Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)

Research Article
Predictor Factors of Gap Speed in the Elderly of the Community
3977
Views & Citations2977
Likes & Shares
Introduction: The elderly population is usually accompanied by a natural decline in organic systems, chronic-degenerative conditions and greater functional disability. All of this can be caused by or can cause loss of muscle mass and strength, decreased balance, proprioception and mobility, resulting in dependence, falls, hospitalizations, institutionalizations and death. Gait can be compromised by an isolated factor or several factors that add up, and can influence gait speed deficiencies such as: balance, osteoarthrosis, osteoporosis, sarcopenia and weakness. It can also be influenced by personal factors such as: body mass index and level of physical activity.
Objective: To evaluate the predictors of gait speed in elderly living in community.
Method: Cross-sectional study, carried out with 91 elderlies with independent gait, residents of the community, who were assessed through BMI, balance test, gait speedtest, chair support test - through the Short Physical Performance Battery (SPPB).
Results: The variables “practice of physical activity” and “strength of lower limbs” showed correlation and were included in the regression analysis, as potential predictors of gait speed. Static balance and BMI showed no correlation with walking speed.
Conclusion: The present study pointed out lower limb strength and physical activity showed correlation with gait speed in active elderly in the Community.
Keywords: Balance. Elderly. Gait speed. IMC. Lower limb strength. Physical activity
INTRODUCTION
Population aging is an irreversible and universal phenomenon, to which countries try to adapt [1]. In Brazil, according to data from the Brazilian Institute of Geography and Statistics, the number of elderly people in 2017 surpassed the mark of 30.2 million, with women representing 56%. In addition to this significant increase, this emerging population is accompanied by a natural decline of organic systems, several chronic-degenerative conditions and greater functional disability [2,3]. Causing loss of muscle mass and strength, decreased muscle balance, proprioception and mobility, resulting in increased dependence, falls, hospitalizations or institutionalization and even death [3]. In general, functional disability in individuals over 65 years of age is described as a social problem, however it can also be conceptualized as a health problem due to the consequences it generates [4]. leading to difficulty in performing activities of daily living (AVD) such as transference, gait, bathing, dressing, among others [5] and promoting gait changes. Gait is a complex motor skill, consisting of a sequence of alternate movements of the lower limbs that generate body movement being an important factor in maintaining independence in basic daily activities [6]. However, this task can change with senescence, as various organs and systems of the body responsible for motor control are affected, gait disturbances can lead the elderly to be more prone to the aforementioned factors, such as loss of strength and balance, impairment of ability to walk and falls [7-10]. According to epidemiological evidence it is reported that a decline in the level of physical activity with increasing chronological age, making sedentary lifestyle a risk factor for morbidity and mortality during the senescence process [11,12]. The practice of regular physical activity influences the maintenance of normal bone activities [13] and has been beneficially associated with the preservation of functionality, reducing the effects caused by aging [6]. Elderly people with Body Mass Index (BMI) above 30 kg/m2 (obesity) are 60% more likely to suffer a decrease in physical capacity when compared to their eutrophic peers [14,15]. In addition to strength, in performing most daily activities, balance is needed, which is characterized by the maintenance of the force center within the base of support; when there is displacement of the force center and the body is not able to correct it in a timely manner, there is postural instability [16-18]. Body imbalance can cause changes in gait pattern, such as reduced speed and step length, increasing the risk of falls [19]. Several studies have shown a relationship between low gait speed (MV) and loss of functionality [20-24]. According to Perera [25] the evaluation of MV is considered by gerontologists an important indicator of the functionality of the elderly due to its ability to point out adverse events such as functional limitations, frailty, loss of independence, hospitalizations, traumas, fractures, psychological disorders and death. According to Ferrucci [26] adequate interventions can improve the difficulty of walking and delay the pathophysiological process that led to physical disability. There are studies in the literature correlating gait speed in the elderly [27-32] however, there is no study with all the aforementioned predictors that influence the gait speed of the elderly, including not only disability measures such as balance, lower limb strength, but also personal factors such as BMI and level of physical activity. The acquisition of such data would provide evidence about possible risks of declining functional capacity, making it possible to design preventive approaches and intervention programs with more precision, aiming at improving quality of life, reducing functional dependence and even death. Thus, the aim of this study was to evaluate the predictors (BMI, lower limb strength, balance and physical activity) of gait speed in the elderly.
