
4744
Views & Citations3744
Likes & Shares
Abbreviations: TAD: Temporary Anchorage Device; MARPE: Micro-implant Assisted Rapid Palatal Expansion
“An implant is a device, made of one or more biomaterials that is purposely inserted inside the body & is either fully or partially buried under the epithelial surface” [1]. Linkow was one of the few authors of the ground-breaking studies in the field of oral implants & because of his pioneering work, he was also designated as ‘Father of Oral Implantology’.
Richard [2] observed that titanium screws were biocompatible with the bone tissues, & light microscopic examinations revealed bone to implant contact, leading to the development of the idea of osseointegration2. The usage of dental implants has dramatically increased during the last 20 years in dentistry [3].
The following potential benefits may result from using dental implants or implantable devices into modern orthodontic practice [3]:
- Serving as a technique to strengthen orthodontic anchoring.
- Reducing the total treatment time.
- Sometimes permitting orthodontic procedures achievable without surgery.
Anchorage loss, which is caused by the mechanics of tooth movement, is an unwanted tooth movement. Because of this, orthodontic devices are made with the intention of resisting unintentional tooth movement. Maximizing desired toot movement while minimizing negative effects is an essential aspect of therapy.
The main benefit of this kind of anchoring is that, implants offer skeletal anchorage, which is unquestionably more reliable and stable than approaches requiring patient cooperation. In order to broaden the scope of orthodontics, techniques have been developed during the past 60 years to establish absolute anchoring with the use of TAD’s [4].
An orthodontic anchoring device known as a TAD is a device that is temporarily secured to bone in order to support tooth or teeth of the anchorage unit (reactive), or by removing the need for the anchorage unit altogether & is to be removed thereafter on completion of utilization [4]. Anchorage devices can be classified based on their origin into 2 groups [5] i.e., Osseo-integrated dental implants & orthodontic mini-implants, palatal implants & retromolar implants.
According to Cope [4], skeletal anchorage can be categorized as biocompatible & biologic.
According to Labanaaskaite [6], classified implants as:
- On the basis of shape: Conical, Disk implants and Miniplate implants.
- On the basis of implant bone interface: Biomechanically retained and Osseo-integrated.
- On the basis of application: Prosthodontic & orthodontic implants.
- On the basis of method of insertion: Mini-screw implants, End osseous implants & Surgical miniplates.
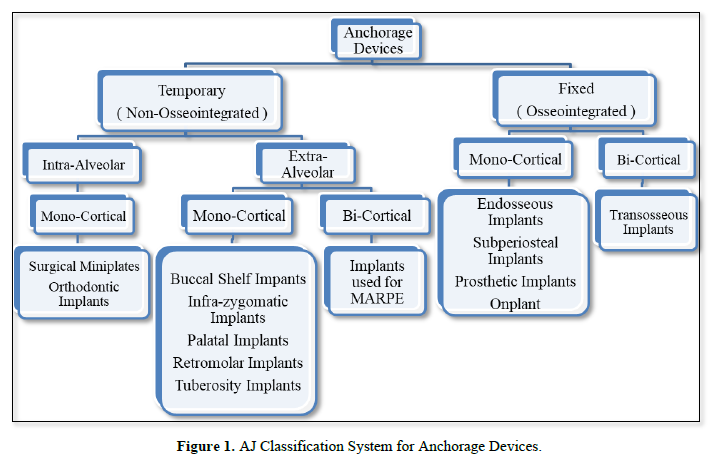
Since, the last classification was given in the year 2005 [4] and after that, there were many clinical material and technique innovations were done by various scientist and authors. Therefore, we propose this comprehensive classification with intention to improve upon older system of classification (Figure 1).
DISCUSSION
We have classified anchorage devices into 2 broad categories i.e., Temporary devices (Non-Osseo-Integrated) and Fixed devices (Osseo-integrated).
Temporary devices are further divided into Intra-alveolar and Extra-alveolar, on the basis of the area of their placement. Intra-alveolar implants generally penetrate only one cortical plate i.e., either buccal, lingual or palatal cortical plate. Therefore, divided into mono-cortical. Examples are surgical miniplates and orthodontic implants. Extra-alveolar implants can be used for single cortical penetration or bi-cortical penetration, therefore, sub divided into mono-cortical and bi-cortical. Some examples of mono-cortical are buccal shelf implants, infra-zygomatic implants, palatal implants, retromolar implants and tuberosity implants. Example of bi-cortical penetrating implants are the implants used for MARPE.
Fixed devices can be further divided on the basis of single or bi-cortical penetration, i.e., into mono-cortical and bi-cortical. The examples of mono-cortical penetrating implants are end osseous implants, subperiosteal implants, prosthetic implants and on plants. The example of bi-cortical penetrating implants are trans osseous implants.
CONCLUSION
With the aim to keep it simple and better for understanding, we have proposed this novel and comprehensive classification system for anchorage devices.
- Graber TM (1972) Orthodontics, Principles and Practice, 3rd edn.
- Sullivan RM (2001) Implant Dentistry and The Concept of Osseointegration: A Historical Perspective. J Calif Dent Assoc 29(11): 737-745.
- Heymann GC, Tulloch JFC (2006) Implantable Devices as Orthodontic Anchorage: A Review of Current Treatment Modalities. J Esthet Restor Dent 18: 68-80.
- Cope JB (2005) Temporary Anchorage Devices in Orthodontics: A Paradigm Shift. Semin Orthod 11: 3-9.
- Melsen B (2005) Mini-implants: Where are we? J Clin Orthod 39: 539-547.
- Labanaaskaite B, Jankauskas G, Vasiliauskas A, Haffar N (2005) Implants for orthodontic anchorage. Meta-analysis. Stomatologija 7: 128-132.

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Advance Research on Alzheimers and Parkinsons Disease
- Chemotherapy Research Journal (ISSN:2642-0236)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)



