Journal of Psychiatry and Psychology Research (ISSN:2640-6136)

Research Article
Perceived Stress, Emotional Intelligence and Resilience Among Surgeons
6024
Views & Citations5024
Likes & Shares
Surgeons operate in the event of injury or disease and can perform number of different surgical procedures on the body and ensure all standards of care and safety. It is important to know the feelings or thoughts that an individual has about how much stress they are under at a given point in time, able to motivate oneself and restrain one’s impulse, recognizing and managing others emotions and handling interpersonal relationship in an effective manner and an ability to cope with a crisis or to return to pre-crisis status quickly. The present study aims to find out the significant gender difference in Perceived stress, Emotional intelligence and Resilience among Surgeons. The participants of the study include 15 Male Surgeons and 15 Female Surgeons. Purposive sampling method was employed for the collection of data. The participants were administered using Perceived stress scale was developed by Sheldon Cohen, the 14-item. Resilience scale was developed by Abiola and Udofia and Emotional intelligence Scale was developed by Hyde, Pethe and Dhar. Obtained results were analyzed using Independent samples to test and Karl Pearson’s Correlation Method. The result indicates there is no significant gender difference between Perceived stress, Emotional Intelligence and Resilience among Surgeons. There is significant relationship between Emotional intelligence and Resilience and also the study reveals that there is significant relationship between Perceived stress and Resilience. It indicates that when the level of Perceived stress increases, Resilience decreases.
Keywords: Perceived stress, Emotional Intelligence, Resilience, Surgeons
INTRODUCTION
Health professionals maintain health in humans through the applying of the principles and procedures of evidence-based medicine and caring. Health professionals’ study, diagnoses, treat and stop human illness, injury and other physical and mental impairments in accordance with the requirements of the populations they present. They advise on preventive and curative measures and support health with the last word goal of meeting the health needs and expectations of individuals and populations and improving population health outcomes. They also direct research and develop concepts, theories and operational methods to advance evidence-based health care. Their duties may include the direction of other doctors [1].
Physicians and surgeons diagnose and deal with injuries or illnesses. Physicians examine patients to take clinical histories, prescribe medications and interpret diagnostic tests. Surgeons operate on patients to deal with injuries, such as broken bones, illnesses such as cancerous tumors and deformities. In the case of surgery is an extremely stressful, intellectually demanding and satisfying career and many more people apply to become surgeons each year. Those who are successful have to be prepared not just to examine a notable deal, but have the proper form of character for the job. The impact of surgical intervention on public health system will continue to grow. Surgery is often the only therapy that can alleviate disabilities and decrease the hazard of death from common conditions.
Definition
A health care provider is a medical doctor who performs surgical operations. The surgeons decide the prognosis and provide the pre-operative care to sufferers and post- operative care to patients and are often accountable for the comprehensive management of trauma victim and the critically ill patient [2].
A surgery is a medical specialty that uses operative manual and instrumental techniques on a patient to examine and treat a pathological condition such as disease or injury, to help improve bodily function or appearance and sometimes for some other reason. An act of performing surgery may be called a surgical procedure, operation, or simply surgery. In this context, the verb 'operating' means performing surgery.
Among many different styles of surgeons, a wide spread healthcare professional is trained to perform surgical operation on most areas of the body. A standard health practitioner can diagnose and treat situations of the abdomen, extremities, smooth tissue, neck, breast or gastrointestinal structures by using Working in a clinical or medical institution setting. Five to seven years of training following medical college is certainly one of the requirements for this general practitioner doctor.
A surgical profession is among the most physically and psychologically demanding. In addition to acquiring large amounts of medical knowledge, surgeons need to grasp an increasing number of tough and constantly get surgical procedures; the protection of their patients relies upon on their maintaining interest on involute technical important points for continuous periods of time. These factors can motive to excessive amounts of stress. While limited quantities of acute stress may additionally enhance excessive amounts of intra operative stress can have disastrous results on surgical overall performance and affected person consequences. Excessive quantities of stress have been shown to negatively influence surgeon’s excellent motor skills, coordination and dexterity, emotional state, focus, teamwork, conversation skills, and decision-making ability. Mental-skills coaching are a distinguished vicinity of performance psychology [3].
Al-Zahrawi, the Islamic Golden Age doctor extensively considered one of the '"Fathers of Modern Surgery “The first individual to report a surgery used to be the sixth Century BC Indian physician-surgeon, Sushruta. He specialized in cosmetic plastic surgical treatment and even documented an operation of open rhinoplasty [4]. His magnum opus Susruta-saṃhita is one of the most necessary surviving historical treatises on medicine and is regarded a foundational textual content of both Ayurveda and surgery. The treatise addresses all aspects of common medicine; however, the translator G. D. Singhal dubbed Susruta "the father of surgical intervention" on account of the incredibly correct and designated accounts of surgical procedure to be found in the work [5]. After the eventual decline of the Sushruta School of Medicine in India, surgery was generally unnoticed till the Islamic Golden Age healthcare professional Al-Zahrawi (936-1013), re-established surgical procedure as a superb medical practice.
He is considered the biggest medieval health practitioner to have appeared from the Islamic World, and has also been described as the father of surgery [6]. His biggest contribution to medicinal drug is the Kitab al-Tasrif, a thirty-volume encyclopedia of medical practices. He was once the first medical doctor to describe an ectopic pregnancy, and the first doctor to identify the hereditary nature of hemophilia [7].
The present study focuses on the health care professionals in Surgeons of Male and Female Surgeons. There has been growing recognition of the reciprocal nature of the affiliation between work characteristics and mental health. Prior psychological distress may also negatively have an effect on current perceptions of the working environment and depressed temper is associated with human beings having a bad view of their surroundings, each of which might also confound the affiliation between present day working conditions and psychological distress [8].
A surgical career is considered to be gratifying but also very demanding. Traditionally, it was considered incompatible with women’s personal goals and family commitments. A surgical profession is regarded to be gratifying however additionally very demanding. Traditionally, it was considered incompatible with women’s private goals and family commitments.
Surgery as a specialty was historically considered to be a man’s domain. ‘Men take charge of the outside, female the inside’. This strong Chinese cultural belief would possibly reflect the unconscious gender-based assumptions and sex-role stereotypes: a woman’s job is usually an extension of domestic roles, the provision of care, rather than managing instruments and getting to know skills. That both men and women surgeons faced many difficulties in their working lives in special tiers of their surgical careers, with their coaching and career improvement affected via family commitments.
Women surgeons, as profession women, wives and mothers, need to strive for balance to fulfill these different stressful roles. Adequate focus for teaching and administration, cautious planning of departmental meeting times and policies protecting unanticipated child care would lessen the stress on woman as well as on male surgeons, and as a result enlarge their work affectivity and productivity. This would enable progress closer to an environment that attracts and retains the high-quality physicians, regardless of sex [9].
The most vital sources of stress were work overload, feeling badly managed and resourced, and managerial obligations and dealing with patients’ suffering, whilst perceived true relationships with patients, family and staff, and expert esteem made the greatest contribution to standard job satisfaction. Most of the surgeons in this find out about have been men and the large majority of nurses were women. As we have seen, no consensus exists in literature involving variations in burnout because of gender. However, longer working hours, on call commitments and terrible working stipulations and management help have all been proven to be related with higher burnout. It can only be postulated whether or not these mitigating factors exist greater in case of colorectal surgeons than colorectal nurse specialists [10].
Good interactional skills with the aid of surgeons are essential for a range of reasons. Surgeons are potentially quite potent function models for more junior fitness professionals, and for this reason it is essential that they efficiently mannequin suited interactional skills. Furthermore, given the nature of their work, they are in all likelihood to be in conditions in which a wide vary of interactional abilities are required, including breaking horrific news to patients, making ready them for surgery, teaching them about their condition, and detecting and dealing with anxiousness in patients. Educating sufferers about their circumstance was once additionally rated as vital with the aid of almost all of the surgeons, and its importance is supported by means of research which indicates that most sufferers want to be aware of as a lot as possible about their ailments which includes cause, treatment and prognosis, Although very few of the surgeons in this pattern perceived themselves to be incompetent at assignment this task, there used to be a high perceived want for formal education and evaluation of this ability as phase of surgical education courses [11].
Perceived stress
Perceived stress is about our feelings about the lack of control and unpredictability than the actual stressors. It measures the degree of stress a person feels about life; how much change is happening in one’s life and confidence in one’s capacity to deal with issues or difficulties. It is not measuring the types or frequencies of stressful situations which have occurred to a person, however rather how a person feels about the common stressfulness of their life and their capability to cope with such stress. Individuals may also go through similar negative life events but evaluate the impact or severity of these two different extents as a result of factors such as personality, coping resources, and support [12].
Stress is your body’s reaction to change that requires a response. These changes can be physical, mental or emotional, and can come from your environment, your thoughts. There are many causes of stress, a lack of control over important things and too much work or even not enough. Perceived stress is different. It’s more about your feelings about the lack of control and unpredictability than the actual stress. Perceived work stress is a serious issue. It can cause Tension, headaches, pain and fatigue, Digestive issues and stomach problems, Anxiety, irritability and anger, a lack of focus and motivation, Depression, Substance abuse, Sleep disorders and Eating disorders. Some of these are direct effects of stress, and some are unhealthy coping mechanisms. It is important then, to be aware of stress and keep it under control.