METHODS
Study design
This is an observational, cross-sectional study, approved by the Research Ethics Committee of FUNCESI on June 14, 2019, number 13923919.6.0000.5110. 2.2 Sample The present study was carried out with elderly people living in the city of Itabira in Minas Gerais, who sought the Physiotherapy service through the Rehabilitation Center. Men and women aged 60 years or over, residents of the community and those who walked independently were included. Exclusion criteria were: elderly affected by disabling musculoskeletal conditions; presence of any type of bleeding; amputees and with motor, visual or auditory sequelae that make it impossible to carry out the tests. Participants were previously instructed by telephone.
Data Collection
Data collection for this research was in two parts:
- through the database from Magalhães [33] - 65 elderly people accessed in 2019;
- with 26 elderly people accessed at the physiotherapy clinic in 2020. Two blinded researchers (A and B) collected the study information. After signing the Informed Consent Form, the participants were submitted to personal and anthropometric information collection, in addition to clinical measurements (APPENDIXES A and B), to investigate the possible predictors of gait speed: BMI, lower limb strength, balance and physical activity. Data from the same outcomes and the same test collected.
Procedures
After signing the consent form and initial data collection, the possible predictors of gait speed were evaluated by the examiners. The initial interview collected data such as BMI and physical activity. Lower limb strength, balance and gait speed were assessed using the Short Physical Performance Battery (SPPB) test. For the balance test, participants were instructed to remain standing in three positions with progressive reduction of the support base, for 10 seconds in each position, side-by-side, semi-tandem stand, tandem stand, respectively. In the gait speed test, the elderly was instructed to walk at a usual pace, at a distance of three meters. To assess the strength of the lower limbs (LL) using the chair support test, the participants were instructed to sit and stand up five consecutive times, without the aid of the upper limbs (arms flexed in front of the chest) [34]. To obtain the SPPB score, the values of the balance test, gait speed and the chair support test were used. The test is given a differentiated score from zero to four, according to the time of each task, if it is impossible to perform any of them, the score is zero. The score, therefore, ranges from zero to 12, determining as dependent / worst performance or good performance, respectively [34]. For the timing of the tests, the digital Chronobiomodel SW2018 chronometer was used.
Sample calculation
The sample size calculation was based on the correlation coefficients between the variables, found in a pilot study with 20 individuals. Considering an alpha of 0.05, a power of 0.80 and assuming the lowest coefficient found in the pilot (ρ=0.30), between physical activity level and gait speed, the required sample would be 90 individuals [35]. This sample size is also sufficient for the regression analysis, considering the possible inclusion of four independent variables (BMI, lower limb strength, balance and physical activity), since the formula used for this calculation would be n=10 (k + 1), where k is the number of possible predictor variables to be included [36].
Statistical analysis
Descriptive analysis and normality tests (Kolmogorov-Smirnov) were calculated for all measures. Pearson's correlation coefficient was used to explore the relationships between gait speed and BMI and lower limb strength. Spearman's correlation coefficient was used to explore the relationships between gait speed and balance and physical activity. The strength of the correlations was classified as low (<0.30), moderate (0.30 to 0.50) or strong (>0.50) [37]. Step-wise multiple linear regression analysis was used to show which independent variables would be able to explain gait speed. This analysis uses specific statistical criteria to maintain or eliminate outcomes that explain the dependent variables. All analyzes were performed using the SPSS 17.0 statistical package for Windows, with a significance level of 5%.
