
3477
Views & Citations2477
Likes & Shares
Anxiety caused by dental treatment is a common disorder that affects the patient’s cooperation with the dentist. Anxious patients may overestimate pain and therefore may need more time to reduce stress. Anxiety is a well-known phenomenon in dentistry, which is referred to as treatment fear in many studies. It seems that controlling the stress and anxiety of the patients improves their dental session [3].
It appears that the etiology of dental stress and anxiety is a combination of behavioral, genetic, and human factors, which are still poorly understood. Previous studies reported that the prevalence of dental stress varied across cultures. In addition, stress depends on many factors, including ethnicity, gender, and the economic, social, and literacy status of the person. If the dentist can understand the source of the patient's stress and anxiety, (s) he can control the patient better. Several studies have shown high stress levels in the field of endodontics. One of the reasons for this finding is the former dental patients recounting their experiences, including the injection pain, post-treatment pain, or pain between sessions, which may affect the stress level of the patients [4].
Some studies even found that dentists and dental students might experience stress during treatment due to the complexities of this field, which may be transmitted to patients [5].
The results of a survey by the American Society of Endodontics showed that the general perception of endodontic treatment is generally negative, which is mostly due to reports of pain associated with endodontic treatment. Wali [6] reported that 13% of their 200 patients did not attend the treatment sessions because of fear of pain.
Studies have shown that women have higher levels of dental fear and anxiety, and mothers, as a subset of women who receive dental services, may delay their children’s dental visits due to their own fears [8,7]. Dental fear and anxiety is very important because dental visits are necessary to maintain and improve the children’s oral and dental health. Dental caries is also considered a cost factor, and in this situation, any delay in receiving basic dental services or, in some cases, general refusal to receive them due to the stress of presence in medical centers can lead to a decrease in the level of oral health and subsequently public health [9].
Therefore, one of the important factors in receiving dental services is the mental preparation of the individual and society to reduce stress and anxiety caused by the dental environment. In a study of 200 mothers and children in India, demographic factors, information related to the Children's Fear Scale, and dmft(Decay, Missing, and Filled) index were collected. The results showed more dental caries in the children of the mothers with higher levels of anxiety. Some studies showed that anxiety could reduce the level of oral health of the individual and society [7,10,11]. Stress can be effectively controlled by creating a suitable learning environment or raising the individual's level of awareness, controlling unknown factors that can affect stress, counseling, establishing proper communication with others, and medication and therapy [12].
The complications of endodontic treatment and different treatment aspects can sometimes lead to reactions from the patient that exaggerate the expression of pain and fear, which can also affect the performance of the dentist [13]. Due to the nature of endodontic treatment, most patients experience pain during or after the treatment session. According to several studies, endodontic treatment is a stressful event for most patients. Knowledge of the factors that cause stress and anxiety for patients undergoing endodontic treatment helps to manage and overcome stress, provides peace of mind for the patient, and improves the quality of treatment. Considering the lack of comprehensive studies in this regard in Iran, we decided to design a study to explore the causes of dental stress.
METHODS
After receiving ethical clearance from the Ethics Committee of Qazvin University of Medical Sciences, the researchers visited Endodontics Department of Qazvin School of Dentistry and invited the volunteers to participate in the study.
First, the patient's need for endodontic treatment was confirmed by one of the professors of the Endodontics Department. Then, the patient was invited to participate in the study and the questionnaire was given to him/her. The researcher answered the patients’ questions regarding completing the questionnaire. If the questionnaire was not completed fully, the researcher asked the patient to complete it again.
The inclusion criteria were Iranian nationality, being a native resident of Qazvin, age above 18 years, confirmed need for endodontic treatment, lack of mental illness, not using psychiatric drugs according to the patient’s self-reports, and consent to participate in the study. The incompleteness of the questionnaire and refusal to continue participation in the study were considered as exclusion criteria.
The DASS (Depression-Anxiety-Stress Scale, a 21item questionnaire developed and validated by Lavibond in 1995 was used for data collection. This questionnaire has been translated and validated in Persian and used in several studies.