Perceived stress is not in simple terms assessing stressful life events but assessing the degree to which life situation are viewed stressful, which is the primary appraisal [13]. According to Lazarus and Folkman [13], this main appraisal (i.e., perceived stress) determines the degree of confidence people possessed concerning their capability to cope with stressful situations (i.e., secondary appraisal).
Surgical education and training are inherently stressful, and the ability to cope effectively with this stress is a critical facet of surgical competence. Acute stress defined as the physical, mental, or emotional response to a perceived increase in demand for motor, cognitive, or other performance is a particular problem in the operating room where the demands or stressors are numerous. A recent systematic review on the impact of stress on performance concluded that stress can impair both psychomotor and teamwork skills in novice surgeons, which has obvious implications for patient safety and surgical education. Although research has shown that there is significant variability in individuals' responses to stress and that these responses are affected by their cognitive appraisal of the stressful situation, little is known about the factors that account for these individual differences. Thus, it may be that certain personality traits put individuals at greater risk of experiencing stress during surgical challenges or confer them with an ability to better cope with stress [14].
Continued Individuals including surgeons have had to cope with and adjust to the rapid speed of development. As a result, work-related stress has become an interesting topic for the medical community as well as all other aspects of society. Work-related stress, both psychological and physical, arises frequently in the operating room. When stress becomes too high, job performance suffers. Excessive stress interferes with performance by diminishing a person's ability to cope and make correct decisions, and causes inconsistencies in behavior as well as frequent skipping [15].
In our daily life, stress is very usual and a normal thing. It is a physical reaction to an internal or external demand that is placed on an individual. It becomes a problem only when one feels challenged by its demands. Stress can define as a person’s response to anything that creates stress, a stressor.
The main sources of stress are problems with practice administration, patient anxiety, interruptions, patient’s expectations and demands, emergencies, work or home conflict, late arrival for appointments and the need to find one’s own patients. High stress and exhaustion have the capacity to negatively effect on work performance and patient care, including medication errors, clinical errors, and patient dissatisfaction [16].
Work-related stress is very common among health care workers. Health care providers around the world are subject to pressures that resulting from a rapid change, growing economic pressures, technological advances, increasing patient expectations, rationing of health care. The requirement for more evidence-based and high-quality health care is improved performance and productivity. It is very clear that health workers experience higher levels of stress and stress-related health problems than other occupational groups.
Physicians are revealed to many stressors, such as expectations of a high degree of professionalism, duty for patient well-being, and maintenance of relationships with patients and health workers. Studies have confirmed that up to 76% of residents meet the standards for burnout and that they have expressed career dissatisfaction, as well as concern that they supply suboptimal patient care. Residents report that the working conditions they are subjected to throughout residency lead to decreased attention, empathy, concern, and sensitivity, and increased irritability, abruptness, and a tendency to objectify patients [14].
According to Lazarus [13], “Stress arises when people become aware of that they cannot properly cope with the demands being made on them or with threats to their well-being”. Evidence indicates that both medical students and physicians experience higher symptom loads of psychological distress, depression, anxiety, and professional burnout than the average population [17].
Emotional intelligence
Emotional intelligence (EI) has recently emerged as a character characteristic that influences the perception of emotional and stressful situations. Early conceptualizations of EI referred to it as ability, a lot like cognitive ability, reflecting efficacy of affective data processing. hence, the usage of the term intelligence. EI used to be conceptualized as a personality trait in other words, not dispositions related to emotions. It refers to a constellation of emotional self-perceptions and essentially concerns people's self-perceptions of their emotional abilities [18].
Individuals with higher trait Emotional Intelligence scores show larger self-efficacy in coping with stress and greater in all likelihood than these with lower trait Emotional Intelligence scores to view potentially stressful tasks as challenges alternatively than as threats. Specifically, within medicine, latest systematic review published that Emotional Intelligence is associated to a variety of the core competencies that modern medical curricula are seeking to deliver, along with empathy, communication or interpersonal skills, and the ability to cope with stress effectively [19].
Emotional intelligence (EI or EQ) describes the ability to perceive, understand and manage one’s own and another person’s emotions the business world has long recognized EI as being meaningful and equally, if not more, important to success than technical and analytical skills [20].
Emotional intelligence (EI) has obtained much attention to generating intense demand for applications in educational, organizational and clinical settings. Many researchers distinguish between two Emotional Intelligence constructs, relying on whether the Operationalization process is primarily based on self-report or on most overall performance (as in IQ tests) [21].
Trait Emotional Intelligence (or trait emotional self-efficacy) issues emotion associated tendencies and self-perceptions measured through self-report, whereas ability Emotional Intelligence (or cognitive-emotional ability) issues emotion-related cognitive abilities measured through performance-based tests [18]. Emotional Intelligence is a personality trait, as adversarial to a cognitive ability; an essential question is where it belongs within established personality hierarchies. Theorists who suggest new person differences constructs ought to be in a position to reveal how these constructs relate to extant information in the field.
Emotional Intelligence is developmental and increases with age and experience. An individual’s Emotional Intelligence may also influence his or her ability to communicate effectively. Emotional intelligence has been defined as ‘a type of social intelligence that involves the ability to observe one’s own and other’s emotions, to discriminate among them, and to use this information to guide one’s own thinking and actions [22]. During consultations, doctors have to be able to make judgments about when to clearly discuss emotion and must also understand how patients or their relatives will perceive their emotional and instrumental behaviors. It can be assumed that Emotional Intelligence is associated with interpersonal competency [23].
Emotional intelligence provides a framework for interpreting individual differences in the recognition and management of emotive cues and concerns; individuals with higher levels of Emotional Intelligence may show more appropriate levels of emotional reactions and interpretations. A recent systematic review Arora [19], found significant positive correlations between undergraduate medical students’ Emotional Intelligence and their interpersonal skills, in which Emotional Intelligence was linked to communication skills in medical school entrance interviews [24].
Emotional Intelligence is important for surgeons and trainees to recognize understand and develop. The ability to handle through those waters affects patients, co-workers and he/she as challenging physically, mentally and emotionally is the surgical workplace.
Psychologist and author Daniel Goleman popularized Emotional Intelligence in the 1990s and found that successful Fortune 500 leaders were distinguished by high EI [25]. Individuals with high Emotional Intelligence seemed to perform better on the job and were more effective leaders.
Studies in the healthcare industry have suggested that high Emotional Intelligence can lead to improved doctor–patient relationships, empathy, teamwork and communication skills [19]. Components of Emotional Intelligence like empathy have been furthermore linked to higher patient satisfaction scores. Surprisingly few studies have focused on Emotional Intelligence in the surgical workplace and more research is needed [26].
Resilience
It refers to the capability of a strained body to recover its size and shape after deformation caused especially by compressive stress. Resilience theory refers to the ideas surrounding how people are affected by and adapt to things like adversity, change, loss, and risk. Being resilient does not mean that people don’t experience stress, emotional upheaval, and suffering. Some people equate resilience with mental toughness, but demonstrating resilience includes working through emotional pain and suffering. Resilience isn’t a fixed trait. Flexibility, adaptability, and perseverance can help people tap into their resilience by changing certain thoughts and behaviors.
Developing resilience is both complex and personal. It involves a combination of inner strengths and outer resources, and there isn’t a universal formula for becoming more resilient. All people are different: While one person might develop symptoms of depression or anxiety following a traumatic event, another person might not report any symptoms at all. A combination of factors contributes to building resilience, and there isn’t a simple to-do list to work through adversity. In one longitudinal study, protective factors for adolescents at risk for depression, such as family cohesion, positive self-appraisals, and good interpersonal relations, were associated with resilient outcomes in young adulthood [27].
People who lack resilience are more likely to feel overwhelmed or helpless, and rely on unhealthy coping strategies (such as avoidance, isolation, and self-medication). One study showed that patients who had attempted suicide had significantly lower resilience scale scores than patients who had never attempted suicide [28].
Resilient people do experience stress, setbacks, and difficult emotions, but they tap into their strengths and seek help from support systems to overcome challenges and work through problems. Resilience empowers them to accept and adapt to a situation and move forward. The 7 Cs of resilience illustrate the interplay between personal strengths and outside resources, regardless of age.
The American Academy of Pediatrics summarizes the 7 Cs as follows:
Competence: This is the ability to know how to handle situations effectively. To build competence, individuals develop a set of skills to help them trust their judgments and make responsible choices.
Confidence: Dr. Ginsburg says that true self-confidence is rooted in competence. Individuals gain confidence by demonstrating competence in real-life situations.
Connection: Close ties to family, friends, and community provide a sense of security and belonging.
Character: Individuals need a fundamental sense of right and wrong to make responsible choices, contribute to society, and experience self-worth.
Contribution: Ginsburg says that having a sense of purpose is a powerful motivator. Contributing to one’s community reinforces positive reciprocal relationships.
Coping: When people learn to cope with stress effectively, they are better prepared to handle adversity and setbacks.
