Research Article
Motivational Interviewing Training for Intimate Partner Violence Intervention Providers: A Quasi Experimental Study
934
Views & Citations10
Likes & Shares
Objective: Client engagement is an essential component in Intimate Partner Violence (IPV) intervention. Engaged clients are more likely to engage with programme facilitators and the intervention itself. Studies show that intervention engagement is low in IPV intervention programmes, which leads to early drop-out from the intervention. Motivational interviewing (MI) may be particularly well suited for violent individuals who are reluctant to attend intervention. However few practitioners in the IPV field receive training in MI, and specifically MI for intervention engagement.
Method: The current study examined the effectiveness of MI training (2-day MI workshop, plus an addition six hours training, followed by individual feedback and coaching) for practitioners (n=10) working in the IPV area.
Results: There was a statistically significant (p < 0.05, r = 0.3) increase in the practitioners’ MI skills post-workshop training (measured by the New Zealand version of the Video Assessment of Simulated Encounters Revised), and that with further training, feedback and coaching, three out of the four practitioners who submitted audio-recordings of their MI practice demonstrated at least a fair level of proficiency in MI (as measured by the Motivational Interviewing Treatment Integrity code 4.2.1).
Conclusion: Given the importance of engagement for IPV intervention programs, it is recommended that IPV intervention providers consider training their staff in MI to increase intervention engagement.
Keywords: Motivational interviewing, Training, Intimate partner violence, Engagement, Intimate partner violence intervention
INTRODUCTION
Studies of the efficacy of Intimate Partner Violence (IPV) intervention have found mixed results and small effects sizes [1, 2]. The most important reason for the small effects of IPV intervention seems to be that on average, 50% of the participants never complete the programme; regardless of whether they are court ordered or not [3]. Furthermore, of particular concern is that those who dropouts are at greater risk of continued IPV [4-6]. Low motivation as a reason for dropout has been identified in a number of studies [2, 7-9]. This highlights the importance of addressing motivation and engagement in IPV interventions.
Motivational Interviewing (MI) is a collaborative conversational style for strengthening a person’s own motivation and commitment to change [10]. It is usually a brief intervention (1-4 sessions) which can be utilised individually or within groups [11]. Motivational Interviewing does not involve telling people either what to do or why to do it, but rather elicits the individual’s own reasons for changes [12].
A large number of controlled trials over more than 35 years have demonstrated the efficacy of MI in helping people to change risky or unhealthy behaviour in a range of settings, including substance abuse and mental treatment, health, and criminal justice settings. Motivational Interviewing has also been found to increase intervention engagement [13, 14], reduce dropout [15], and improve outcomes among clients who are reluctant to attend intervention and/or change their behaviour [16-18].
Motivational Interviewing may also be a practical and effective intervention strategy for treating IPV, increasing IPV intervention engagement, readiness to change, improving session attendance, and intervention compliance [19,20]. Further, it may be particularly appropriate for mandated clients for whom motivation to change may be low as MI has been found to work best for people who are ambivalent about change [21].
Zuckoff, Swartz, and Grote [22] have noted the distinction between MI for intervention engagement and MI for behavior change. They recommended that MI for intervention engagement should include consideration of motivation for changing the behavior under consideration (i.e., changing the risky or unhealthy behavior) and also consideration of additional factors that might influence engagement in intervention as a way of changing the particular behavior.
Motivational Interviewing Training
Over the past 20 years, the need to train professionals in MI has increased [23] as the interest in the application of MI has grown. One of the most important findings from research on MI training is that self-directed learning through reading books and self-reflection is not an effective strategy for learning MI [24]. Instead longer more interactive training, which provides skill-building exercises followed by interactive debriefings, is recommended to develop MI skills [24]. For this reason MI training is often provided in workshops lasting between 2-3 days [5, 23]. These workshops usually include an introduction to the spirit and processes of MI, a demonstration of the method, and opportunities to practice MI skills [23], such as open-ended questions, simple and complex reflection, affirmation, summarizing, and eliciting and responding to change talk.
Studies suggest that although workshop training develops MI skills, newly acquired skills tend to erode soon after training unless there is ongoing post-training feedback and coaching [25-29]. However, while there is strong evidence for extended and multi-component training combined with ongoing coaching and feedback, in reality, trainees and their managers often prefer brief single-session workshop-based training due to time and financial constraints [30].
Despite the challenges for engagement in IPV settings few practitioners in the IPV field receive formal training in MI, and specifically MI for intervention engagement. It is therefore important for research to evaluate what is required to training practitioners working in this area to develop MI skillfulness.
The current study evaluates the effectiveness of MI training for practitioners working in the IPV area. It was hypothesized that participants who received MI training would demonstrate increased skillfulness in MI. The current study was part of a larger study [31] and had ethical approval from the Human Ethics Committee at the University of Canterbury.