According to the DASS, the patient's stress and anxiety is classified as normal, mild, moderate, intense, and very intense. The answer options are scored in a 5-point Likert scale from 0 to 4. The total score of the questionnaire ranges from 0 to 84. The first part of the questionnaire is related to demographic characteristics, including age, sex, education level and occupation. The patients were asked about the history of dental visits and categorized to two groups as patients with a positive history and first-timers. Immediately after completing the questionnaire, the researcher checked it in terms of the accuracy of the answers and if there were any ambiguities, the patient was asked to correct it. All of the participants had OPG X-rays through which the researcher could easily discover a positive history of endodontic therapy. After careful evaluation and ensuring their completeness, the questionnaires were analyzed using the SPSS software version 24. One-way analysis of variance, t- test and Pearson’s correlation coefficient were used for data analysis.
RESULTS
Two hundred and fifty eight patients completed the questionnaires, of whom 129 were men and 129 were women, According to the results, the highest age frequency was seen in the 21-30 year-old group (n=93) followed by the 31-40 year-old group (n=57) and the 41-50 year-old group (n=49). The mean age of the patients was 32 years old. As for the education level, below high school education and high school diploma had the highest frequency and doctorate degree had the lowest frequency (n=30). Two hundred and seven participants had a positive history of dental treatment and 51 were first-timers. Moreover, 145 participants had a history of root canal treatment and 113 attended the dental school clinic for root canal treatment for the first time (Table 1).
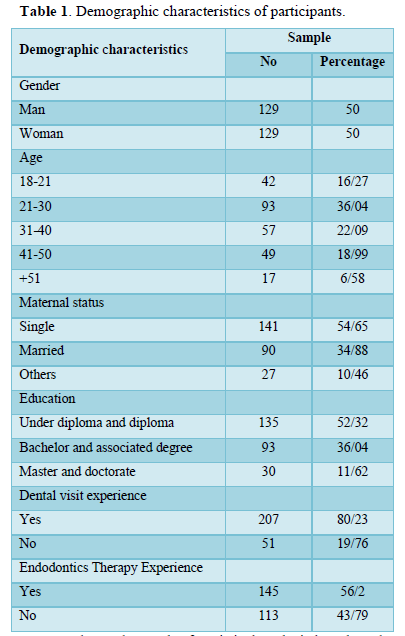
Table 2 shows the result of statistical analysis based on the participants Gender. According to t-test results, women had higher stress scores (48/37) compared to men (43/24) indicating a marginally significant difference (p=0.054).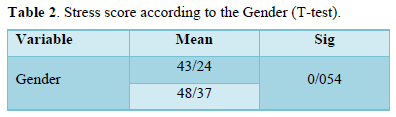
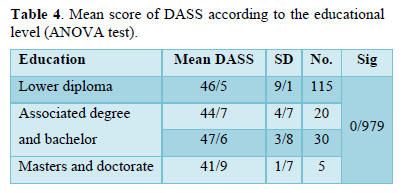
Table 3 shows that the relationship between the history of endodontic and dentistry treatment and the DASS stress. The patients with a history of endodontic treatment had significantly lower scores compared to the patients with a negative history. Also, T-test results showed a significantly lower mean score of stress and anxiety in patients with a positive history of dental visits compared to first-timers. According to the ANOVA results, the highest (47.6) and lowest stress score (41.9) was seen in patients with a bachelor's degree and those with a postgraduate education and doctorate, respectively. However, the difference was not statistically significant (Table 4).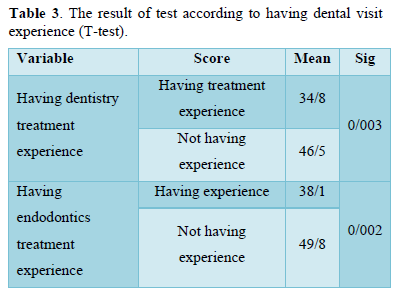
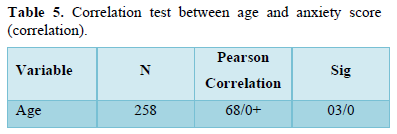
According to Table 5, the correlation coefficient of the relationship between age and DASS score was -0.68 indicating a negative significant correlation. In addition, comparison of this value with the tables of correlation coefficients suggested that this correlation was very strong, and the stress level decreased with age.
