
4117
Views & Citations3117
Likes & Shares
INTRODUCTION
Individuals who understand and incorporate the knowledge and establish a sense of personal control over their oral health are more likely to follow self-care practices.
Lesser data are available on oral health awareness from developing countries. Reasonably insufficient amount of oral health awareness and practice occur amongst the Indian community compared to western countries [3,4]. Unfortunately, oral health is given last priority by policymakers in India as the authorities are inadequately informed about the burden of dental problems and its association with systemic health [5]. Also, several studies suggested that most health care providers were not aware of the association between oral health and general health problems [6]. It is evident from the available dental literature that many oral diseases are preventable with proper education or awareness. Although, good oral health practices and knowledge regarding oral health are associated with better oral health status among a varied group of the population of children, adolescents, and even university students. The available oral health education programmes are deficient in content, achieves only short-term behavioral change and doesn't address faulty oral hygiene practices in people [7].
Dental professionals are expected to participate in oral disease prevention, but their approach is limited to curative means rather than preventive. There are reports that patients only visit the dentist when in pain and never bother to return for follow-up in most cases [8-10]. Therefore, while developing any health promotion program, teachers are sole members since they are usually the first line of advice to the student as they interact with them daily, and have close contacts with their families. Moreover, teachers are role models for the children and can encourage young people to develop positive attitudes towards oral health. Hence the way teachers perceive their role in the health and social well-being of students becomes far-reaching. However, inadequate oral health knowledge, lack of training, and support for teachers in this regard create a barrier for effective implementation of health education programs [5,7].
To help dental professionals to design necessary programmes intended to train this population and enable them to educate the students about different aspects of oral health and its maintenance, the present pilot study was done to measure the awareness of university teachers in India towards oral health and dental aesthetics. The aim of this cross-sectional survey was to assess the knowledge, attitude and practices towards oral health and dental care amongst the government university teachers attending an academic staff college in India.
METHODOLOGY
A descriptive cross-sectional survey was conducted by the author (H.K) during the orientation/ refresher courses for the university teachers at the UGC Academic staff college, Jamia Millia Islamia. Since the study is observational research of public behavior, it was taken with less than minimal risk with no linked identifiers and was exempted from ethical review. The ethical approval for the study was taken from the institutional ethical committee. [Proposal no 7 (17/12/307/JMI/IEC/2020)].
The sample of this pilot study included the faculty members enrolled in the courses and presently working as faculty in various university positions in India. Those who have had training on oral health such as Dental/ Medical faculty were excluded. All the faculty who gave a written informed consent to participate was enrolled in the study. A self-administered questionnaire was used to obtain information on demographics, knowledge of the impact of oral health on daily life activity, self-reported oral health status, as well as their oral hygiene practices (Table 1). The questionnaire was piloted for feasibility and validity prior to finalization.
The questionnaire was a close-ended questionnaire and included 20 items designed to assess the knowledge (9 questions), attitude (5 questions) and practices (6 questions) of university teachers of the public sector towards oral health and dental treatment. The subjects were encouraged to respond to each of the items compulsorily and were asked to approach the investigator (H.K) available in case they needed any clarification at any point.
STATISTICAL METHODS
The data compiled on a workbook (Microsoft® Excel for Mac, version 16.46) and analyzed using Statistical Package for Social Sciences SPSS for Windows, version 22.0 (SPSS Inc.; Chicago, IL, USA). Descriptive statistical analyses were obtained and the frequency distribution within the groups as well as for the total sample was calculated. Further comparison between the groups was done using Pearson’s Chi-square test and the level of significance was set at p<0.05.