METHOD
The Host Organizations
The research was conducted at Aviva Family Violence Services (Aviva for short) and Stopping Violence Services (SVS), which are the two main providers of IPV services in Christchurch, a metropolitan city in New Zealand (NZ). Aviva is a not-for-profit agency supporting NZ families to be free from violence. It started its operation in 1973 as the Christchurch Women’s Refuge. Stopping Violence Services works with men, women, and youth, and provides assessments and non-violence programmes predominantly for the Ministry of Justice, the Department of Corrections, and self-referred clients. Stopping Violence Services has provided non-violence programmes for men and women since 1983 and youth since 2008.
Participants
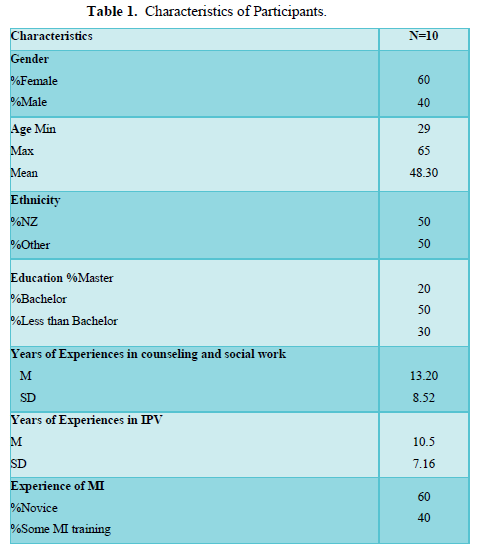
Practitioners at Aviva (n=4) and SVS (n=6) who provided the initial contact with men referred for IPV intervention by the Family Court or the Department of Corrections, and self-referrals were recruited into the study. After meeting with clinical leaders at both agencies, an email containing information about study was sent to practitioners, and those who were interested in participating entered the study voluntarily. Characteristics of the participants are presented in (Table 1). The participants comprised four men and six women, aged 29-65 years (M = 48.30), with a mean of 13.20 (SD = 8.52) years of experience in counseling and social work, and a mean of 10.5 (SD = 7.16) years of experience with IPV specifically. Seven had university-level education (2 at master’s-level and 5 at a bachelor level). Six of the 10 reported having no prior MI training.
Design
The study utilized a quasi-experimental within-groups design to examine the effectiveness of MI training.
Measures
Video Assessment of Simulated Encounters - Revised (VASE-R) NZ
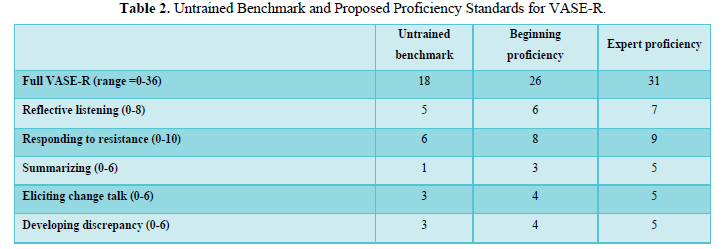
The participants were administered the VASE-R NZ pre- and post-training. Their scores were compared pre- and post-training, with benchmarks for untrained and trained practitioners [32] (Table 2). The VASE-R NZ [33] is a NZ version of the VASE-R. This version is essentially the same as VASE-R, except the wording is consistent with the language used in NZ context, and the use of NZ actors with NZ accents.
The VASE-R NZ was coded by the first author after training in the scale by the second author (a member of the Motivational Interviewing Network of Trainers - MINT). The training involved each person independently rating VASE-R NZ practice examples, and any differences in scores were discussed. This involved coding three samples of VASE-R NZ and the inter-rater reliability (percent agreement) was 80%.
The VASE-R is helpful for researchers to determine an individual’s MI skills and to ascertain if priori skill targets were met before permitting an MI practitioner to begin providing MI for an intervention trial. Subscales can also discriminate between areas of skill and areas in need of further work [32]. The inter-rater reliability and internal consistency, along with concurrent validity of VASE-R have been tested and established [32], [34], [35] with excellent inter-rater reliability (intra-class correlations) for the full-scale score (0.85) and acceptable levels for the subscales (0.44 to 0.73) [32].
While the VASE-R has demonstrated sensitivity to the effects of training [32, 36, 37], it cannot measure actual in session MI behavior. Therefore, a more comprehensive approach for assessing MI skills is required to review and score MI encounters [32]. For this purpose, the most commonly used measurement is the Motivational Interviewing Treatment Integrity rating system, of which the latest version, the MITI 4.2.1 [38], was used in the current study.