DISCUSSION
This study was conducted to investigate the factors affecting the stress and anxiety of patients requiring endodontic treatment in Qazvin Dental School in 2022. The standard DASS questionnaire, which is widely used in psychological studies at an international level, was used for data collection.
According to the results, gender may serve as a determinant of stress. The mean stress score was significantly higher in women than in men. This finding was similar to the results of studies by Riyadh Alroomy [3,15,16] that reported higher mean stress scores in women compared to men. This difference could be due to the mental structure of women who usually are more emotional and experience higher levels of stress [17]. As for the relationship between the history of dental treatment and stress score, the results showed a significantly lower stress score in the group with a positive history of treatment compared to the group with a negative history. This finding can be explained by the known or unknown effect of a phenomenon on the human mind in causing stress. In this regard, after undergoing dental treatment, people gain more self-confidence and trust in the dental office and overcome the stress more efficiently. This finding was similar to the results of a study by Grisolia [18] according to which a positive history of dental visits was effective in reducing fear. Regarding the relationship between the history of endodontic treatment and the stress score, the results showed a significantly lower mean score in the group with a history of endodontic treatment compared to the group with a negative history. Obviously, similar to the history of dental visits, a positive history of endodontic treatment can be effective in increasing self-confidence and confidence in an experienced person. This finding was similar to a study by Thomson [16] that found a positive history of dental treatment, including endodontic treatment, was effective in reducing stress. As for the relationship between the education level and stress score, the education level had no significant relationship with the stress score. The results showed that an increase in the education level resulted in a decrease in the mean stress score. The highest stress score was seen in patients with a bachelor’s degree and the lowest was observed in patients with a master’s or doctorate degree but the difference was not significant. The reason for this finding may be that stress is not a factor that is solely controlled by a person's education. People with higher education levels usually have a higher mean age than other groups. The bachelor level of education is associated with economic and social factors, and issues such as unemployment are very frequent in this educational group in Iran. Moreover, the stress associated with the urge to continue their education at the higher levels may have an even greater effect on stress in this group. On the other hand, gender and age were homogenous in the present study, indicating that some other factors may have stronger effects on the subjects compared to the education level [17,19].
Investigating the correlation between age and anxiety score showed a negative significant relationship between the two variables (-0.68). Thus, the stress level decreased with age. It should be considered that with an increase in age, the probability of a positive history of dental visits increases the person's experience and skills to deal with the life's problems are strengthened. This finding was similar to the results of a study by Elizabeth Carter in which the age groups above 40-65 years showed lower stress levels compared to the age group 20-39 years [20]. The results of a study by Elizabeth Carter [21], who compared Australian and Saudi Arabian populations and a study by Chen [2], who compared Chinese and non-Chinese populations, showed that racial, ethnic, and cultural differences changed the overall stress level. In order to control this variable, permanent residence in Qazvin was considered as an inclusion criterion in order to increase cultural homogeneity among the participants. The findings of the present study suggest dental fear is a general phenomenon embedded in human psychology and an effective factor in procedures such as endodontic treatment that causes more stress. One of the strengths of the present study was adjustment for some confounding variables. For this purpose, only patients who were native residents of Qazvin Province were included in the study in order to control cultural variables. Another advantage of this study was that it was conducted in an academic center (Qazvin University of Medical Sciences); as a result, the participants were economically homogeneous to a large extent. In addition, the patients aged less than 18 years were excluded; therefore, age was also controlled to some extent. Obviously, due to the different mental and psychological structure of children and adolescents compared to adults, it was not possible to have clear results if these age groups were not separated. Strength of the study was that it included more variables compared to other similar studies. This study had some limitations that need to be addressed. One of the limitations was COVID-19 pandemic, which reduced the available sample size. Similar studies should be conducted in younger age groups as well as patients visiting other private and public dental centers to measure the impact of economic differences on different parameters. Moreover, it is necessary to conduct studies in other departments of dental schools, such as the department of surgery, where the stress level is higher, or orthodontics and cosmetic departments, where stress levels are lower, to investigate the difference in the stress score between different dental conditions.
CONCLUSION
Demographic variables and a person's previous experience in dentistry can affect the level of stress.
- George S, Joseph BB (2018) Level of stress and its causes among 1st year dental students-a cross-sectional study. Natl J Physiol Pharm Pharmacol 8(11): 1518-1521.