RESULTS
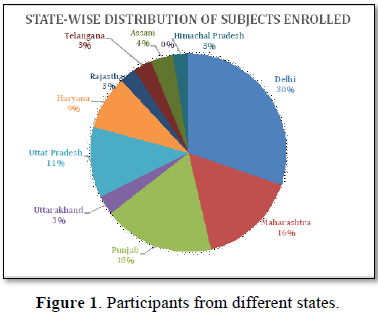
Out of 206 forms distributed, the average participant dropout rate was 6.7%. The data was collected from 192 university teachers- 109 Males (56%) and 83 Females (44%) attending the Academic staff college programme of Jamia Millia Islamia University in the academic years 2017-18. The participation covered 10 out of 29 states of India, majorly North India (30% Delhi, 18% Punjab, 11% Uttar Pradesh, 9% Haryana, 3% Himachal Pradesh, 3% Uttarakhand) followed by Maharashtra (16%), Assam (4%) Telangana (3%) and Rajasthan (3%) (Figure 1).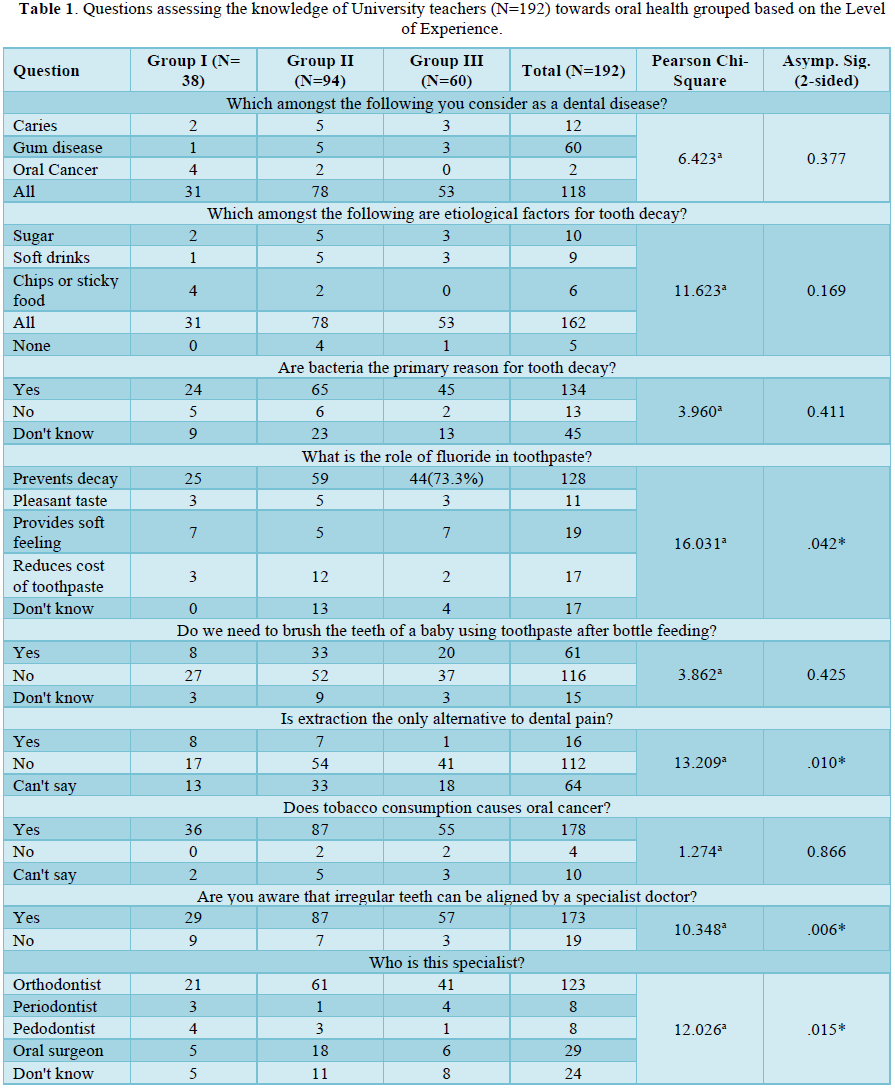
The mean age of the participants was 36.26+/- 5.86 years (minimum 24 years and maximum 56 years). While 184 (95.8%) of the teachers were assistant professors, only 8 were Associate professors. Henceforth, based on years of experience, the participants were further divided into 3 groups: Group I= up to 5 years (N= 38; 17.9 %, mean age 31.98), Group II- 5-10 years (N= 94; 48.4%, mean age 37.06) and Group III- more than 10 years (N=60; 33.7 %, mean age 40.3). The results for each group for the knowledge, attitude and practices towards oral health are shown in Tables 1-3.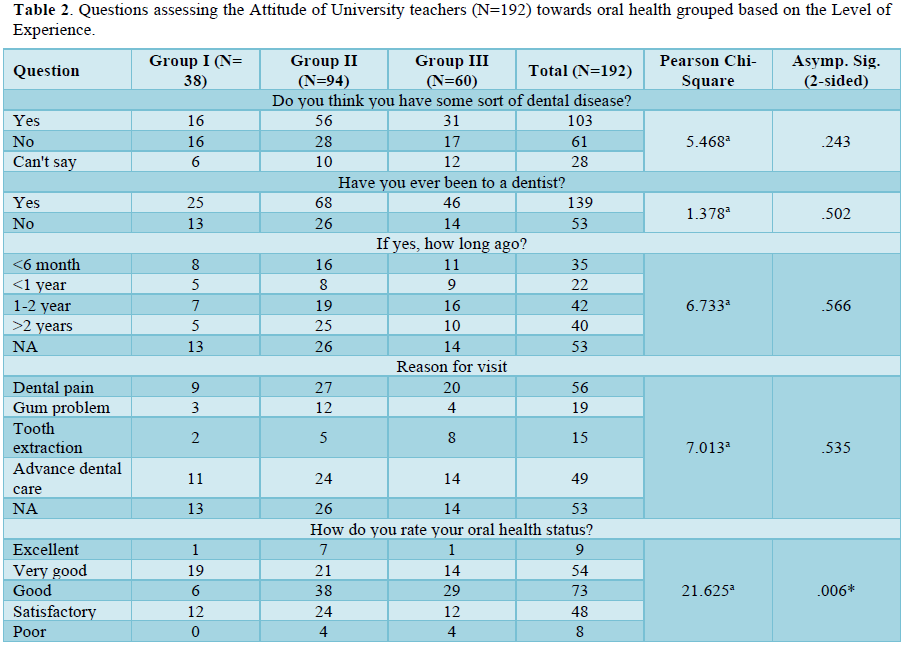
DISCUSSION
According to WHO bulletin, 2005, “Worldwide, the prevalence of dental caries among adults is high as the disease affects nearly 100% of the population in the majority of countries [11]. Oral health is an integral component of general health, a tenet; no one can disagree with [12]. In 2016, when India’s first state-wise global disease burden (GDB) was done, oral health was not included, despite of high prevalence of many oral diseases like oral cancer, periodontal diseases, and dental caries. Therefore, over the last decade, assessment of consequences of impaired oral health from the patient's perspective has emerged as an important research area, leading to increasing measures to assess knowledge and attitude of people towards their oral health [13-15].
In this study, we collected data from 192 university teachers attending the Academic staff college program of Jamia Millia Islamia University, 2017-18. The gender distribution of the participants was 109 Males (56%) and 83 Females (44%) with mean age of 36.26+/- 5.86 years. This is unlike similar studies done for the school teachers, which mostly had female preponderance [16-19]. Since most of them were assistant professors by designation, we divided the participants into 3 groups, based on their teaching experience. The questionnaire was developed, having 20 questions focusing on 3 areas: knowledge, attitude and practices of university teachers towards oral health. We proposed the null hypothesis, that younger faculty should have better knowledge and awareness, based on the fact they are much more active and exposed to social media [17].