Motivational Interviewing Treatment Integrity (MITI) 4.2.1
Participants were asked to submit two audio-recordings of MI sessions with their clients post-training and each recording was coded by the second author using the MITI 4.2.1. While the reliability of this coding was not established for the current study, the second author regularly double codes the MITI 4.2.1 with another member of MINT with high reliability. Written feedback on the results of the coding and areas to work on were provided individually to each participant to further facilitate MI skill development post-workshop training.
The inter-rater reliability for all items in the MITI is in the good to excellent range (0.65 to 0.98) [39]. Also, summary scores (Table 3) from the MITI have correlated with client outcomes in the expected direction [39-41].
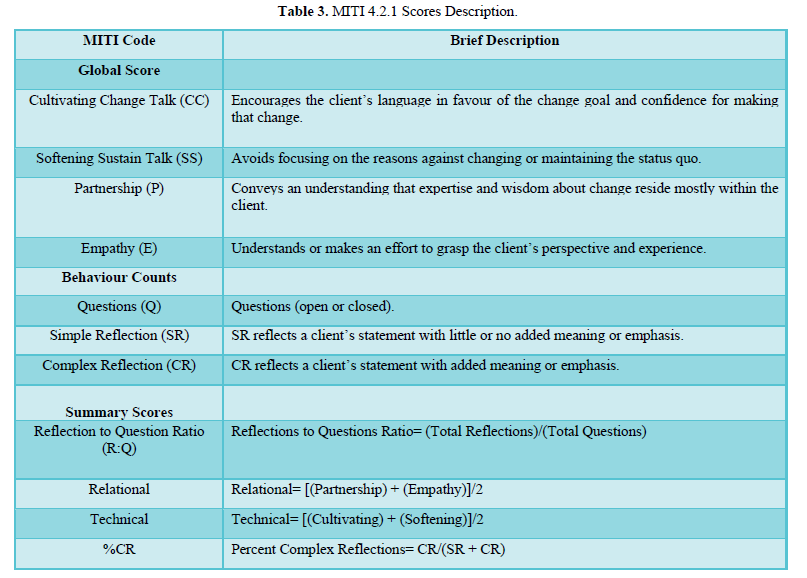
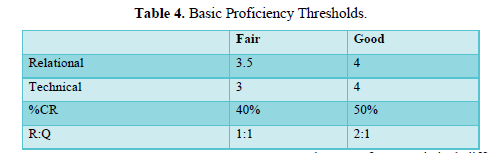
Coding the MITI 4.2.1 involves global ratings of the technical component (cultivating change talk and softening sustain talk), and the relational component (partnership and empathy) of MI (Table 3). Cultivating change talk measures the client’s own language in favor of, and confidence in, making that change. Softening sustain talk measures avoidance of focusing on the reasons against changing or on maintaining the status quo. Partnership conveys that expertise and wisdom about change resides mostly within the client. Empathy involves the practitioner understanding or making an effort in grasping the client’s perspective and experience. The MITI 4.2.1 also includes behavior counts of giving information, questions, simple reflections, complex reflections, affirmations, seeking collaboration, and emphasizing autonomy (MI-consistent behaviors), and confront, persuade, and persuade with permission (MI-inconsistent behaviors). Each global scale is measured on a 5-point Likert scale, while behavior counts are tallied for each occurrence of MI specified behaviors and summary scores are generated (Table 3). The MITI 4.2.1 proposes two levels of proficiency in MI - “fair” and “good” (Table 4).
Procedure
A 2-day (7 hours per day) MI training workshop was facilitated by the second author. In preparation for the workshop, the participants were asked to complete an online training(http://learning.bmj.com/learning/module-intro/.html?moduleId=10051582) and to read an article (10 Things that MI is Not) [42]. The aim of the workshop was for participants to learn the basic style of MI and how to continue learning it in practice. The workshop comprised video-recorded demonstrations, didactic teaching, modelling, and skills practice with feedback. The first day comprised a broad overview of MI, including the spirit of MI, the four processes, the core skills and how these are used across the four processes, and the concepts of change talk, sustain talk, ambivalence, resistance, as well as research evidence on MI efficacy. The focus of the second day was to practice and enhance MI skills, with a focus on building the participants’ skills of evoking and strengthening change talk.
In addition to the workshop, three further MI training sessions (each for 2 hours) were provided starting one month after the 2-day workshop over a 2-month period, which were attended by three participants from SVS. One of these participants had completed the workshop training, another had attended only half a day for each day of the 2-day workshop, and the third one had not participated in the workshop, and had stated that she had received MI training in the past and was keen to increase her skills in MI, however had not been available to attend the 2-day workshop. This practitioner was 65 years old, had a master's degree, and had 12 years of experience in the IPV area.