Control: Developing an understanding of internal control helps individuals act as problem- solvers instead of victims of circumstance. When individuals learn that they can control the outcomes of their decisions, they are more likely to view themselves as capable and confident [29].
The study, published in September 2018 in the journal The Gerontologist, also showed that men with high resilience showed no additional depressive symptoms following a loss, and their overall well-being almost mirrored that of their married counterparts [30].
Resilience is that ineffable quality that allows some people to be knocked down by life and come back stronger than ever, the capacity to recover quickly from difficulties, often equated with toughness. Dean Becker, the President and CEO of Adaptive Learning Systems suggests that ‘more than education, more than experience, (and) more than training, a person’s level of resilience will determine who succeeds and who fails. That’s true in the cancer ward, it’s true in the Olympics, and it’s true in the boardroom’. I pose to you, members of the AAS, that it’s also true in surgery.
Physician wellbeing is surprisingly emphasized presently, with health practitioner burn- out (‘medical doctor distresses) defined as a mental country characterized via emotional exhaustion, depersonalization, and a diminished feel of personal accomplishment. Burn-out poses adverse consequences for both patients and clinicians and has been attributed to 5 key drivers including: excessive workload, inefficient work environment/inadequate support, problems with work-life balance, loss of autonomy/flexibility/control, and loss of meaningful work. Burn-out has clearly been linked to medical errors and complicates recruitment and retention into the field of Surgery (students, residents, fellows and faculty) with certain specialties more ‘at risk’ than others. Importantly, resilience may be predictive of resident and surgeon well-being.
Emotional resilience not only protects our mental and physical wellbeing, but also helps to prevent cognitive errors and enables us to care for our patients safely and effectively.
REVIEW OF LITERATURE
This section intends to outline the existing on Surgeons, Perceived stress, Emotional intelligence and Resilience.
Studies related on Perceived stress
Green [31] conducted a study about perceived stress in surgeons. They have taken sample of 1000 members of the Association of Surgeons of Great Britain and Ireland was circulated with a postal questionnaire relating to their occupational stressors, their type A coronary‐prone behavior and their mental health. Six hundred and seventy‐two (67 per cent) useable forms were returned anonymously. The major individual stressors were (1) the interference of the job with personal life, (2) general administration, and (3) the number of patients in clinics. Type A behavior was similar to that of other professional groups. The result showed that Surgeons showed mean scores significantly higher than the general population on two subscales of the mental health index. The findings for the few female surgeons (2 per cent) were similar to those in men but they did not exhibit raised free‐floating anxiety levels.
Westerman [32] conducted a study on Perceived sources of stress in the dental school environment. The study was aimed to identify the perceived stress of dental students across the entire curriculum. The dental environmental stress (DES) questionnaire was administered to 244 (90.4 percent) dental students during 1990. The result showed that there were significant differences were found for 12 questionnaire items across four classes. For male-female comparisons, significant differences were found for 17 questionnaire items, all perceived as more stressful by females; and between classes, significant differences were accounted for by three questionnaire items. Comparisons with previous dental students (1980s) on the identical questionnaire were noted.
Sanders [33] conducted a study was examined the relationship between perceived stress and academic performance in 202 dental students enrolled in an Australian dental school. In this study, four key stress factors labeled self‐ efficacy beliefs, faculty and administration, workload and performance pressure. The result of this research was that students reported higher levels of stress on the DES factor “faculty and administration” tended to show lower grades for clinical competency and contextual understanding.
Radcliffe [34] conducted a qualitative study on Perceived stress during undergraduate medical training which explored the views of Year 5 medical students on the causes of stress throughout their undergraduate medical training. The method of this study was conducted with 21 final year medical students at the University of Birmingham between January and May 2001. The study found that Pressure of work, especially in terms of preparing for examinations and acquiring professional knowledge, skills and attitudes were reported as the most stressful aspects of medical training. A perceived lack of support from the medical school authorities also appeared to add to student stress levels.
Pau [35] conducted a study to measure the relationship between emotional intelligence (EI) and perceived stress (PS) in dental undergraduates. In this research Two hundred and thirteen students (48 percent male) participated and a response rate of 70 percent. The mean score for Emotional Intelligence was 117.54 and Perceived Stress was 17.73. The result showed that low Emotional Intelligence scorers report more Perceived stress.
Maville [36] conducted a Qualitative study to explore the phenomenon of perceived stress by nurse practitioner (NP) students enrolled in a master of science in nursing program. The result showed that Students reported stress levels ranging from moderate to highest ever in their lives. Although reasons given for becoming a Nursing Practitioners included increased autonomy and increased ability, high-level stress was attributed to high demands and to independent teaching-learning techniques in the Nursing Practitioners courses. Participants also expressed concerns about time management and financial obligations.
Shah [37] conducted a study Perceived Stress, Sources and Severity of Stress among medical undergraduates in a Pakistani Medical School. The research study results showed that stressed cases were associated with occurrence of psychosocial and academic related stressors. The most common sources of stress were related to academic and psychosocial concerns. There was a negative but insignificant correlation between perceived stress and academic performance.
Abdollahi [38] conducted a study on Hardiness as a mediator between perceived stress and happiness in nurses. The participants, comprised 252 nurses from six private hospitals in Tehran, completed the Personal Views Survey, the Perceived Stress Scale, and the Oxford Happiness Inventory. Structural Equation Modelling (SEM) was used to analyze the data and answer the research hypotheses. As expected, hardiness partially mediated between perceived stress and happiness among nurses. The result showed that nurses with low levels of perceived stress were more likely to report greater hardiness and happiness. In addition, nurses with high levels of hardiness were more likely to report happiness. This study showed hardiness as being a protective factor against perceived stress and a facilitating factor for happiness in nurses.
Uzun [39] conducted a study to find the relationship between cultural sensitivity and perceived stress among nurses working with foreign patients. This study was implemented at the State Hospital in Kilis on the southeast border of Turkey, between June-July 2014. The study sample consisted of 120 nurses. Data collection tools included a questionnaire about the socio‐demographic and professional characteristics of participants. The result showed that the average score for nurse cultural sensitivity was 84·32 and the average score for perceived stress was 27·97, corresponding to a medium level. They identified negative correlation between cultural sensitivity and perceived stress.
Studies related on Emotional Intelligence
Wagner [40] conducted a study to find the relationship between patient satisfaction and physician’s scores on a test of emotional intelligence. Here the researchers used Bar-On Emotional Quotient Inventory (EQi) which completed by Faculty and resident physicians at a southern medical school. Results of the research was like this When patient satisfaction scores were used to dichotomize physicians into two groups, those with 100% satisfied patients and those with less than 100% satisfaction, only one subscale of EQi, “happiness” was related to higher satisfaction. This research concluded that a limited relationship between physician’s scores on a test of emotional intelligence and patient satisfaction.
Weng [41] conducted a study to explore the associations among doctor Emotional Intelligence, patient trust and the Patient Doctor Relationship using multi- source and multi-level approaches. The research consisted of 994 outpatients and 39 doctors representing 11 specialties were surveyed. In this research the studies showed that doctors’ self-rated Emotional Intelligence was not significantly correlated with any variables rated by the patients. The nurse-rated Patient Doctor Relationship and the Emotional Intelligence score for the doctor were positively associated with patient trust at a significant level. This research concluded that Multi-sources for assessment of doctor Emotional Intelligence may be more objective and predictive than doctor self-ratings in ascertaining the associations among patient trust, the Patient Doctor Relationship and patient satisfaction. Emotional intelligence coaching for doctors and interdisciplinary collaboration among clinicians are needed to optimize the efficient and therapeutic function of the Patient Doctor Relationship for patients.
Carr [42] conducted a study on medical students and explores correlations between Emotional Intelligence and selection scores at the University of Western Australia. In this research consist of 177 respondents of senior medical students from a 6-year undergraduate curriculum. The result shows that Males had higher Emotional Intelligence scores than females and Asian students demonstrated higher Emotional Intelligence Total and branch scores than White students. The highest and lowest Emotional Intelligence scores were obtained for the branches Understanding and Perceiving Emotions respectively. No significant correlations were found between Emotional Intelligence Total.
Weng [26] conducted an observational study to determine the inter-relationships among emotional intelligence (EI), patient satisfaction, and doctor burnout and job satisfaction. They used a positive perspective and multi-source data collection. This study consists of 110 internists and 2872 out-patients were surveyed in face-to-face interviews. In this research the results showed that higher self-rated Emotional Intelligence was significantly associated with less burnout and higher job satisfaction. Higher patient satisfaction was correlated with less burnout. Less burnout was found to be associated with higher job satisfaction. The result concluded that Emotional Intelligence as a factor in understanding doctor’s work-related issues.
Weng [43] conducted a study to determine the associations of surgeon’s emotional intelligence and surgeon’s empathy with patient-surgeon relationships, patient perceptions of their health, and patient satisfaction before and after surgical procedures. In this research they used multi-source approaches to survey 50 surgeons and their 549 outpatients during initial and follow-up visits. The result showed that Surgeon’s emotional intelligence had a positive effect on patient-rated patient-surgeon relationships. Patient-surgeon relationships had a positive impact on patient satisfaction before surgery. Surgeon empathy did not have an effect on patient-surgeon relationships or patient satisfaction prior to surgery. But after surgery, surgeon empathy appeared to have a significantly positive and indirect effect on patient satisfaction through the mediating effect of patient’s self-reported health status. This study showed that long-term patient satisfaction with their surgeons is affected less by emotional intelligence than by empathy.