For the questions relating to the knowledge of oral health issues, all 3 groups were well aware of oral health measures with no statistically significant difference between the groups for most of the questions. Group III showed a significantly better response to the questions such as alternatives to extractions for dental pain; use of fluoridated toothpaste to prevent tooth decay, and; irregular teeth to be aligned by a specialist orthodontist. Overall, the responses for all questions, such as dental caries as the primary reason for tooth decay, were positively higher/ better when compared to previous studies in school teachers or the adult population [20-22]. This observed finding could be associated with increased oral health awareness among people through public health programs, advertisements on social media and improving dental policies in India. Around 67% of the total respondents knew about fluoride importance where again Group III performed slightly better, this was inconsistent with a previous study done within school teachers in Mumbai where less than 50% of participants knew about the role of fluoride in their toothpaste [16]. More than 90% of the teachers knew about the importance of orthodontists in the treatment of malocclusion in contrast to the study done by Kim, where people in their 40s-50s had lowered interest [23].
Regarding their attitude towards oral health needs, slightly more than 50% of teachers have had some sort of dental disease and 72% have been to a dentist. Nearly 28% either did not ever visit a dentist or did not remember when they have had a dental sitting. The major reason for the visit had been dental pain (29%) followed by advanced dental care (25%). This is in correspondence/contrast (add both) to previous studies [24]. Most of the teachers rated their oral health status as good (38%) with Group III showing a statistically significant difference at 48%.
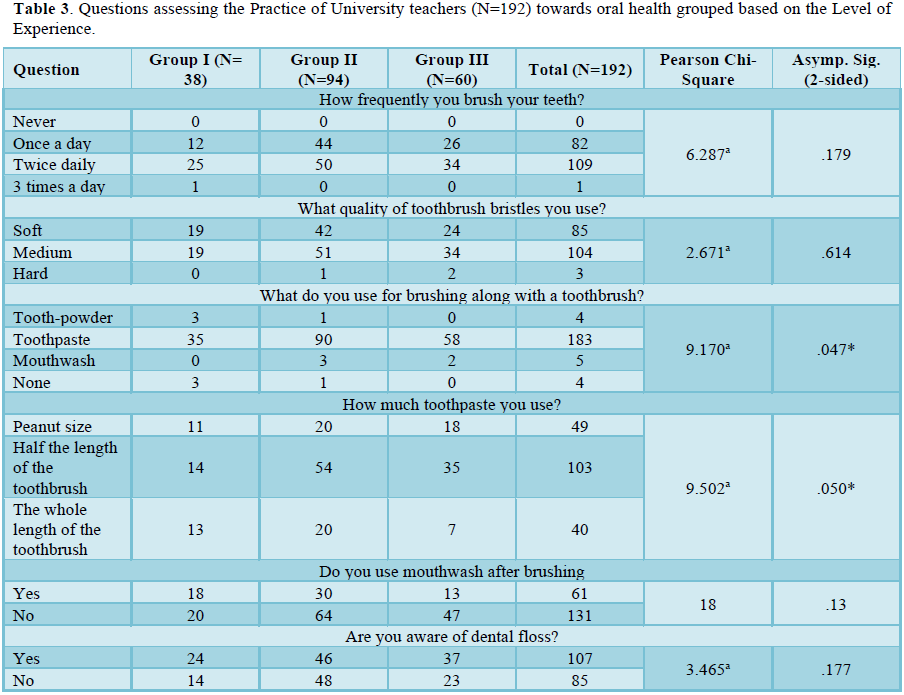
The younger population of teachers had slightly better oral hygiene practices than their senior counterparts, although the difference was not statistically significant. Overall, the teachers brushed twice daily (57%) with medium quality of bristles (54%) and primarily used toothpaste (95%), mouthwash (68%) and floss (55%). All these finding remains consistent with the previous studies [25,26]. The use of mouthwash and floss was more in group III teachers, which may relate to age-related care for oral hygiene.
One of the focuses of WHO-led oral health programmes in the target countries includes the development of methods and tools to analyze the process and outcomes of oral health promotion interventions as part of national oral health programmes [27]. In India, a nation with 17.5 % of the world’s population and 44 % of its population in productive age, imparting basic knowledge of primary oral health care is still missing. Not even 20% of rural PHCs in the country have a general dentist [21]. This demands a mandate of imparting oral health knowledge to all the public service providers, especially the educators. Currently, the literature mainly focuses on school children and school teachers [28,29]. To the best of our knowledge, this study was the first pilot run to assess the awareness of oral health issues amongst university teachers who have been overlooked till now. Our study was undertaken to assess the oral health knowledge, attitude and practices amongst government university teachers across India.