In these MI refresher sessions, specific problems and challenges in applying MI were identified by the trainer from the review of their audio-recordings. These sessions comprised skills practice and feedback on the technical component of MI, with a focus on evoking and strengthening change talk. The participants from Aviva reported that they did not need the MI refresher sessions, as they had continued to practice MI together within their workplace post the workshop training.
Analysis
Data were analyzed using the SPSS statistical software package version 24. Wilcoxon Signed-Rank test, which is the non-parametrical equivalent of the paired-sample t-test, was used to test for a statistical difference in the VASE-R NZ scores pre- and post-training. Descriptive statistics were used to report the means and standard deviations for global score and behavior counts in MITI 4.2.1. In addition to the confidence intervals and p-values, effect size were also reported for significant results [43].
RESULTS
Video Assessment of Simulated Encounters-Revised NZ
The VASE-R NZ was completed pre- and post-training by seven out of the 10 participants who attended the workshop. The other three participants did not complete the VASE-R NZ as they were not given dedicated time to attend the training and so were absent when the VASE-R was completed. The inter-rater agreement was 77%, which is considered good [44].
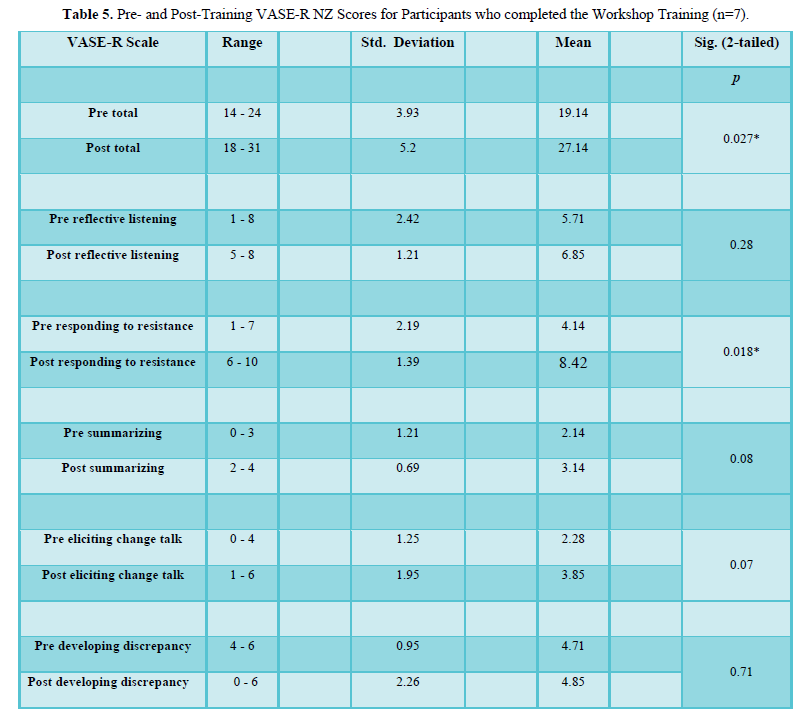
The range, standard deviation, mean, and p-value for the VASE-R-NZ full scale and its subscales pre- and post-training are provided in (Table 5). The participants’ full score on the VASE-R-NZ showed a statistically significant (p < 0.02) increase from pre- (19.14) to post-training (27.14). This result was also associated with a medium effect size (r = 0.3). However, only the responding to resistance (p < 0.018) showed a statically significant increase from pre- (4.14) to post-training (8.42), which was associated with a medium effect size (r = 0.33).
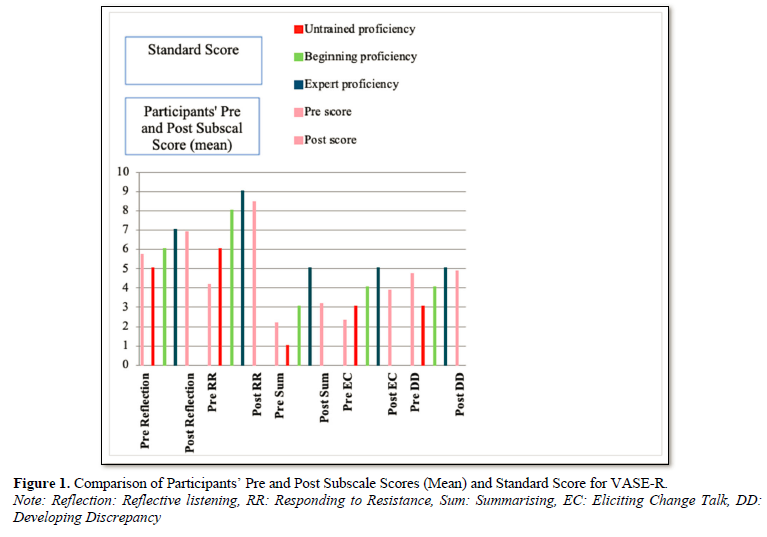
With regards to the full-score, most (n = 5, 71.4%) of the participants were at an untrained benchmark pre-training, with the remaining two at the beginning proficiency level. After the workshop, only one participant was still at the untrained benchmark. Two were at the beginning proficiency level, and the majority (n = 4) had reached an expert proficiency level. The comparison of VASE-R subscale scores pre- and post-training (mean) for these participants with the standard score is presented in (Figure 1).