RESULTS
Characteristics of participants
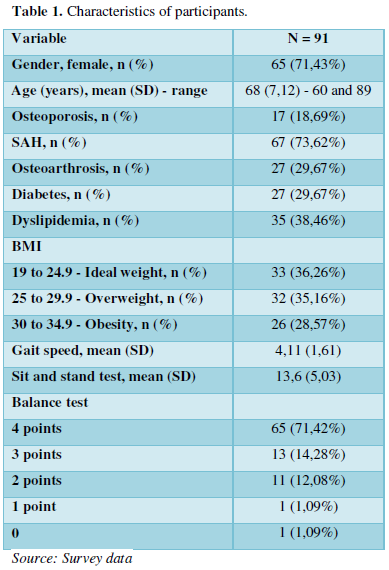
The sample consisted of 91 individuals. The age of the individuals ranged between 60 and 89 years, with a mean of 68 years and standard deviation of 7.12. Of the total, 65 patients (71.43%) were female; 7 (7.69%) were alcoholics and 6 (6.59%) were smokers. The pathologies reported by the participants through the anamnesis or exams were Osteoporosis 17 (18.69%), Systemic Arterial Hypertension (SAH) 67 (73.62%), Osteoarthrosis (AO) 27 (29.67%), Diabetes Mellitus (DM) 27 (29.67%), Dyslipidemia 35 (38.46%). The number of medications used per day ranged from 0 to 13 units, with an average of 4.10. The summarized data are shown in Table 1.
Correlation between walking speed and BMI and lower limb strength
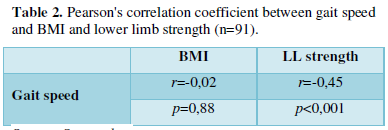
There was no correlation between BMI and gait speed (p>0.05). The correlation between gait speed and lower limb strength was significant, negative (inversely proportional) and of moderate magnitude (r=-0.45; p<0.01), suggesting that the longer the time spent to perform the sit and stand test, lower walking speed (Table 2).
Correlation between gait speed and balance and physical activity
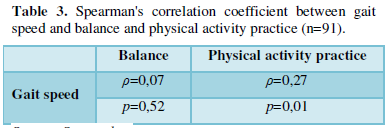
There was no correlation between gait speed and balance (p>0.05). The correlation between gait speed and physical activity practice was significant, positive (proportional) and of low magnitude (ρ=0.27; p<0.01), suggesting that individuals who practice physical activity have greater speed of gait (Table 3).
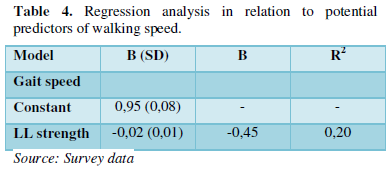
The variables included in the regression analysis, as potential predictors of gait speed, were physical activity practice and lower limb strength, variables that achieved a significant correlation. After the analysis, only the lower limb muscle strength remained in the model, being able to explain 20% (p<0.001) of the variation in gait speed (Table 4).
DISCUSSION
This study aimed to evaluate and establish the predictors of gait speed in the elderly, evaluating a possible correlation between BMI, physical activity, lower limb muscle strength and balance. As in two other Brazilian surveys on sarcopenia, most participants were women; the rate of women ranged between 70 and 95% [24,38] taking into account that women take more care of themselves, go more to the doctor, are always concerned about their health, while men do not always seek help and have less healthy lifestyle habits than women [38]. Moreover, females are more likely to become sarcopenic. The results showed significant correlations between gait speed and lower limb strength, suggesting that the lower the muscle strength, the longer the time spent to cover a distance of 3 meters. Many years befor, Buchne [39], in a study carried out with 409 elderly people, reported a significant correlation between lower limb strength and gait speed. Sowers et al. in their observational study, correlated for the first time the decrease in lean mass common to aging with lower limb strength and gait speed. Since then, other authors have confirmed the statement that strength training improves speed and gait stability in the elderly, among them, the work of Garcia et al. Carried out with 81 elderly Brazilians and who used the isokinetic dynamometer to assess the muscle strength of the lower limbs. In Moreira, Perez and Lourenço´s study, data from 745 elderly Brazilians were analyzed and a relationship was found between sarcopenia with advanced age, caucasian race, single marital status, low income and the presence of comorbidities. The population of the present study was much smaller, but with similar characteristics and, therefore, it would be valid to measure the percentage of sarcopenic elderly. From what has been seen in recent publications, the gold standard for early diagnosis of sarcopenia is computed tomography [40] while it is difficult to access for a large part of the population, other tests continue to be the most accessible options used in clinical practice. The present study also demonstrated that the practice of physical activity has a significant correlation between gait speed, suggesting that individuals who practice physical activity have greater gait speed. According to Santos [41] in one of their studies, they identified a statistically significant difference in gait speed in the groups that performed physical activity [41]. These data corroborate other studies that also identified the change in speed, amplitude variation, direction and different environments with the practice of exercises [42]. In the research by Matsudo and Neto it was evident that the practice of regular physical exercise reduces the risk of falls, increases muscle strength in the lower limbs and spine, improves motor synergy and postural reactions, improves speed of gait, mobility and flexibility. Finally, a meta-analysis carried out by Busk with 8 clinical trials demonstrated that external electrical stimulation combined with activity improves functional motor ability and gait speed in patients who have experienced stroke within the last 6 months. Such findings demonstrate possible fields of action of the rehabilitation professional in geronthology, both in prevention and treatment. Regarding the nutritional status of the elderly, the results showed that 35.16% were overweight and 28.57% were obese, totaling 63.73% of individuals with a high percentage of body fat. It is known that adipose tissue peaks occur between 60 and 70 years of age, and that this nutritional transition is associated with