Hariharan conducted a study attempts to measure the emotional intelligence of doctors. The research consisted of 50 senior doctors and 45 Post Graduate Medical Students (PGMS) working in the Government sector. There was used administered Hyde’s scale of emotional intelligence (2002). Difference in emotional intelligence (EI) between the senior doctors and Post Graduate Medical Students was worked out using ‘t’ test. The Results revealed a significant difference in eight out of ten dimensions. Inferences are drawn as probable causes. Measures for enhancing emotional intelligence among medical professionals are discussed.
Psilopanagioti [44] conducted a study which was aimed to find the relationships, direct or indirect between emotional intelligence, the surface acting component of emotional labor and job satisfaction in medical staff working in tertiary healthcare. The research consists of 130 physicians collected from Greece, who completed a series of self- report questionnaires. The Results showed that Emotional intelligence (Use of Emotion dimension) was significantly and positively correlated with job satisfaction.
Morales [45] conducted a literature review which was aimed to evaluate the relationship between physician emotional intelligence and quality of care. This literature review determined three domains which are impact on physician-patient interaction, impact on staff, and direct impact on physician. Each of these domains is broad categories where there is a strong proven relationship with physician emotional intelligence. The concluded result of this research was all three domains are strongly connected to each other and throughout the literature review common themes began to develop across the domains such as trust, communication, and job satisfaction. Understanding the impact of physician emotional intelligence on all of these domains is fundamental to better understanding the importance of developing and continuously improving emotional intelligence in areas such as healthcare.
Hutchinson [46] conducted Qualitative phase of a larger mixed -method study to explore clinical nurses’ experiences of utilizing emotional intelligence capabilities during clinical reasoning and decision making. In this research 12 nurses were taken. The research study showed in three themes, the sensibility to engage Emotional intelligence capabilities in clinical contexts, motivation to actively engage with emotions in clinical decision making and incorporating emotional and technical perspectives in decision-making.
Malik conducted a descriptive cross-sectional study which was aimed to determine perceived emotional intelligence and its relationship with work life balance and job satisfaction among the healthcare professionals in twin cities of Pakistan. The study used two different pre validated tools, the impact of work life balance factors on job satisfaction questionnaire and the NHS emotional intelligence questionnaire. In this study were selected sample of 283 prescribers, 214 nurses, and 215 pharmacists. The results showed that Job satisfaction had a statistically significant linear weak negative correlation with self-awareness, emotion management, empathy, social skills and motivation and work life balance had a statistically significant very weak negative correlation with emotion management, empathy and motivation. The results of the study concluded that a significant relationship existed among the emotional intelligence, work life balance and job satisfaction. The emotionally intelligent healthcare professionals were better in managing their work life balance and were more satisfied with their job. Pharmacists possessed better social skills with higher motivation levels while physicians were better in managing work life balance than all the other healthcare professionals in Pakistan.
Studies related on Resilience
Hart [47] conducted on nurses. The aim was to describe nursing research there were conducted to understand the phenomenon of resilience in nurses. A comprehensive search was undertaken for nursing research conducted between 1990 and 2011. Key search terms were nurse, resilience, resiliency and resilient. Whittemore and Knafl's integrative approach was used to conduct the methodological review. This study showed this review provides information about the concept of resilience. Becoming aware of contributing factors to the need for resilience and successful strategies to build resilience can help in recruiting and retaining nurses.
Waddimba [48] conducted a study which was aimed to investigate the factors associated with resilience among medical professionals. The study was done using cross-sectional design which was engaged to collect data by structured self-administered questionnaire from 308 respondents from a rural health care network. The conclusion drawn from the results showed that more resilient practitioners experienced frequent satisfaction, relational needs gratification, better uncertainty tolerance, lighter workloads, and practiced on units with more colleagues.
Waddimba [48] conducted a cross‐sectional questionnaire survey to measure Resilience among Employed Physicians and Mid‐Level Practitioners in Upstate New York. The aim of the study was to investigate the factors associated with resilience among medical professionals. In this study found that Relational needs, uncertainty intolerance, satisfaction 75percent of the time, number of practitioners on a unit, and workload were significantly associated with resilience. Higher scores were most strongly associated with uncertainty tolerance, satisfaction, and practitioner numbers. Practitioner/unit demographics were mostly non-significant. So that more resilient practitioners experienced frequent satisfaction, relational needs gratification, better uncertainty tolerance, lighter workloads, and practiced on units with more colleagues. Further studies should investigate well‐being interventions based on these mutable factors.
Ng [49] conducted a study which was aimed to explore the relationship between trainee resilience and intra operative stress. The research was done using confirmatory factor analysis which was engaged to collect data of 171 responses were received and assessed using the 10-item Connor-Davidson Resiliency Scale. The study results showed that Trainees with higher stress or lower resilience were more likely to have considered leaving residency. Increasing resilience correlated with lower intra operative stress.
Imani [50] conducted a phenomenological study to explore Iranian hospital nurses’ lived experiences of intelligent resilience. This study was based on the Husserlian descriptive phenomenology. A purposive sample of ten hospital nurses was drawn from hospitals affiliated with Hamadan University of Medical Sciences, Hamadan, Iran. The result showed that the participating hospital nurses’ lived experiences of intelligent resilience came into four main themes of patience and wisdom, reverence, situational self‐control and appealing to religiosity. Each of the four main themes included two subthemes which were having peace and wise quietness, reverence for the patients, physicians and nurses, distancing themselves from stressful situations and displacing staff who cause stress, and the nurse's trust in God as well as the patient and his family`s trust in God, respectively. So that it concluded as Nurses with intelligent resilience are able to bring peace, reverence for others and situational self‐ control to stressors thereby providing higher quality of care to their patients.
Lebares [51] conducted a study on Burnout among physicians affects mental health, performance, and patient outcomes. They examined burnout and the psychological characteristics that can contribute to burnout vulnerability and resilience in a group of surgical trainees. In this survey 566 surgical residents who participated. Burnout was assessed with an abbreviated Maslach Burnout Inventory. Stress, anxiety, depression, resilience, mindfulness, and alcohol use were assessed and analyzed for prevalence. The result showed that trainees with burnout and high stress were at increased risk for depression and suicidal ideation. Higher dispositional mindfulness was associated with lower risk of burnout, severe stress, and distress symptoms, supporting the potential of mindfulness training to promote resilience during surgery residency.
O'Dowd [52] conducted a study which was aimed to contribute to knowledge regarding how physicians define resilience, the challenges posed by workplace stressors, and strategies which enable physicians to cope with these stressors. In this research a qualitative approach was adopted with 68 semi-structured interviews conducted with Irish physicians. Data were analyzed using deductive content-analysis. The result showed in five themes emerged from the interviews. The first theme, ‘The Nature of Resilience’ captured participants understanding of resilience. Many of the participants considered resilience to be “coping” rather than “thriving” in instances of adversity. The second theme was ‘Challenges of the Profession’ as participants described workplace stressors. The third theme ‘Job-related Gratification’ captured aspects of the workplace that support resilience. ‘Resilience Strategies’ summarized coping behaviors that participants considered to be beneficial to their wellbeing including spending time with family and friends and the final theme ‘Resilience Strategies (Attitudes)’ captured attitudes which protected against stress and burnout.
Vranceanu [53] conducted a study to characterize resiliency and burnout among health care professionals in the neurosciences critical care unit (NCCU) at a tertiary care center. The final analysis included 65 participants Median emotional exhaustion, depersonalization, and personal accomplishment scores were followed. The study result showed that a significant minority of participants reported high levels of emotional exhaustion and depersonalization, with those working longer in the NCCU more likely to experience emotional exhaustion.
McKinley [54] conducted a study which aimed to the existing literature on influences on resilience levels of medical doctors. A narrative synthesis was performed. The following influences on resilience in doctors were identified the demographics, personality factors, organizational or environmental factors, social support, leisure activities, overcoming previous adversity and interventions to improve resilience. The result showed that Resilience is not limited to a doctor’s own personal resource.
Shakir [55] conducted a study to determine the relationship among burnout, grit, and resilience. They surveyed U.S. neurosurgical residents to perform a discretional analysis of prevalence of burnout. Multivariate analysis was performed to determine which variables were associated with higher and lower levels of emotional exhaustion (EE), depersonalization (DP), personal accomplishment (PA), burnout, grit, and resilience. The result showed that there were positive correlations between EE and DP and among PA, grit, and resilience. There were negative correlations for EE and DP with PA, grit, and resilience and between grit/resilience and burnout. There is an inverse relationship between grit/resilience and burnout.
Studies related on surgeons
Buchler [56] conducted a research about leadership characteristics and business management in modern academic surgery. This research focused on practical aspects of surgical management, leadership and training. This explains how the implementation of business management concepts changes workflow management and surgical training. The result of this research concluded that Changes in surgery occur with unprecedented speed because of a growing demand for surgical procedures with limited financial resources. Modern leadership and management theories have to be tailored to surgery. In business management, common traits of successful leaders include team orientation and communication skills. So, the need for surgeons with advanced skills in business, finance and organizational management is evident and will require systematic and tailored training.