Motivational Interviewing Treatment Integrity 4.2.1
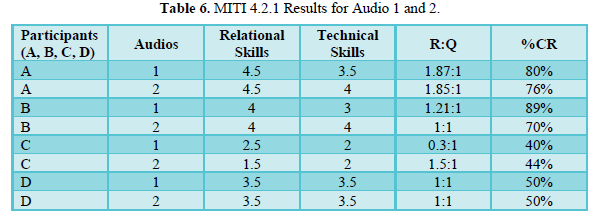
Out of the seven participants who completed the workshop, two from Aviva submitted audio-recordings. From the three participants at SVS who attended the post-workshop training, two also submitted audio recordings (in total, n= audio recordings for MITI4.21. coding.). The reasons given for not submitting audio-recordings by the rest of the participants were heavy workload, the difficulty of using the audio-recording technology, and not feeling confident enough in using MI. The participants’ MITI ratings are presented in (Table 6).
Three of the four participants demonstrated a fair level of proficiency in their first audio for technical skills, and one participant did not reach proficiency. For the second audio, half (n=2) reached a good level of proficiency, and one had a fair level of proficiency. However, still, one participant (the same participant previously mentioned) did not meet proficiency. This suggests that this participant was not able to attend to the technical aspect of MI (evoking and strengthening change talk). For the relational skills, half (n=2) of the participants reached a good level of proficiency in both audios, suggesting that they were demonstrating the spirit of MI. However, for both audios, the same participant as mentioned above did not reach a fair level of proficiency.
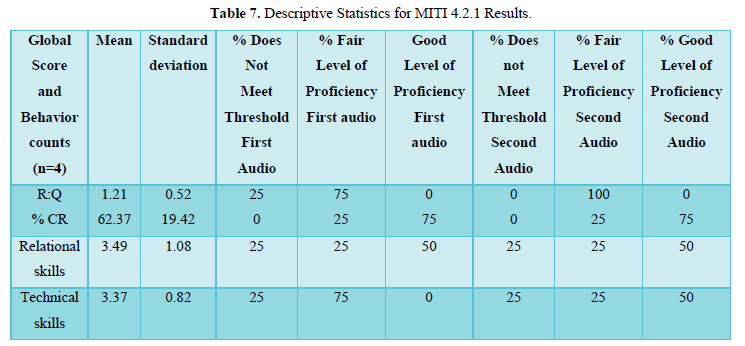
For the MI behavior counts (Table 7), the mean R-Q ratio was 1.21 (SD = 0.52), which is at the fair level of proficiency. Three out of four participants in their first audio and all four participants in their second audio reached a fair level of proficiency for the R-Q, which suggests that they were able to reflect at least as much as they asked questions. The mean score for the %CR was 62.37 (SD = 19.42), which met the criteria for a good level of proficiency in MI. A total of three out of four participants reached a good level of proficiency in the %CR in their first audio, which remained unchanged for the second audio. This suggests that the majority of reflections made were complex, demonstrating a deeper understanding of what their clients were saying. The mean score for the relational and technical skills was 3.49 (SD = 1.08), and 3.37 (SD = 0.82) respectively, which suggests a fair level of proficiency.
In summary, the MITI 4.2.1 ratings of the audio-recordings suggested that all participants who submitted audio-recordings, except one, demonstrated at least a fair level of proficiency in MI after training. Further, there was evidence of increased MI skill after receiving feedback (from Audio 1 to 2) in cultivating change talk (the technical aspect of MI) for two participants.
DISCUSSION
The results suggest that the MI training produced measurable gains in the MI skills of the practitioners working in the IPV area. Participants who attended the workshop training demonstrated an increase in MI skills immediately after finishing the workshop based on the VASE-R NZ results. The full score significantly increased from pre-training (19.14) to post-training (27.14) which also yielded a medium effect size (r = 0.3).
Previous research utilising the VASE-R has also found VASE-R scores to significantly increase from pre- to post-MI training [32, 35, 36]. The findings of the current study indicated that participants in the present research performed better than the previous studies, with their total score on the VASE-R increasing by eight points (from 19.14 pre-training to 27.14 post-training), whereas changes reported in previous studies range from 4.12 (32) to 5.92 (35).