changes in eating behavior and a reduction in the degree of physical activity of individuals in this age group [43]. When this body composition undergoes changes, the functional decline tends to worsen, certainly due to the decrease in fat-free mass and the increase in fat mass. Regarding BMI, no significant correlation was found with gait speed. However, for some authors, the body composition of the elderly has been considered as one of the components of physical fitness such as flexibility, balance, muscle strength and aerobic endurance. It is believed that the choice of calculating BMI, weight for height, is not the best way to assess body composition, as it does not reveal the reality of the individual's health, healthy weight, lean mass and muscles, which may erroneously sort it out. One criticism is that there was no assessment of grip strength and Bioimpedance (BIA) of the 26 elderly people evaluated in 2020, therefore, these data could not be evaluated in the total sample. If included in the regression analysis, perhaps the findings would be more significant, given that they are important tools for identifying sarcopenia Thus, further studies are suggested, using more reliable calculations such as BIA, skinfolds and densitometry. According to Heyward, Stolarczyk skinfold measurement is widely used to estimate the amount of body fat due to its ease of use, good accuracy and low cost compared to other techniques. BIA is a non-invasive, inexpensive, portable and fast method used to measure body composition, based on the relationship between the volume of a conductor and its electrical resistance [44]. The variables mentioned above, such as old age, sedentary lifestyle, high blood pressure and obesity, lead us to a common deniminator: type 2 diabetes mellitus (t2DM). Identified in almost 30% of this sample, it is one of the main health problems worldwide. Pechman's study compared diabetic patients with controls and found, in diabetics, lower grip strength, higher rates of sarcopenia and osteoposis. Such data alert us to the need for early assessment in this type of patient [45]. According to Mesinovic, Zengin, Courten, Ebelin, Scott there are numerous links between T2DM and sarcopenia, such as insulin resistance, inflammation, increased oxidative stress and vascular complications. These factors may affect various components of muscle health and the existence of one condition may increase the risk of developing the other. This is what they called a bidirectional relationship. No significant correlation was found with gait speed and static balance, and this can be explained by the type of test used (with a ceiling effect and a result on a classification scale and not on time). It is known that decreased balance causes postural changes, especially in the sagittal plane, as a strategy to keep the center of mass within the limits of the body's base of support, such changes cause a decrease in gait speed [46]. Santos [41] show that older adults with lower balance scores on the Berg scale had lower gait speed, correlating body balance with gait speed. It is believed that the choice of the sample composed of elderly people from the community, able to seek health care and who were willing to go to the clinic where the data for this study were chosen, directly interfered in the results regarding balance. Thus, the active lifestyle positively interfered in the postural stability conditions of the elderly participants. Thus, it is suggested that further studies be carried out, with different elderly populations, comparing muscle mass and static balance. Mariana [47] state that for muscle strength it is essential to maintain balance. Hauser et al in a study carried out with elderly people who, as well as this one evaluated the strength of the lower limbs, also statistically confirmed the correlation between balance and muscle strength. In this context, the study by Santos [41] showed that elderly people assessed with lower balance by the Berg scale had lower gait speed. As well as the application of dynamic and functional balance tests such as Berg Balance Scale (EEB), Up and Go Test (TUG), Barthel Mobility Scale, Tinetti Balance Scale could be a differential in the result [10,41]. According to Ribeiro, Pereira 2005, these assessment instruments show excellent reliability and this scale has excellent test and retest objectivity (ICC=0.98) [48,49]. Structural and functional changes resulting from aging, such as strength and gait speed, proven in this study, lead to changes in activities and social participation and are perceived by the elderly [28,50]. Sitting and getting up from seats, carrying objects, walking at a safe speed, climbing and descending stairs are vital activities for the health and independence of the elderly [50,51]. In this context, one of the limitations of this study was the failure to investigate how much these changes interfere in important functional activities specific to each individual. One of the ways to carry out this assessment would be the use of questionnaires on activities of daily living (ADL) and instrumental activities of daily living (IADL), such as the Katz, Lawton or Pfeffer questionnaires, which are accessible, easy to apply and allow tracking rapid decline in functionality in various populations [5,52]. The association of vascular and metabolic comorbidities should also be further explored, as they contribute to the loss of muscle mass and strength The main positive point of the present study is the realization of a quick and easily applied assessment in clinical practice.
