
Psychological assessment
Intelligence quotient was scored at 66 suggesting mild intellectual disability.
Physical examination and clinical investigations
Patient presented truncal adiposity and breast enlargement.
Laboratory tests revealed hypercholesterolemia (total cholesterol: 237 mg/ml, LDL cholesterol: 140 mg/dl), increased levels of ESR: 16 mm/1 h, GOT: 34 U/l, serum calcium: 11 mg/dl and T3: 1.74 ng/ml. Electrocardiogram (ECG) depicted sinus respiratory arrhythmia. Electroencephalography (EEG) in wakefulness displayed single generalized spike-wave discharge on the graph, patient was referred to Pediatric Neurology.
Neurological examination
Patient presented appearance particularities, such as asthenic constitutional type, prominent metopic ridge, high-arched palate, signs of precocious puberty. The girl walked independently, unipedal stance test performed with difficulty right>left lower limb, motor disability, increased deep tendon reflexes lower limbs>upper limbs, normal coordination tests. Further investigations were recommended: awake EEG test to be repeated, sleep-deprived and intermittent photic stimulation (IPS) EEG test and cerebral MRI; also, the patient was referred to Endocrinology and Genetics. Awake, IPS and sleep EEG line provided a normal background rhythm for the age, lack of epileptiform patterns to support school difficulties.
Imaging results
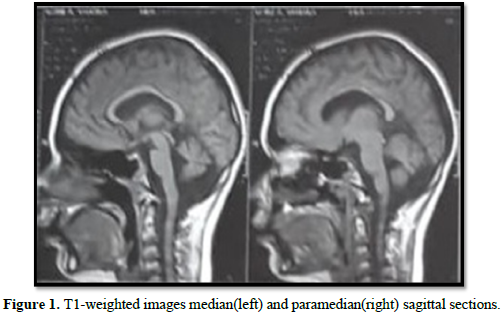
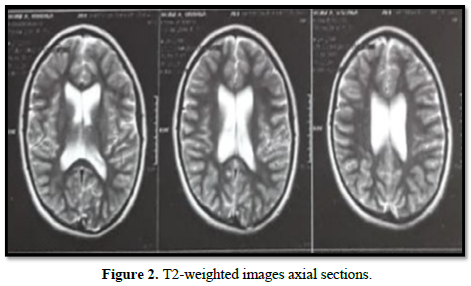
Cerebral MRI indicated Dandy-Walker syndrome aspect with mega cisterna magna, communication through median aperture in the lower roof with a slightly enlarged fourth ventricle, tectal plate mildly ascended, widening of cerebellar fissures (Figure 1). Median structures in normal position with modest thinning of corpus callosum and moderate triventricular hydrocephalus, without discernible cerebrospinal fluid (CSF) flow abnormalities were also detected (Figures 1 & 2).
Endocrinology examination
Premature thelarche was recommended to be further investigated: measurement of hormones LH, FSH, estradiol levels before and after GnRH analog administration, pelvic ultrasound imaging and hand-wrist radiograph for bone age study. Results were ongoing at the time of hospital discharge.
Genetic examination
Growth parameters were evaluated H=140 cm 97th percentile, G=28.5 kg 75th percentile and head circumference=48 cm <3rd percentile. Dysmorphology assessment showed the following abnormal areas: face-general impression: subtle dysmorphic features, head-microcephaly; eyes-bilateral partial blepharoptosis; mouth-held open, dental malocclusion, high-arched palate; jaw-micrognathia; lower limbs-bilateral partial syndactyly 2/3 toes; nervous system-fine motor disability; speech-bradylalia, dyslalia, hypernasal voice. Genetic testing was recommended for in observation DiGeorge syndrome.
Therapeutic recommendations
At the time of discharge, patient was under neurological supervision, she had not needed a neurosurgical intervention for ventriculoperitoneal or cyst peritoneal shunt in order to drain the hydrocephalus. Mental health recommendations included appropriate school curriculum and support teacher, suitable cognitive stimulation for child’s developmental level and adequate psychoeducational intervention for child’s emotional needs.