The subscale that had a significant increase from pre- to post-training in the current study was responding to resistance which was associated with a medium effect size as well (r = 0.33). This suggests that the biggest shift for the participants after MI training was in their response to client resistance, with a shift from responses that may engender resistance, or neutral responses, to responses that were likely to decrease resistance. This is of particular relevance to the IPV area, where client resistance, especially for mandated clients, can be common.
The eliciting change talk and summarising scales showed less change from pre- to post-training.
However, the lower scores on the summarising subscale may not reflect the ability of participants to develop a summary. A good summary, as defined based on the VASE-R is a summary that contains both change talk and ambivalence evident in the client’s statements. While the inclusion of these elements can be justified as consistent with MI, it may not be the case that both change talk and sustain talk should be included in a summary, especially if the practitioner was aiming to soften sustain talk. A possible change to the VASE-R scoring procedure could be to include either, rather than both, as the criterion for a full credit score [32].
The lack of change in the eliciting change talk subscale, however, was of a concern as eliciting or cultivating (as it is referred to in the MITI 4.2.1) change talk, is a core skill in MI. Difficulty in achieving proficiency in cultivating change talk is also mentioned in other studies (for e.g. [45]). This suggests that the technical component of MI may be more difficult to acquire than the relational component.
Further training, practice, and feedback, appears to have an impact on improving the practitioners’ skill in cultivating change talk. In the current research, practitioners were given feedback and extra materials and guidance on how to elicit change talk. In subsequent audio-recordings, a considerable improvement in eliciting change talk was seen for half of the participants (2 out of 4). The change in score was from 3.5 to 4 for one participant and 3 to 4 for the other.
These results are consistent with previous research showing that workshop training is sufficient to provide foundational exposure to MI and assists basic skill development, but insufficient to produce proficiency for practitioners to enable them to consistently implement MI in their practice [45]. On-going training supported by coaching and feedback is the most effective method to achieve proficiency in MI [46], with many individual competencies requiring upwards of a year to acquire. It has been recommended [45, 47, 48] that feedback and coaching based on observed practice are essential to build skilful MI practice, and is best done through in-session audio-recordings. The addition of coaching and feedback post-workshop plays an important role in the sustainability of MI skills, and those who do not have this feedback and coaching sessions do not reach to the proficiency level [26, 49].
All of the participants in the current study demonstrated at least a fair level of proficiency on R-Q and the %CR. Also, three out of four of them achieved at least a fair level of proficiency in their technical and relational skills. These results indicated that most of the participants who submitted audios had a fair level of proficiency in MI after training.
There was one participant though who had scores suggesting a fair level of proficiency in MI, but the coder noted that the participant received this score because there was no resistance or sustains talk in the session. The finding suggests that the MITI’s technical scale should be interpreted with caution. The impression of the coder was that this participant did not fully understand when MI should be used and was weak on the technical aspects of MI, while having good empathic listening skills. The reason for this could be that this participant did not attend all the workshop training (attended half day each day) and only attended two out of three of the MI refresher sessions. It appears that this participant may have needed more training in MI over an extended period of time.
A caution when interpreting the results of the current study is that the MI skills demonstrated in the recorded sessions may have been the participants’ best practice as they selected the client and session to record and submit for coding. Therefore, there is no guarantee that this represents their skills in routine encounters with clients. Ideally, future studies would record as many sessions as possible and then randomly select the audios to be reviewed and coded. Additionally, in the present research there was a high participant attrition rate. This suggests that the participants who provided audio-recordings were highly motivated to learn MI. The same results may not occur when training practitioners who are less interested in learning this approach.
In the current study, of the 10 participants who signed up to attend the 2-day MI training workshop, only seven completed it, and all participants did not attend all sessions. This problem has also been observed in other MI research, with possible causes identified as time constraints, high workload, and lack of agency support [35, 50-52], similar to the current research. This emphasises the importance of organisational support for MI training so that staff are provided with enough time out and reduced workloads to attend training, and they are allocated the necessary time and resources post-training to practice MI in order to further develop their skills.
Despite numerous reminders from the researchers few audio-recordings were submitted. This is consistent with other research [34, 35, 51]. There are a number of possible reasons as to why this may have occurred, including time constraints, forgetfulness, high staff turnover, and dislike for the MI approach or lack of engagement with the research. Additionally, there may be fundamental aspects of clinical activities in the community practice that make the use of recordings from client encounters difficult [34]. The difficulty with collecting audio-recordings of clinical sessions with real clients raises questions about the utility of the method for evaluating training in the community-based trials. Yet, as mentioned above, feedback on real practice of MI is important to develop MI skilfulness post-workshop training.
Further research needs to be undertaken to determine what additional measures can be taken to facilitate an increase in MI audio submission in real-work settings. Possible ways to increase participant engagement in submitting audios could include: allocating time for practice, encouragement and on-going support from management, as well as the inclusion of MI skill development, and supports within staff performance plans and appraisals [51]. Furthermore, it is recommended that practitioners’ willingness and readiness to engage in the MI skill development process be assessed before training in MI, and any concerns they may have to be subsequently addressed by the organisation.