CONCLUSION
The present study showed that lower limb strength and physical activity were correlated with gait speed, but not significantly correlated with balance and BMI. New studies, with a broader population and more specific tests, are needed to clarify the behavior of BMI and Balance when compared to gait speed linked to senescence.
- Alexandre K, Renato PR, Roberto RL (1987) O envelhecimento da população mundial: um desafio novo. Rev. Saúde Públ., São Paulo 21(3): 200-201.
- Luciana CA, Beatriz CQ, Maria ELV, Marilia SC, Ana Glória GV (2007) The effect of chronic diseases on functional status of the elderly living in the city of São Paulo, Brazil. Cad Saude Publica 23(8): 1924-1930.
- Aline CT (2009) Evaluation of functional activity in older adults undergoing soil kinesiotherapy. J Neurosci 17(1).
- Linda PF, Catherine MT, Jeremy W, Anne BN, Calvin H, et al. (2001) Frailty in older adults: Evidence for Phenotype. J Gerontol 56(3): M146-M157.
- Gary F, Jackson B, Thomas MJ, Howard M, Jaffe W, et al. (1963) Studies of Illness in The Aged. The Index of Adl: A Standardized Measure of Biological and Psychosocial Function. JAMA, Chicago 185(12): 914-919.
- Luigi F, Jack MG, Marcel ES, Linda PF, Karen BR, et al. (1996) Effect of age and severity of disability on short-term variation in walking speed: the women’s health and aging study. J Clin Epidemiol 49(10): 1089-1096.
- Robert WB, Sarah HY, Kathleen MJ (2003) A longitudinal study of gait and balance dysfunction in normal older people. Arch Neurol 60(6): 835-839.
- Rebecca QILB, Robert GC, Paul M, Karin A (2006) Visual Impairment and falls in older adults: The blue mountains eye study. J Am Geriatr Rev Bras Geriat Gerontol 8(1): 9-20.
- Máximo PLS, Valadares BF, Almeida MT (1999) Avaliação da marcha em idosos/Gait Assessment in the Elderly. O Mundo da saúde 23(4): 221-228.
- Tinetti ME (1986) Performance - oriented assessment of mobility problems in elderly patients. J Am Geriatr Soc 34(2): 119-126.
- Goodarz D, Eric LD, Dariush M, Ben T, Jürgen R, et al. (2009) The Preventable Causes of Death in the United States: Comparative Risk Assessment of Dietary, Lifestyle, and Metabolic Risk Factors. PLoS Med 6(4): e1000058.
- Sanna S, Taina R, Eino H (1998) Physical activity and survival in elderly people: a five-year follow-up study. J Aging Phys Act 6: 133-140.
- Natália MO, Rogéria S (2006) Efectos de la actividad física en huesos normales y en la prevención y tratamiento de osteoporosis. Rev Bras Med Esporte 12(3).
- Laura SA, Annemarie K, Marjolein V (2013) Adiposity, Muscle Mass, and Muscle Strength in Relationto Functional Decline in Older Persons. Epidemiol Rev 35: 51-65.