DISCUSSION
The complexity of this case resides in its heterogeneity and multiple common and distinct features intertwined and conducting final diagnosis. Learning difficulties, development delay and intellectual disabilities are associated with Dandy-Walker syndrome and also with DiGeorge syndrome [2-5]. Fine motor disability, syndactyly and awake EEG discharge indicating risk of seizures are components of Dandy-Walker malformation clinical manifestation [3,4]. Advanced age of diagnosis is notable and it may be due to lack of severe symptoms related to hydrocephalus, coordination, posture and balance problems, speech problems presented by our patient could be associated with cerebellum impairment [5,7,8]. Endocrine dysfunctions met in DiGeorge syndrome are discussed, hypocalcemia found in 30-60% of cases [5] was not detected in our patient, moreover high levels of calcium were determined. Hyperthyroidism, although less common than hypothyroidism [5], was indicated by increased levels of T3. Attention difficulties could be associated with DiGeorge syndrome [9]. Phenotype patient particularity is hyper nasal voice revealing velopharyngeal incompetence, a submucosal type of cleft palate, more frequent than overt cleft palate, which could delay diagnosis [6]. Causes of hypercholesterolemia remain unclear. Unspecified inflammatory marker (ESR) could be related to DiGeorge syndrome susceptibility to infections [5]. Truncal adiposity could be a sign of precocious puberty [10]. Hydrocephalus could be a possible etiology of precocious puberty [11].
CONCLUSION
Relevance of reported case consists in detection of two rare diseases, DiGeorge syndrome and Dandy-Walker malformation, starting from relatively benign and unspecific symptoms such as learning disabilities, mild attention difficulties and slight developmental delay. These could lead to neurological and genetic implications with permanent impact in prognostic, evolution and quality of life. Hence multidisciplinary teams have a crucial role for proper approach and complex treatment of rare diseases, in particular. We intend to contribute with future follow-up paper of presented case as relevant diagnostic data was not available at the time.
- Fletcher JM, Grigorenko EL (2017) Neuropsychology of Learning Disabilities: The Past and the Future. J Int Neuropsychol Soc 23(9-10): 930-940.
- Zamora EA, Ahmad T (2021) Dandy Walker Malformation. Available online at: https://www.ncbi.nlm.nih.gov/books/NBK538197/
- Dandy-Walker malformation (2020) Available online at: https://medlineplus.gov/genetics/condition/dandy-walker-malformation/
- Alanis GT, Gonzalez NC, Josel VMC, Juan BGF, Hector RMM, et al. (2014) Dandy Walker malformation. Arch Argent Pediatr 112(1): 103-105.
- Firth H, Hurst J (2017) Clinical Genetics and Genomics. Second edition. Oxford: Oxford University Press. Available online at: https://oxfordmedicine.com/view/10.1093/med/9780199557509.001.0001/med-9780199557509
- Bawle E (2018) DiGeorge Syndrome Clinical Presentation. Available online at: https://emedicine.medscape.com/article/886526-clinical/
- Varimo T, Heta H, Paivi JM, Laura K, Johanna H, et al. (2017) Precocious Puberty or Premature Thelarche: Analysis of a Large Patient Series in a Single Tertiary Center with Special Emphasis on 6- to 8-Year-Old Girls. Front Endocrinol (Lausanne) 8: 213.
- Marien P, Herman A, Michael A, Caroline HSB, Alan B, et al. (2014) Consensus paper: Language and the cerebellum: an ongoing enigma. Cerebellum 13(3): 386-410.
- Hacihamdioglu B, Merih B, Zeynep S, Figen D, Pelin B, et al. (2011) Case Report: Two Patients with Partial DiGeorge Syndrome Presenting with Attention Disorder and Learning Difficulties. J Clin Res Ped Endo 3(2): 95-97.
- Hillman J, Biro F (2010) Dynamic Changes of Adiposity During Puberty: Life May Not Be Linear. J Adolesc Health 47(4): 322-323.
- Rajput R (2018) Dandy-Walker variant with precocious puberty: A rare association. BMJ Case Rep 11(1): e226281.


QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Chemotherapy Research Journal (ISSN:2642-0236)
- International Journal of Diabetes (ISSN: 2644-3031)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Pathology and Toxicology Research
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)