The findings of this study can be used to create dental awareness amongst university teachers, in planning oral health programs, implementing appropriate policies motivating self-care practices. However, some inherent limitations of this study should be noted. This study is just a pilot survey done on a small population of university teachers, consisting mainly of North Indian universities. Hence, further surveys (preferably standardized by a single questionnaire) in different universities across the country can be done and data from these can be compared for regional socio-demographic conditions of teachers. Also, actual practices practiced by the participants weren’t observed directly. There may be an associated recall bias overestimating the positive practices and underestimated negative ones. Despite the availability of one the authors for transliteration, since the questionnaire was in English and contained some dental terms, so subjects may have faced some difficulty or misinterpreted the questions.
However, we emphasize the fact that this study is the first of its kind focusing on teachers at a university level. Teachers are considered as role models to transmit the values of life. Teachers by virtue of their training can influence many students. Therefore, it is important that their oral health knowledge, behavior and practices comply with the expectations of the oral health practitioners to reduce the oral health burden of the society [21].
CONCLUSIONS
The overall goal of this pilot survey is to provide veritable information for the implementation, monitoring and evaluation of the existing national oral health policy, with more emphasis at the university levels. The level of knowledge and awareness amongst university teachers towards their oral needs did increase with experience and age. However, the younger population of teachers was better skilled in oral hygiene practices than their senior compeers.
ACKNOWLEDGEMENTS
The authors have no acknowledgements.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.
FUNDING
The authors report no funding.
- Sajjanshetty M, Rao A, Gururaghavendran R, Shenoy R, Pai BHM (2019) Oral health knowledge and practices: Their influence on oral health status of auxiliary health workers in health centers of Mangalore, India. J Indian Assoc Public Health Dent 17: 97-102.
- Singh S, Gupta N, Kaur M (2012) An assessment and comparison of oral health status among dental students and dental professionals of a teaching institute in Punjab, India using the Hiroshima University - Dental Behavioral Inventory (HU- DBI). Int J Public Health Dent 3(2): 9-15.
- Grewal N, Kaur M (2007) Status of oral health awareness in Indian children as compared to Western children: A thought provoking situation (a pilot study). J Indian Soc Pedod Prev Dent 25: 15-19.
- Diwan S, Saxena V, Bansal S, Kandpal SD, Gupta N (2010) Oral Health: Knowledge and Practices in Rural Community. Indian J Community Health 22(2): 29-31.
- National Oral Health Programme; 2015. Available online at: https://main.mohfw.gov.in/sites/default/files/N_56820_1613385504626.pdf
- Aggnur M, Garg S, Veeresha K, Gambhir R (2014) Oral Health Status, Treatment Needs and Knowledge, Attitude and Practice of Health Care Workers of Ambala, India - A Cross-sectional Study. Ann Med Health Sci Res 4(5): 676-681.
- National Oral Health Survey; 2002-2003. Available online at: https://ghdx.healthdata.org/record/india-national-oral-health-survey-2002-2003
- Hugoson A, Lundgren D, Asklöw B, Borgklint G (2007) Effect of three different dental health preventive programmes on young adult individuals: A randomized, blinded, parallel group, controlled evaluation of oral hygiene behavior on plaque and gingivitis. J Clin Periodontol 34(5): 407-415.
- Al-Ansari JM, Honkala S (2007) Gender differences in oral health knowledge and behavior of the health science college students in Kuwait. J Allied Health 36(1): 41-46.
- Gambhir RS, Brar P, Singh G, Sofat A, Kakar H (2013) Utilization of dental care: An Indian outlook. J Nat Sci Biol Med 4(2): 292-297.
- Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C (2005) The global burden of oral diseases and risks to oral health. Bull World Health Organ 83(9): 661-669.
- India State-Level Disease Burden Initiative Collaborators (2017) Nations within a nation: Variations in epidemiological transition across the states of India, 1990-2016 in the Global Burden of Disease Study. Lancet 390(10111): 2437-2460.