CONCLUSION
Given the challenges with engagement in IPV interventions and the importance of intervention engagement for positive intervention outcomes, MI for engagement may be a useful skill for practitioners working in the IPV area to have. The current study showed that training in MI consisting of a 2-days workshop, plus post-workshop training (6 hours for some staff), and individual feedback and coaching, produced measurable gains (based on VASE-R NZ scores and MITI 4.2.1 coding of audio-recordings) in the MI skills of practitioners working in the area of IPV. These results were consistent with the findings of previous research. However, the findings of the current study are preliminary and should be interpreted with caution given the small sample, the diversity of training experience, and inconsistent completion of measures.
The results also suggest that practitioners working in the IPV area may be able to learn the basic skills of MI, but without comprehensive training, they might not be able to achieve proficiency in MI. Micro-counselling skills are necessary but insufficient to achieve the technical aspects (cultivating change talk) of MI. Mastering deeper level of reflections, evoking and strengthening change talk, while softening sustain talk requires training and on-going practice, feedback and coaching [53]. This requires organisational support for initial training, on-going training and audio-recording of practice for MI to be implemented successfully. Also, the level of ‘‘trainability’’ of staff in various roles may be different [30]. Some practitioners may have a greater interest in, or receptivity towards learning MI. Training those practitioners who have an interest and willingness to learn MI (i.e., attend training workshops, and provide on-going audio-recordings) and designating them as the primary deliverers of MI, might offer the most efficient route for integrating MI into practice [30].
- Babcock JC, Green CE & Robie C (2004) Does batterers' treatment work? A meta-analytic review of domestic violence treatment. Clin Psychol Rev 23: 1023-1053.
- Eckhardt CI, Murphy CM, Whitaker DJ, Sprunger J, Dykstra R, et al. (2013) The effectiveness of intervention programs for perpetrators and victims of intimate partner violence. Partner abuse 4: 196-231.
- Daly JE & Pelowski S (2000) Predictors of dropout among men who batter: A review of studies with implications for research and practice. Violence and victims 15: 137-160.
- Babcock JC & Steiner R (1999) The relationship between treatment, incarceration, and recidivism of battering: A program evaluation of Seattle's coordinated community response to domestic violence. J Fam Psychol 13: 46.
- Bennett GA, Moore J, Vaughan T, Rouse L, Gibbins JA (2007) Strengthening motivational interviewing skills following initial training: a randomised trial of workplace-based reflective practice. Addict Behav 32: 2963-2975.
- Gordon JA & Moriarty LJ (2003) The Effects Of Domestic Violence Batterer Treatment On Domestic violence recidivism: The Chesterfield County Experience. Crim Justice Behav 30: 118-134.
- Arias E, Arce R & Vilariño M (2013) Batterer intervention programmes: A meta-analytic review of effectiveness. Psicosoc Interv 22: 153-160.
- Hardy SA, Dollahite DC, Johnson N, Christensen JB (2015) Adolescent motivations to engage in pro‐social behaviors and abstain from health‐risk behaviors: A self‐determination theory approach. J Pers 83: 479-490.
- Naughton P, McCarthy SN & McCarthy MB (2015) The creation of a healthy eating motivation score and its association with food choice and physical activity in a cross sectional sample of Irish adults. Int J Behav Nutr Phy 12: 74.
- Miller WR & Rollnick S (2013) Motivational interviewing: Helping people change (3rd edition). New York, NY: Guilford Press; USA.
- Wagner CC (2013) Motivational interviewing and client-centered therapy. Interdisciplinary applications of the person-centered approach, Springer pp: 43-47.
- Rosengren DB (2014) Building Motivational Interviewing Skills. New York: Guilford Publications.
- Baker A & Hambridge J (2002) Motivational interviewing: enhancing engagement in treatment for mental health problems. Behav Change 19: 138-145.
- Dean S, Britt E, Bell E, Stanley J, Collings S (2016) Motivational interviewing to enhance adolescent mental health treatment engagement: a randomized clinical trial. Psychol Med 46: 1961-1969.
- Roberto SR, José Ramón FH, Cristina AM (2004) Motivational interviewing and treatment retention among drug user patients: A pilot study. Substance Use & Misuse 39: 1369-1378.
- Chlebowy DR, El-Mallakh P, Myers J, Kubiak N, Cloud R, et al. (2015) Motivational interviewing to improve diabetes outcomes in African Americans adults with diabetes. West J Nurs Res 37: 566-580.