- Vincent HK, Vincent KR, Lamb KM (2010) Obesity and Mobility Disability in the Older Adult. Obes Rev 11(8): 568-579.
- Momoko Y, Tome I, Midori K, Mitsuhiro M, Noriaki I (2017) Correlation between movement complexity during static standing and balance function in institutionalized older adults. Clin Interv Aging 12: 499-503.
- David AW, Aftab EP, Milad I, William HG (2003) Motor mechanisms of balance during quiet standing. J Electromyogr Kinesiol13(1): 49-56.
- Studensk S, Wolter L (2002) Instability and falls. In: Duthie, EH, Katz PR, organizers. Practical geriatrics. 3rd Rio de Janeiro: Revinter pp: 193-200.
- Natalia MP, Marcel JPMA, Marcos S (2019) Effectiveness of a Treadmill Training Programme in Improving the Postural Balance on Institutionalized Older Adults. J Aging Res 2020(3): 1-7.
- Teresa LA, Jennifer CD, Lindsay SN, Chun LH, Lindsay AK, et al. (2010) Changes in executive functions and self-efficacy are independently associated with improved usual gait speed in older women. BMC Geriatr 10(25): 1-8.
- Teresa LA, Lindsay SN, Peter G, Beattie BL, Maureen CA (2010) Resistance Training and executive functions: a 12-month randomised controlled trial. Arch Intern Med 170(2): 170-178.
- Friedman PJ, Richmond DE, Baskett JJ (1998) A prospective trial of serial gait speed as a measure of rehabilitation in the elderly. Age Ageing 17(4): 227-235.
- Verghese J, Jeannette M, Ambrose AF, Cuiling W, Roee H (2010) Effect of cognitive remdiation on gait in sedentary seniors. J Gerontol: Med Sci 12: 1338-1343.
- Roberto AL, Virgílio GM, Eliane FCB, Danielle VG, Kelly CAS, et al. (2019) Prevalence of frailty and associated factors in a community-dwelling older people cohort living in Juiz de Fora, Minas Gerais, Brazil: Fibra-JF Study. Ciênc Saúde Coletiva 24(1): 35-44.
- Subashan P, Kushang VP, Caterina R, Susan MR, Suzanne S, et al. (2016) Gait speed predicts incident disability: A pooled analysis. J Gerontol A Biol Sci Med Sci 71: 63-71.
- Luigi F, Stefania B, Enrico B, Angelo DI, Claudio M, et al. (2000) Subsystems contributing to the decline in ability to walk: bridging the gap between epidemiology and geriatric practice. In CHIANTI Study. J Am Geriatr Soc 48(12): 1618-1625.
- Álvaro CCM, Louise MA (2010) Factors associated with alterations in the gait speedand hand grip in institutionalized elderly. Rev Bras Geriatr Gerontol Rio de Janeiro 13(2): 179-189.
- Joelita PO, Anita LN (2014) Gait speed, grip strength and self-rated health among the enderly: data from the FIBRA Campinas network, São Paulo, Brazil. Cien Saude Colet 19(8): 3343-3353.
- Lilian AS, Kelly CA, Eliana BFC, Danielle VG, Roberto AL, et al. (2018) Gait speed, falls and fall self-efficacy as predictors models of frailty. Rev HUPE 17(2): 67-72.
- Anelise PO, Lilian RLA, Poliana RA, Deivis C (2019) Gait speed: The six vital signs as a predictor of health outcomes. RBPFEX 13(87): 1318-1322.
- Maria HL, Larissa SS, Susanne EB, Clóris RBG, Regina B, et al. (2019) Gait speed and occurrence of falls in the long-lived elderly. REME 23: 1190-1195.
- Rômulo DN, Aline SM, Victor ZD (2011) Usual gait speed assessment in middle-agedand elderly Brazilian subjects. Rev. Bras. Fisioter., São Carlos 15(2): 117-122.
- Alice MM, Barbara BG, Daniella MC, Gabriela VO, Kênia KPM (2020) Assessment of balance, gait, lower limb strenght and functionality in sarcopenic and non-sarcopenic enderlies. MTP Rehab J 18: 807.
- Renata MM, Renata CC, Márcio MN (2010) Funtional Capacity of elderly people living in a long-term care faility: A prospective study. Rev Bras Geriatr Gerontol Rio de Janeiro 13(2): 203-214.