Arora [57] conducted a study which was aimed to explore the relationship between trait emotional intelligence (EI) and objective and subjective measures of stress in medical students faced with unfamiliar surgical tasks. In this research 17 medical undergraduates completed an unfamiliar laparoscopic task on a simulator during January to April 2008. Subjective stress before, during and after the task was measured using the self- report State-Trait Anxiety Inventory. Objective stress was measured using continuous heart rate (HR) monitoring. The results showed that highest levels of subjective stress were reported during the task and correlated positively with trait Emotional Intelligence as well as with the trait Emotional Intelligence factors of well-being and emotionality. The research concluded that Students with higher trait EI are more likely to experience stress during unfamiliar surgical scenarios but are also more likely to recover better compared with their lower-trait-Emotional Intelligence peers.
Seyedfatemi [58] conducted a cross-sectional study which was aimed to determine the relationship between the perceived stress with resilience in undergraduate nursing students. The research consists of 309 undergraduate nursing students of Tehran University of Medical Sciences. The research Findings revealed that most of the students (99.3%) had a moderate or high perceived stress. There was a statistically significant relationship between the perceived stress with the resilience.
Stobbs conducted a study which was aimed understand what emotional intelligence is and assess what evidence is available for reviewing surgeon’s emotional intelligence. The result showed that modern-day surgeons do have emotional intelligence, and have equal emotional intelligence capabilities when compared with other specialties, and better skills compared with the general population. This concept is now filtering through into education and training, with a greater importance being placed on it, especially now it is included in professional guidance and literature.
Lebares [51] conducted a study to test the feasibility and acceptability of modified Mindfulness-Based Stress Reduction (MBSR) training during surgical residency. The study conducted with 21 surgical interns in a residency training program at a tertiary academic medical center. The result showed that Local and national surveys demonstrate 2 to 5 times higher burnout, stress, and distress symptoms in surgery residents than in the general population. Focus group discussion revealed a perceived need for stress-resilience training during surgical residency. Content analysis of quotations revealed recurrent themes of anger as a culturally encouraged coping strategy, the experience of highly distressing affective and behavioral changes, and an early experience of disillusionment in the absence of adequate coping skills.
Lindeman [59] conducted longitudinal cohort study to find the Association of Burnout with Emotional Intelligence and Personality in Surgical Residents. The survey completed by 143 general surgery residents from Tertiary academic medical centers in the Northeast. The research result showed that severe burnout was observed in 51% of residents. Higher scores were associated with female sex. Burnout scores were highest at the beginning and end of the academic year Emotional Intelligence and personality scores remained stable. The research concluded that surgical residents have high levels of burnout. Higher EI and positive work experiences are associated with lower burnout.
Beierle [60] conducting a prospective study to Explore Variations in Surgical Resident Emotional Intelligence and Burnout. The study used general surgeon residents were performed via self-report assessment. In this study All general surgery residents PGY1 to PGY5 including preliminary residents were given the assessment tools and the option of participating. The result showed that Improvements in burnout and Emotional Intelligence scores were seen across 3 administrations of surveys without any intervention.
Summary of Review of literature
The review of literature suggests that there are more studies on perceived stress, Emotional intelligence and Resilience among surgeons. The study by Shakir [55] the result showed inverse relationship between Resilience and burnout. The study by Seyedfatemi [58] the result indicated that there was a statistically significant relationship between Perceived stress and Resilience. A study by Weng [26] the results showed Emotional intelligence had a positive effect on patient-surgeon relationship. A study by Ng [49] the results indicated that in trainees higher the stress level, lower Resilience. There is study by Pau [35] that low emotional intelligence scores report more Perceived stress. Another study by Green [31] indicates surgeons showed significantly higher Stress than general population. Majority of the studies by Shakir [55], Seyedfatemi [58], Weng [26], Ng [49], Pau [35] and Green [31] have revealed that there is a significant relationship between Perceived stress, Emotional intelligence and Resilience. While social norms may slowly change across the industry gender stereotypes still manifest sometimes, prominently among females. One thing to lack in progression is because females cut back professionally to accommodate personal responsibilities. So, the present study is finding out to underline the difference in male and female surgeons on Perceived stress, Emotional intelligence and Resilience which can motivate students who are interested in pursuing the field of surgery and back off from the field with an assumption that gender could be a barrier.
Need for the study
Physicians pursue the arduous task of becoming surgeons to vary the lives of people facing serious health problems, to experience bliss of facilitating healing, and to assist support those patients for whom medicine doesn't yet have curative treatments. It is believed that surgeons have big pockets and a bigger ego. This is a myth. They are the first to back off if they have made a mistake and immediately rectify. Despite its virtues, a career in surgery brings significant challenges which will cause substantial personal distress for the individual surgeon and his or her family. So, the rationale of the study is to give awareness to budding surgeons in a such male dominated field of medical science to map a career pathway that integrates personal and professional goals with the result of maintaining their stress, professionalism and to rebound quickly without being permanently injured throughout his or her professional career.
METHOD
The research aims to find out the level of Perceived stress, Emotional Intelligence and Resilience among Surgeons. This Chapter consists of research questions, aim, objectives, research design, participants, sampling and sample selection criteria, procedure, tools and nature of the tools and the statistical analysis used in the study.
Objectives
- To find out if there is any significant gender difference in the level of Perceived stress, Resilience and Emotional intelligence among
- To find out the relationship between Perceived stress, Resilience and Emotional intelligence among
Research Problems
- Is there any significant gender difference in the level of Perceived stress among surgeons?
- Is there any significant gender difference in the level of Emotional intelligence among surgeons?
- Is there any gender significant difference in the level of Resilience among surgeons?
- Is there any significant relationship between Perceived stress and Emotional intelligence among surgeons?
- Is there any significant relationship between Emotional intelligence and Resilience among surgeons?
- Is there any significant relationship between Perceived stress and Resilience among surgeons?
Aim
To study the level of Perceived Stress, Emotional Intelligence and Resilience among Surgeons.
Variables
Independent variable:
- Gender-Male; Surgeon: female surgeon
Dependent Variables:
- Perceived stress, Emotional intelligence and
OPERATIONAL DEFINITIONS
Perceived stress
It is the feelings or thoughts that an individual has about how much stress they are under at a given point in time or over a given time of period. It is the degree to which situations in one’s life are appraised a s stressful.
Emotional intelligence
Emotional intelligence a cluster of traits or abilities relating to the motional side of life- abilities such as recognizing and managing one’s own emotions, being able to motivate oneself and restrain one’s impulse, recognizing and managing others emotions and handling interpersonal relationship in an effective manner [25].
Resilience
Resilience can be described as quality that allows an individual or group to function well despite the odds against them.
Surgeons
A surgeon is a physician who performs surgical operations. The surgeons establish the diagnosis and provide the preoperative care to patients and post-operative care to patients and are often responsible for the comprehensive management of trauma victim and the critically ill patient [2].
Hypotheses
- Ho1- There is no significant gender difference in the level Perceived stress among
- Ho2- There is no significant gender difference in the level of Emotional intelligenceamong
- Ho3- There is no significant gender difference in the level of Resilience among
- Ho4- There is no significant relationship between Perceived stress and Emotionalintelligence among
- Ho5- There is no significant relationship between Emotional intelligence and Resilienceamong
- Ho6- There is no significant relationship between Perceived stress and Resilienceamong
Research design
Exploratory in nature and sample survey research design will be adopted.
Sample
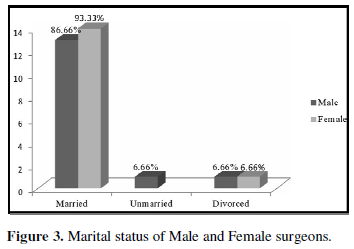
Sampling method adopted for the research was purposive sampling and data was collected from the state of Kerala. The Sample size was 30, with 15 female and 15 male surgeons (Table 1).
Inclusion criteria
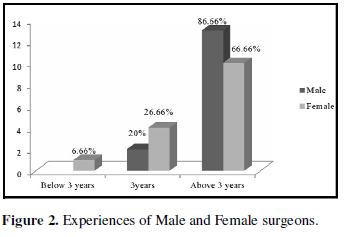
- Surgeons have an experience of minimum 3 years and above.
- Couples who are into different Profession.
Exclusion criteria
- Pathologist
- Individuals who are Unmarried, widower and widow.
Assessment Tools
Personal Data Sheet
The personal datasheet was prepared by the researcher. The data sheet contains Socio- demographic details like Name, Age, gender, place, work experience and marital status etc.
- Perceived stress scale
The perceived stress scale (PSS) was developed by Cohen [12]. The scale is reprinted with permission of the American sociological Association, from Cohen [12]. A global measure of perceived stress.