- Chen WJ, Carter A, Boschen M, Love RM, George R (2020) Fear and Anxiety Pathways Associated with Root Canal Treatments Amongst a Population of East Asian Origin. Eur Endod J 5(1): 2-5.
- Alroomy R, Kim D, Hochberg R, Chubak J, Rosenberg PA, et al. (2020) Factors influencing pain and anxiety before endodontic treatment: A cross-sectional study amongst American individuals. Eur Endod J 5(3): 199-204.
- Liu P, McGrath C, Cheung GSP (2012) Quality of life and psychological well‐being among endodontic patients: A case‐control study. Aust Dent J 57(4): 493-497.
- Seijo MOS, Ferreira EF, Sobrinho APR, Paiva SM, Martins RC (2013) Learning experience in endodontics: Brazilian students’ perceptions. Int Dent Educ 77(5): 648-655.
- Wali A, Siddiqui TM, Gul A, Khan A (2016) Analysis of level of anxiety and fear before and after endodontic treatment. J Dent Oral Health 2(3): 19-21.
- Ain TS, Sultan S, Gowhar O, Ravishankar TL (2016) Maternal dental anxiety as a risk factor for dental caries in children: A cross-sectional study. Int J Res Med Sci 4: 4867-4872.
- Hägglin C, Hakeberg M, Ahlqwist M, Sullivan M, Berggren U (2000) Factors associated with dental anxiety and attendance in middle‐aged and elderly women. Community Dent Oral Epidemiol 28(6): 451-460.
- Bagramian RA, Garcia-Godoy F, Volpe AR (2009) the global increase in dental caries. A pending public health crisis. Am J Dent 22(1): 3-8.
- Goettems M, Ardenghi T, Romano A, Demarco F, Torriani D (2012) Influence of maternal dental anxiety on the child’s dental caries experience. Caries Res 46(1): 3-8.
- Khawja SG, Arora R, Shah AH, Wyne AH, Sharma A (2015) Maternal dental anxiety and its effect on caries experience among children in Udaipur, India. J Clin Diagn Res 9(6): ZC42.
- Anthony TE, Dee N, Bernard A, Lerchner W, Heintz N, et al. (2014) Control of stress-induced persistent anxiety by an extra-amygdala septohypothalamic circuit. Cell 156(3): 522-536.
- Martin T (2012) Predictors of pain associated with routine procedures performed in general dental practice. Community Dent Oral Epidemiol 40(4): 343-350.
- Bentley KH, Gallagher MW, Carl JR, Barlow DH (2014) Development and validation of the Overall Depression Severity and Impairment Scale. Psychol Assess 26(3): 815.
- Schwarz E, Birn H (1995) Dental anxiety in Danish and Chinese adults-A cross-cultural perspective. Soc Sci Med 41(1): 123-130.
- Thomson W, Poulton R, Kruger E, Davies S, Brown R, et al. (1997) Changes in self-reported dental anxiety in New Zealand adolescents from ages 15 to 18 years. J Dent Res 76(6): 1287-1291.
- Zlotnick C, Dryjanska L, Suckerman S (2022) Health literacy, resilience and perceived stress of migrants in Israel during the COVID-19 pandemic. Psychol Health 37(9): 1076-1092.
- Grisolia BM, Dos Santos APP, Dhyppolito IM, Buchanan H, Hill K, et al. (2021) Prevalence of dental anxiety in children and adolescents globally: A systematic review with meta‐analyses. Int J Paediatr Dent 31(2): 168-183.
- Cairney J, Boyle M, Offord DR, Racine Y (2003) Stress, social support and depression in single and married mothers. Soc Psychiatry Psychiatr Epidemiol 38(8): 442-449.
- Carter AE, Carter G, Boschen M, AlShwaimi E, George R (2015) Ethnicity and pathways of fear in endodontics. J Endod 41(9): 1437-1440.
- Carter AE, Al Shwaimi E, Boschen M, Carter G, George R (2019) Influence of culture change on the perception of fear and anxiety pathways in Endodontics: A pilot proof of concept study. Aust Endod J 45(1): 20-25.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5





QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Chemotherapy Research Journal (ISSN:2642-0236)
- Advance Research on Alzheimers and Parkinsons Disease
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)