- Leslie GP, Mary PW (2009) Foundations of clinical research - Applications to practice. 3rd Upper Saddle River: Pearson Prentice Hall. pp: 892.
- Ian RD, Wayne MS, Henrik S (2009) Veterinary Epidemiologic Research (2nd). Charlottetown, Canada: VER, Inc.
- Jacob C (1988) Statistical power analysis for the behavioral sciences. 2 edição. Hillsdale: Lawrence Erlbaum Associates Publishers. pp: 559.
- Maria LFF, Maria ART (2004) O Gênero (in)visivel da Terceira idade no saber da enfermagem. Rev Bras Enferm 57(6): 679-682.
- Devid MB, Eric BL, Edward HW, Koepsell TD, Barbara JL (1996) Evidence for a non-linear relation shipbetween leg strenght and gait speed. Age Ageing. Seattle 25(5): 386-391.
- Pankajakshan RS, Shikha SP, Anjana NKN, Arya R, Sandeep P, et al. (2020) Prevalence and associated factors of sarcopenia among patients underwent abdominal CT scan in Tertiary Care Hospital of South India. J Frailty Sarcopenia Falls 5(3): 79-85.
- Isabela RS, Rafael CC, Karin BSP, Samuel C, Andreia S, et al. (2016) Análise dos parâmetros da marcha e do equilíbrio dos idosos após exercícios aeróbicos e terapêuticos. Arquivo de Ciência e Saúde UNIPAR, Umuarama 20(1): 19-23.
- Carla H, Lucila P, Carolina PO, Pereira O, Jessika B (2013) Efeitos de diferentes modalidades de treinamento físico e do hábito de caminhar sobre o equilíbrio funcional de idosos. Fisioter Mov 26(2): 321-327.
- Andre H, Thomas L, Annette, Carolin E, Brigit W, et al. (2015) Prevalence and determinants of overweight and obesity in old age in Germany. BMC Geriatric 15(1): 1-13.
- Ian J, Steven H, Richard B, Robert R (2000) Estimation of skeletal muscle mass by bioelectrical impedance analysis. J Appl Physiol 89(2): 465-471.
- Pechmann LM, Jonasson TH, Canossa VS, Trierweiller H, Kisielewicz G, et al. (2020) Sarcopenia in Type 2 Diabetes Mellitus: A Cross-Sectional Observational Study. Int J Endocrinol 2020: ID 7841390.
- Eluciene MSC, Sâmara PFM, Guilherme PFS, João MCF (2011) A postura do idoso e suas implicações clínicas. Geriatria & Gerontologia. Fortaleza 5(3): 170-174.
- Mariana C, Patricia D, Julia G, Viviane DK, Jorge O (2013) Effects of a group-based exercise programon musclestrengt and postural control among community- Dwelling elderly women: a randomized-controlled trial. Revista Brasileira de Geriatria e Gerontologia. Rio de Janeiro 16(3): 527-540.
- Katherine OBDWS, Williams JI, Gayton D (1989) Measuring balance in the elderly: preliminar development ofan instrument. Physiotherapy Canada 41: 304-311.
- Angela SBR, John SP (2005) Improved balance and reduced chance of falling in the old women after the Cawthorne and Cooksey exercises. Rev Bras Otorhinolaringol 12(2): 113-122.
- Albert B (1986) The social foundations of thought and action: A social cognitive approach. Englewood Cliffs: Prentice Hall pp: 617.
- Anne SC, Marjorie HW (2003) A perspective of mobility throughout life: Motor control theory and practical applications. 2nd São Paulo: Manole. pp: 349.
- Powell L, Elaine MB (1969) Assessment of older people: Self-monitoring and instrumental activities of daily living. The Gerontologist, Washington 9(3): 179-186.
- Pfeffer RI, Kurosaki TT, Harrah CH, Chance JM, Filos S (1982) Measurement of functional activities in older adults in the community. J Gerontol 37(3): 323-329.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4




QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Advance Research on Alzheimers and Parkinsons Disease
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Journal of Allergy Research (ISSN:2642-326X)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Journal of Pathology and Toxicology Research