Scoring key
Perceived stress scores obtained by reversing responses (e.g., 0=4, 1=3, 2=2, 3=1&4=0) to the four positively stated items (items 4, 5, 7&8) and then summing across all scale items. A short 4 item scale can be made from questions 2, 4, 5 and 10 of the perceived stress 10 item scales. It is a measure of the degree to which situation in one’s life are appraised as stressful. Items were designed to tap how unpredictable, uncontrollable and overloaded respondents find their life. The scale also includes a number of direct queries about current levels of experienced stress. The perceived stress scale was designed for use in community samples with at least a junior high school education. The questions in the perceived stress scale ask about feelings and thoughts during the last month. In each case, respondents are asked how often they felt a certain way.
Evidence for validity: higher PSS scores were associated with
- Failure to quit
- Failure among diabetics to control blood sugars
- Greater vulnerability to stressful life-event-elicited depressive
Reliability
A Cronbach’s Alphas coefficient of 0.72 was obtained.
- The 14-item Resilience scale (RS-14)
Resilience scale was developed by Abiola and Udofia [61], Department of Psychiatry, Aminu Kano Teaching Hospital, Kano, Nigeria in the year 2011.
Scoring key
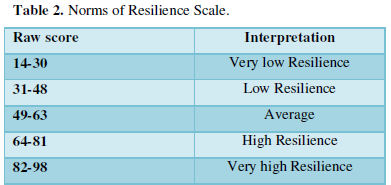
To score the 14-item resilience scale add up the scores of all the items to obtain the total score. The score should range from 14-98 with a neutral score of 56 (Table 2).
Reliability
The internal consistency reliability score was found to be 0.91 and Cronbach’s alpha is found to be 0. 90.
- Emotional intelligence Scale
Hyde [62] developed such a tool called Emotional intelligence Scale (EIS) for measuring emotional intelligence behavior which covers self-awareness, empathy, self- motivation, emotional stability, managing relations, integrity, self-development, value orientation etc.
Scoring
Emotional intelligence scale contains 34 statements, each to be rated on a five-point scale ranging from ‘strongly agree’ (5) to ‘strongly disagree’ (1). The statements relate different components of emotional intelligence like self-awareness (4items), empathy (5items), self-motivation (6items), emotional stability (4items), managing relations (4items), integrity (3items), self-development (2items), commitment (2items), and altruistic behavior (2items). The obtainable score ranges from 34 to 170 where higher score indicates higher level of emotional intelligence. There are no negative items. Individual subscales scores are obtained by summing the scores belonging to a particular Subscales. Validity: the scale has high adequate content validity.
Reliability
The split-half reliability of the scale is 0.88.
Procedure
The Purpose of the study was explained to the participants. The participant’s willingness to participate in the study was ascertained after the establishment of rapport. The socio- demographic details were collected. The participants were briefed about both the inventories separately and were provided with clear instructions. After the completion of administration of the Perceived stress, emotional intelligence Scale, resilience Scale were administered, both the inventories were collected and checked for any kind of omissions. Then the scoring was done for the responses obtained and interpretations were made. The questionnaires were given to the participants through Google Forms, making them clear with the intention of the study.
Ethical issues
- Research is taken only after approving from the department of
- Confidentiality was maintained throughout the
- Data collected is used only for research
- Informed consent was taken from the participants before collecting the
Statistical Analysis
Descriptive statistics
- Mean
- Standard deviation
Inferential statistics
Here using Independent samples t-test and Karl Pearson’s Co-efficient of Correlation.
- The independent samples t-test were used to understand the significant gender difference in the level of Perceived stress, Emotional intelligence and Resilience among surgeons (H01, H02 and H03 are analyzed to using independent samples t-test).
- Karl Pearson’s Co-efficient of Correlation will be used to understand the significant relationship between Perceived stress, Emotional intelligence and Resilience among Surgeons (H04, H05 and H06 are analyzed to using Karl Pearson’s Co-efficient ofCorrelation).
RESULTS AND DISCUSSION
The objective of the present research was to study the level of Perceived stress, Emotional Intelligence and Resilience among Surgeons. This chapter consists of the data relevant to the test hypotheses and Interpretation of the results. The results obtained were analyzed using Independent samples t-test and Karl Pearson’s Co-efficient of Correlation. The independent samples t-test was used to understand the significant difference in the level of Perceived stress, Emotional Intelligence and Resilience among Surgeons. The Coefficient of Correlation between Perceived stress, Resilience and Emotional Intelligence was obtained through Karl Pearson’s Co-efficient of Correlation.
Section 1: Socio-demographic details of the participants
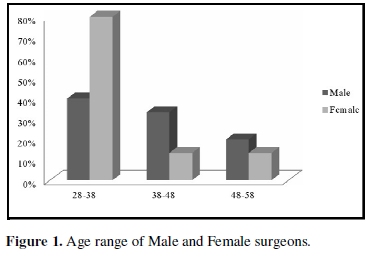
The age of surgeons indicates that 40% of the male participants and 80% of the female participants falls under the age range of 28-38 and 33.33%of male participants and 13.33% of the female participants falls under age range of 38-48 and 20% of the male participants and 13.33%of the female participants falls under the age range of 48-58 (Figure 1).
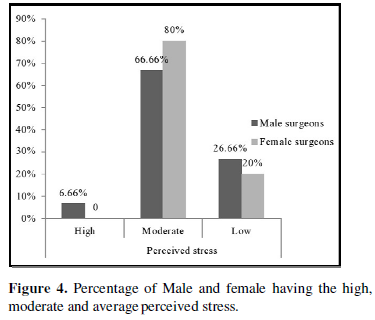
Level of Perceived Stress
Percentage of male and female Surgeons having high, moderate and low level of Perceived stress indicates that 6.66% of male Surgeons and no female surgeons have high level of Perceived stress; 66.66% of male surgeons and 80% of Female surgeons have average level of Perceived stress.26.66% Male Surgeons and 20% female Surgeons have low level of Perceived stress. It indicates that Males have more level of Perceived stress as compared with that female (Figure 4).
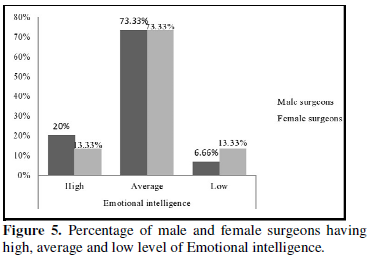
Level of Emotional Intelligence
Percentage of male and female surgeons having high, average and low level of Emotional Intelligence indicates 20% male surgeons and 13.33% of female surgeons have high level of Emotional intelligence. 73.33% of both Male and Female surgeons have average level of emotional intelligence.6.66% male surgeons and 13.33% Female surgeons have low level of emotional intelligence. It indicates that males have more level of emotional intelligence compared with that of females (Figure 5).
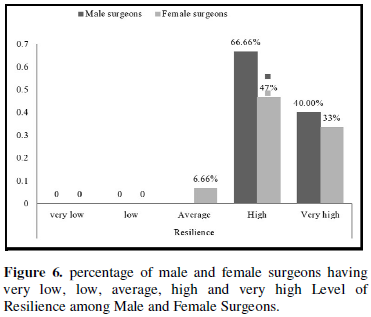
Level of Resilience
The level of Resilience among Male surgeons indicates that 66.66% has high resilience, 40%% has very high and 0% with average, low and very low resilience and female surgeons indicates that 47% has high resilience, 33% has very high, and 6.66% has average and 0% with low and very low resilience. It indicates that male surgeons have more level of Resilience as compared with those female surgeons (Figure 6).
MAIN VARIABLE ANALYSIS
Section 2: Testing of Hypothesis using Independent samples t test.
Independent samples t-test: The independent samples t-test used to know the significant differences in the level of Perceived stress, Emotional intelligence and Resilience among the Surgeons. The hypothesis of Ho1, Ho2 and Ho3 stating that there is no significant gender difference in the level of Perceived stress, Emotional Intelligence and Resilience among Surgeons.
Perceived stress
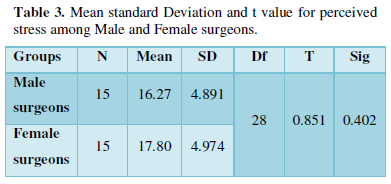
The hypothesis stating that there is no significant difference in the level of Perceived stress among Male and Female Surgeons was tested using independent samples t- test. The obtained t value is 0.851 which is not significant. Thus, the obtained result indicates that there is no significant difference in the level of Perceived stress among Male and Female Surgeons. Hence, the null hypothesis is accepted (Table 3, Figure 7).
Resilience
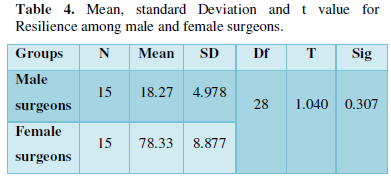
The hypothesis stating that there is no significant difference in the level of Resilience among Male and Female Surgeons was tested using independent sample t- test. The obtained t value is 1.040 which is not significant. Thus, the obtained result indicates that there is no significant difference in the level of Resilience among Male and Female Surgeons. Hence, the null hypothesis stating that there is no significant difference in the level of Resilience among Male and Female surgeons is accepted (Table 4, Figure 8).