- Heather F, Harvey I, Needs K (2002) Oral health care education and its effect on caregivers' knowledge and attitudes: A randomized controlled trial. Community Dent Oral Epidemiol 30(2): 91-100.
- Nakre PD, Harikiran AG (2013) Effectiveness of oral health education programs: A systematic review. J Int Soc Prev Community Dent 3(2): 103-115.
- Shanbhog R, Raju V, Nandlal B (2014) Correlation of oral health status of socially handicapped children with their oral heath knowledge, attitude, and practices from India. J Nat Sci Biol Med 5(1): 101-107.
- Lang P, Woolfolk MW, Faja BW (1989) Oral health knowledge and attitudes of elementary schoolteachers in Michigan. J Public Health Dent 49(1): 44-50.
- Mota A, Oswal KC, Sajnani DA, Sajnani AK (2016) Oral Health Knowledge, Attitude, and Approaches of Pre-Primary and Primary School Teachers in Mumbai, India. Scientifica 2016: 5967427.
- Amith HV, D'Cruz AM, Shirahatti RV (2013) Knowledge, attitude and practice regarding oral health among the rural government primary school teachers of Mangalore, India. J Dent Hyg 87(6): 362-369.
- George B, John J, Saravanan S, Arumugham IM (2008) Oral health knowledge, attitude and practices of school teachers in Chennai. J Indian Assoc Public Health Dent 6(12): 20.
- Tangade PS, Jain M, Mathur A, Prasad S, Natashekara M (2011) Knowledge, attitude and practice of dental caries and periodontal disease prevention among primary school teachers in Belgaum City, India. Pesq Bras Odontoped Clin Integr João Pessoa 11: 77-78.
- Sakai VT, Oliveira TM, Silva TC, Moretti AB, Geller-Palti D, et al. (2008) Knowledge and attitude of parents or caretakers regarding transmissibility of caries disease. J Appl Oral Sci 16(2): 150-154.
- Sekhar V, Sivsankar P, Easwaran MA, Subitha L, Bharath N, et al. (2014) Knowledge, attitude and practice of school teachers towards oral health in Pondicherry. J Clin Diagn Res 8(8): ZC12-ZC15.
- Kim Y (2017) Study on the perception of orthodontic treatment according to age: A questionnaire survey. Korean J Orthod 47(4): 215-221.
- Maganur PC, Satish V, Marwah N, Vishwas TD, Dayanand MC (2017) Knowledge, Attitudes, and Practices of School Teachers toward Oral Health in Davangere, India. Int J Clin Pediatr Dent 10(1): 89-95.
- Zhu L, Petersen PE, Wang HY, Bian JY, Zhang BX (2005) Oral health knowledge, attitudes and behavior of adults in China. Int Dent J 55(4): 231-241.
- Asgari F, Majidi A, Koohpayehzadeh J, Etemad K, Rafei A (2015) Oral Hygiene Status in a General Population of Iran, 2011: A Key Lifestyle Marker in Relation to Common Risk Factors of Non-Communicable Diseases. Int J Health Policy Manag 4(6): 343-352.
- Petersen PE (2004) Challenges to improvement of oral health in the 21st century - the approach of the WHO Global Oral Health Programme. Int Dent J 54(6 Suppl 1): 329-343.
- Mishra A, Pandey RK, Chopra H, Arora V (2018) Oral health awareness in school-going children and its significance to parent's education level. J Indian Soc Pedod Prev Dent 36(2): 120-124.
- Lawal FB, Bankole OO (2014) Oral Health Awareness and Practices of Primary School Teachers in Ibadan, Nigeria. J West Afr Coll Surg 4(2): 47-65.
-
 Table 1
Table 1 -
Table 2
-
Table 3




QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- BioMed Research Journal (ISSN:2578-8892)
- Journal of Allergy Research (ISSN:2642-326X)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- International Journal of Diabetes (ISSN: 2644-3031)