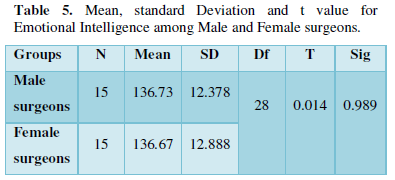
Thus, the obtained result indicates that there is no significant difference in the level of Emotional Intelligence among Male and Female Surgeons. Hence, the null hypothesis stating that there is no significant difference in the level of Emotional Intelligence among Male and Female surgeons is accepted (Table 5, Figure 9).
Section 3: Testing of Karl Pearson’s Co-efficient of Correlation
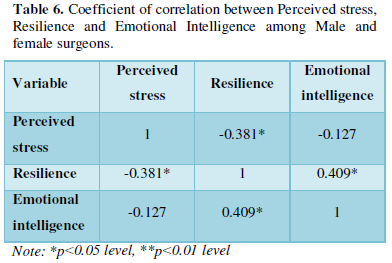
The hypothesis stating that there is no significant relationship between Perceived stress and Emotional Intelligence was tested using Karl Pearson’s Co-efficient of Correlation (Table 6). The findings of the analysis indicate that there is no relationship between Perceived stress and Emotional Intelligence (-0.127) which is not significant. Thus, the result indicates that with the increase in the level of Perceived stress, does not affect the level of Emotional Intelligence. Therefore, the null Hypothesis, Ho4 stating that there is no significant relationship between Perceived stress and Emotional Intelligence is accepted. The research findings are contradictory to what Pau wrote in their research which states that low Emotional Intelligence scorers report more Perceived stress. Likewise, there is another research which is done by Nitin Joseph in his research which states that Perceived Stress scores were found to decrease with increase in Emotional Intelligence scores.
The hypothesis stating that there is no significant relationship between Emotional Intelligence and Resilience was tested using Karl Pearson’s Co-efficient of Correlation. The findings of the analysis indicate that there is a significant relationship between Emotional Intelligence and Resilience (0.409*) which is significant. Thus, the result indicates that with the increase in the level of Emotional Intelligence there increase in the level of Resilience. Therefore, the null Hypothesis, Ho5 stating that there is no significant relationship between Emotional Intelligence and Resilience is rejected and the alternate Hypothesis is accepted which states that there is a significant relationship between Emotional Intelligence and Resilience. The present findings were supported by some of the studies which indicated a positive relation between Emotional Intelligence and Resilience [63].
The hypothesis stating that there is no significant relationship between Perceived stress and Resilience was tested using Karl Pearson’s Co-efficient of Correlation. The findings of the analysis indicate that there is significant negative correlation between Perceived stress and Resilience (r=-0.381*) which is significant negatively. Thus, the result indicates that when the level of Perceived stress increases, there is decrease in the level of Resilience. Therefore, the null Hypothesis, Ho6 stating that there is no significant relationship between Perceived stress and Resilience is rejected and the alternate Hypothesis which states that there is a significant relationship between Perceived stress and Resilience is formed and accepted. The present findings were supported by some of the studies were what Seyedfatemi [58] wrote in their research which states that There is a significant relationship between the perceived stress with the resilience.
SUMMARY AND CONCLUSION
This chapter contains brief summary of the present research work, major findings, conclusions, implication, limitations, and scope for further research.
Summary of the Research
The present study was undertaken to study the level Perceived Stress, Resilience and Emotional Intelligence among Male and Female Surgeons. The Male surgeons and Female Surgeons are the independent variable. Perceived Stress, Resilience and Emotional Intelligence are the dependent variables. The sample included 30 participants, comprising of 15 Male surgeon’s and 15 Female surgeons. The Purposive Sampling Technique was used to collect the data. The Sample Survey Research Design was adopted in the study. The participants who are in the age range of 28-58 years were included in the study. The Male and Female surgeons who had an experience of 3 and more years were included in the study.
The perceived stress scale (PSS) was developed by Cohen [12] was used to assess the level of Perceived stress and Resilience The 14-item Resilience scale (RS-14) developed by Abiola and Udofia [61] was used to assess level of resilience among the participants of the study and Emotional intelligence Scale was developed by Hyde [62] was used to assess the level of emotional intelligence. The obtained results were analyzed using Independent Samples t-test and Karl Pearson’s Co-efficient of Correlation.
FINDINGS OF THE STUDY
The level of Perceived stress, Emotional intelligence and Resilience of the participants were determined.
- Male surgeons had more level of perceived stress compared to those female surgeons.
- Male surgeons had more level of Emotional intelligence compared to those female surgeons.
- Male surgeons had more level of Resilience compared to those female surgeons.
Independent Samples t-test: The Independent Samples t-test was undertaken to know the difference in the Perceived stress, Emotional intelligence and Resilience among Surgeons.
- The obtained result indicates that male and female surgeons do not differ significantly in the level of Perceived stress.
- The obtained result indicated that male and female surgeons do not differ significantly in the level of Emotional Intelligence.
- The obtained result indicates that male and female surgeons do not differ significantly in the level of Resilience.
Karl Pearson’s Co-efficient of Correlation: The relationship between Perceived stress, Emotional intelligence and Resilience among surgeons.
- The result indicates that with the increase in the level of Perceived stress, there is decrease in the level of Resilience.
- The result indicates that with the increase in the level of Emotional intelligence, there is decrease in the level of Perceived stress but it is not significant.
- The result indicates that with the increase in the level of Emotional intelligence, there is increase in the level of Resilience.
CONCLUSION
From the findings of the study, it is clearly evident that there is no significant difference among male and female surgeons. There is a military ethic in surgery that may not be appealing to a woman’s mentality, so the researcher would like to conclude that female surgeons who are already in this profession has comparatively less stress than males, which means it is absolutely flawless for budding surgeons to go for the surgical field if it is their passion, because stress is normal for all the professions and is not based on the gender.it is a strong misconception that females cannot take up some of the professions. The study also reveals that both male and female surgeons do not differ in resilience and emotional intelligence.
LIMITATIONS OF THE STUDY
- The data of the study was collected mainly from the state of Kerala; hence caution has to be exercised while generalizing the findings.
- The Educational qualification of surgeons and the specialization have not been taken into consideration for the study, both of which might have contributed.
- The sample size taken for the study is very small.
IMPLICATION
The result was shown that there is no significant difference in the Perceived stress, Emotional intelligence and Resilience between Male and Female surgeons. A suitable intervention plan can be planned to increase the Emotional intelligence and Resilience among surgeons in hospitals.
SCOPE FOR FURTHER STUDY
- Mixed method analysis can be done so as to get a deeper understanding of the various problems or conditions which affect them.
- The study can be extended using Longitudinal Research.
- World Health Organization (WHO) (2013) Definition and list of health professionals. Accessed on: March 1, 2020. Available online at: https://www.ncbi.nlm.nih.gov/books/NBK298950/
- Sushrutasamhita (2016) Available online at: https://en.wikipedia.org/wiki/Sushruta_Samhita
- Anton NE, Montero PN, Howley LD, Brown C, Stefanidis D (2015) What stress coping strategies are surgeons relying upon during surgery? Am J Surg 210(5): 846-851.
- Papel ID, Frodel J. Facial Plastic and Reconstructive Surgery.
- Singhal GD (1972) Diagnostic considerations in ancient Indian surgery: (based on Nidāna-Sthāna of Suśruta Saṁhitā). Varanasi: Singhal Publications.
- Ahmad Z (2007) Al-Zahrawi - The Father of Surgery. ANZ J Surg 77(1): A83
- Cosman MP, Gale JL (2008) Handbook to Life in the Medieval World. Handbook to Life Series. 2. Infobase Publishing. pp: 528-530.
- Bartram DJ, Yadegarfar G, Baldwin DS (2009) Psychosocial working conditions and work-related stressors among UK veterinary surgeons. Occup Med (Lond) 59(5): 334-341.
- Chan SWW, Cheung PSK, Lee JFY, Fung JTK, Patil NG, et al. (2010) Women surgeons in Hong Kong. Surg Pract 14(1): 2-7.
- Sharma A, Sharp DP, Walker LG, Monson JRT (2008) Stress and burnout among colorectal surgeons and colorectal nurse specialists working in the National Health Service. Colorectal Dis 10(4): 397-406.
- Girgis A, Sanson-Fisher RW, McCarthy WH (1997) Communicating with Patients: Surgeons' Perceptions of their Skills and Need for Training. Aust N Z J Surg 67(11): 775-780.
- Cohen S, Kamarck T, Mermelstein R (1983) A Global Measure of Perceived Stress. J Health Soc Behav 24(4): 385-396.
- Folkman S, Lazarus RS, Gruen RJ, DeLongis A (1986) Appraisal, coping, health status, and psychological symptoms. J Pers Soc Psychol 50(3): 571-279.
- Papp KK, Stoller EP, Sage P, Aikens JE, Owens J, et al. (2004) The Effects of Sleep Loss and Fatigue on Resident-Physicians: A Multi-Institutional, Mixed- Method Study. Acad Med 79(5): 394-406.
- Sami A, Waseem H, Nourah A, Areej A, Afnan A, et al. (2012) Real-time observations of stressful events in the operating room. Saudi J Anaesth 6(2): 136-139.
- Anto MM, Hridya VM, Babu M, Lijo J (2015) Stress profile among maxillofacial surgeons. Int J Res Health Sci 3(1): 150-157.
- Dyrbye LN, Thomas MR, Shanafelt TD (2006) Systematic Review of Depression, Anxiety, and Other Indicators of Psychological Distress Among U.S. and Canadian Medical Students. Acad Med 81(4): 354-373.
- Petrides KV, Pita R, Kokkinaki F (2007) The location of trait emotional intelligence in personality factor space. Br J Psychol 98(2): 273-289.
- Arora S, Ashrafian H, Davis R, Athanasiou T, Darzi A, et al. (2010) Emotional intelligence in medicine: a systematic review through the context of the ACGME competencies. Med Educ 44(8): 749-764.
- Colman A (2008) A Dictionary of Psychology (3 ed.). Oxford University Press.
- Petrides KV, Furnham A (2003) Trait emotional intelligence: Behavioral validation in two studies of emotion recognition and reactivity to mood induction. Eur J Pers 17: 39-75.
- Mayer JD, Salovey P (1997) What is emotional intelligence? In Salovey P, Sluyter D (eds.). Emotional development and emotional intelligence: Implications for educators. New York: Basic Books. pp: 3-31
- Birks YF, Watt IS (2007) Emotional intelligence and patient-centered care. J R Soc Med 100(8): 368-374.
- Austin EJ (2009) A reaction time study of responses to trait and ability emotional intelligence test items. Pers Indiv Differ 46(3): 381-383.
- Goleman D (1998) What Makes a Leader? Harv Bus Rev 76: 92-105.
- Weng HC, Steed JF, Yu SW, Liu YT, Hsu CC, et al. (2011) The effect of surgeon empathy and emotional intelligence on patient satisfaction. Adv Health Sci Educ Theory Pract 16(5): 591-600.
- Hurley K (2020) What Is Resilience? Definition, Types, Building Resiliency, Benefits, and Resources. Everyday Health. Accessed on March 1, 2020. Available online at: https://www.everydayhealth.com/wellness/resilience/#:~:text=Resilience%20is%20the%20ability%20to,%2C%20emotional%20upheaval%2C%20and%20suffering.&text=Resilient%20people%20tap%20into%20their,challenges%20and%20work%20through%20problems.
- Fletcher D, Sarkar M (2013) Psychological resilience: A review and critique of definitions, concepts, and theory. Eur Psychol 18(1): 12-33.
- Ginsburg KR, Jablow MM (2011) Building resilience in children and teens: Giving kids roots and wings (2nd). Elk Grove Village, Illinois: American Academy of Pediatrics.
- King BM, Carr DC, Taylor MG (2019) Depressive Symptoms and the Buffering Effect of Resilience on Widowhood by Gender. Gerontologist 59(6): 1122-1130.
- Green A, Duthie HL, Young HL, Peterst TJ (1990) Stress in surgeons. Br J Surg 77(10): 1154-1158.
- Westerman GH, Grandy TG, Ocanto RA, Erskine CG (1993) Perceived sources of stress in the dental school environment. J Dent Educ 57(3): 225-231.
- Sanders AE, Lushington K (2002) Effect of perceived stress on student performance in dental school. J Dent Educ 66(1): 75-81.
- Radcliffe C, Lester H (2003) Perceived stress during undergraduate medical training: A qualitative study. Med Educ 37(1): 32-38.
- Pau AK, Croucher R (2003) Emotional Intelligence and Perceived Stress in Dental Undergraduates. J Dent Educ 67(9): 1023-1028.
- Maville JA, Tucker BA, Kranz PL (2004) Perceived Stress Reported by Nurse Practitioner Students. J Am Acad Nurse Pract 16(6): 257-262.
- Shah M, Hasan S, Malik S, Sreeramareddy CT (2010) Perceived Stress, Sources and Severity of Stress among medical undergraduates in a Pakistani Medical School. BMC Med Educ 10: 2.
- Abdollahi A, Talib AM, Yaacob SN, Ismail Z (2014) Hardiness as a mediator between perceived stress and happiness in nurses. J Psychiatr Ment Health Nurs 21(9): 789-796.
- Uzun Ö, Sevinç S (2015) The relationship between cultural sensitivity and perceived stress among nurses working with foreign patients. J Clin Nurs 24(23-24): 3400-3408.
- Wagner PJ, Jester DM, Moseley GC (2002) Medical Students as Health Coaches. Acad Med 77(11): 1164-1165.
- Weng HC, Chen HC, Chen HJ, Lu K, Hung SY (2008) Doctors’ emotional intelligence and the patient-doctor relationship. Med Educ 42(7): 703-711.
- Carr SE (2009) Emotional intelligence in medical students: Does it correlate with selection measures? Med Educ 43(11): 1069-1077.
- Weng HC, Hung CM, Liu YT, Cheng YJ, Yen CY, et al. (2011) Associations between emotional intelligence and doctor burnout, job satisfaction and patient satisfaction. Med Educ 45(8): 835-842.
- Psilopanagioti A, Anagnostopoulos F, Mourtou E, Niakas D (2012) Emotional intelligence, emotional labor, and job satisfaction among physicians in Greece. BMC Health Serv Res 12: 463.
- Morales JB (2014) The Relationship between Physician Emotional Intelligence and Quality of Care. Int J Caring Sci 7(3): 704-710.
- Hutchinson M, Hurley J, Kozlowski D, Whitehair L (2017) The use of emotional intelligence capabilities in clinical reasoning and decision-making: A qualitative, exploratory study. J Clin Nurs 27(3-4): e600-e610.
- Hart PL, Brannan JD, De Chesnay M (2014) Resilience in nurses: An integrative review. J Nurs Manag 22(6): 720-734.
- Waddimba AC, Scribani M, Hasbrouck MA, Krupa N, Jenkins P, et al. (2016) Resilience among Employed Physicians and Mid-Level Practitioners in Upstate New York. Health Serv Res 51(5): 1706-1734.
- Ng R (2017) Resiliency in the Operating Room: Exploring Trainee Stress During Surgery and the Role of Individual Resilience. Accessed on: March 1, 2020. Available online at: https://ir.lib.uwo.ca/cgi/viewcontent.cgi?article=6586&context=etd
- Imani B, Kermanshahi SMK, Vanaki Z, Lili AK (2018) Hospital nurses’ lived experiences of intelligent resilience: A phenomenological study. J Clin Nurs 27(9-10): 2031-2040.
- Lebares CC, Guvva EV Ascher NL, O'Sullivan PS, Harris HW, et al. (2018) Burnout and Stress Among US Surgery Residents: Psychological Distress and Resilience. J Am Coll Surg 226(1): 80-90.
- O'Dowd E, O'Connor P, Lydon S, Mongan O, Connolly F, et al. (2018) Stress, coping, and psychological resilience among physicians. BMC Health Serv Res 18(1): 730.
- Vranceanu AM (2019) Burnout and Resiliency Among Neurocritical Care Staff; Potential Solutions to A Growing Problem. Neurocrit Care 31(2): 251-252.
- McKinley N, Karayiannis PN, Convie L, Clarke M, Kirk SJ, et al. (2019) Resilience in medical doctors: A systematic review. Postgrad Med J 95(1121): 140-147.
- Shakir HJ, Cappuzzo JM, Shallwani H, Kwasnicki A, Bullis C, et al. (2020) Relationship of Grit and Resilience to Burnout Among U.S. Neurosurgery Residents. World Neurosurg 134: e224-e236.
- Buchler P, Martin D, Knaebel HP, Buchler MW (2006) Leadership characteristics and business management in modern academic surgery. Langenbecks Arch Surg 391(2): 149-156.
- Arora S, Russ S, Petrides KV, Sirimanna P, Aggarwal R, et al. (2011) Emotional intelligence and stress in medical students performing surgical tasks. Acad Med 86(10): 1311-1317.
- Seyedfatemi N, Pourafzal F, Inanloo M, Haghani H (2015) Percieved-stress and Resilience in Nursing Students. Eur Psychiat 30: 1005.
- Lindeman B, Petrusa E, McKinley S, Hashimoto DA, Gee D, et al. (2018) Corrigendum to “Association of burnout with emotional intelligence and personality in surgical residents: Can we predict who is most at risk?” [J SurgEduc (2017) e22- e30]. J Surg Educ 75(4): 1135-1136.
- Beierle SP, Kirkpatrick BA, Heidel RE, Russ A, Ramshaw B, et al. (2019) Evaluating and Exploring Variations in Surgical Resident Emotional Intelligence and Burnout. J Surg Educ 76(3):628-636.
- Abiola T, Udofia O (2011) Psychometric assessment of the Wagnild and Young's resilience scale in Kano, Nigeria. BMC Res Notes 4: 509.
- Hyde A, Pethe S, Dhar U (2002) Manual for emotional intelligence scale. Lucknow, India: Vedanta Publications.
- Maulding W, Peters GB, Roberts J, Leonard E, Sparkman L (2012) Emotional intelligence and resilience as predictors of leadership in school administrators. J Leaders Stud 5(4): 20-29.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6















QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)