- Lewis-Fernández R, Balán IC, Patel SR, Sánchez-Lacay JA, Alfonso C, et al. (2013) Impact of Motivational Pharmacotherapy on Treatment Retention Among Depressed Latinos. Psychiatr 76: 210-222.
- Lincourt P, Kuettel TJ & Bombardier CH (2002) Motivational interviewing in a group setting with mandated clients: A pilot study. Addict Behav 27: 381-391.
- Scott K, King C, McGinn H & Hosseini N (2011) Effects of motivational enhancement on immediate outcomes of batterer intervention. J Family Violence 26: 139-149.
- Soleymani S, Britt E & Wallace-Bell M (2018) Motivational interviewing for enhancing engagement in Intimate Partner Violence (IPV) treatment: A review of the literature. Aggress Violent Behav 40: 119-127.
- Stewart JS (2012) A Critical Appraisal of Motivational Interviewing within the Field of Alcohol Misuse. J Psychiatr Ment Hlt Nurs 19: 933-938.
- Zuckoff A, Swartz HA, Grote NK (2015) Motivational interviewing as a prelude to psychotherapy for depressed women. In H. Arkowitz, W.R. Miller, & S. Rollnick (Eds.), Motivational interviewing in the treatment of psychological problems (pp: 136-169). New York: Guilford Press.
- Schumacher JA, Madson MB, Nilsen P (2014) Barriers to learning motivational interviewing: A survey of motivational interviewing trainers' perceptions. Journal of Addictions & Offender Counseling 35: 81-96.
- Smith D, Hohman M, Wahab S & Manthey T (2017) Student-perceived quality of motivational interviewing training: A factor-analytic study. Journal of the Society for Social Work and Research 8: 1-18.
- Martino S, Ball SA, Nich C, Frankforter TL, Carroll KM (2008) Community program therapist adherence and competence in motivational enhancement therapy, Durg Alcohol Depend 96: 37-48.
- Miller WR, Yahne CE, Moyers TB, Martinez J, Pirritano M (2004) A randomized trial of methods to help clinicians learn motivational interviewing. J Consult Clin Psychol 72: 1050-1062.
- Moyers TB, Manuel JK, Wilson PG, Hendrickson SML, Talcott W, et al. (2008) A randomized trial investigating training in motivational interviewing for behavioral health providers. Behav Cogn Psychother 36: 149-162.
- Schwalbe CS, Oh HY & Zweben A (2014) Sustaining motivational interviewing: A meta‐analysis of training studies. Addic 109: 1287-1294.
- Walters ST, Matson SA, Baer JS & Ziedonis DM (2005) Effectiveness of workshop training for psychosocial addiction treatments: a systematic review. J Subst Abuse Treat 29: 283-293.
- Cook PF, Manzouri S, Aagaard L, O’Connell L, Corwin M, et al. (2017) Results from 10 years of interprofessional training on motivational interviewing. Eval Health Prof 40: 159-179.
- Soleymani S (2019) Motivational interviewing for enhancing engagement in intimate partner violence intervention. Doctor of Philosophy, University of Canterbury: New Zealand.
- Rosengren DB, Hartzler B, Baer JS, Wells EA, Dunn CW (2008) The video assessment of simulated encounters-revised (VASE-R): Reliability and validity of a revised measure of motivational interviewing skills. Drug Alcohol Depend 97: 130-138.
- McMaster H (2012) Hall McMaster & Associates Limited.
- Baer JS, Rosengren DB, Dunn CW, Wells EA, Ogle RL, et al. (2004) An evaluation of workshop training in motivational interviewing for addiction and mental health clinicians. Drug Alcohol Depend 73: 99-106.
- Dear EJP (2014) Evaluating motivational interviewing measures of knowledge and skill using training outcome data. University of Canterbury. Psychology.
- Doran N, Hohman M & Koutsenok I (2011) Linking basic and advanced motivational interviewing training outcomes for juvenile correctional staff in California. J Psychoact Drugs 43: 19-26.
- Hohman M, Doran N & Koutsenok I (2009) Motivational interviewing training for juvenile correctional staff in California: One year initial outcomes. J Offender Rehabil 48: 635-648.
- Moyers TB, Manuel JK & Ernst D (2014) Motivational Interviewing Treatment Integrity Coding Manual 4.2.1. University of New Mexico. pp: 1-40.
- Moyers TB, Rowell LN, Manuel JK, Ernst D, Houck JM (2016) The motivational interviewing treatment integrity code (MITI 4): rationale, preliminary reliability and validity. J Subst Abuse Treat. 65: 36-42.
- McCambridge J, Day M, Thomas BA & Strang J (2011) Fidelity to motivational interviewing and subsequent cannabis cessation among adolescents. Addict Behav 36: 749-754.
- Woodin EM, Sotskovaa A & O’Leary KD (2012) Do Motivational Interviewing Behaviors Predict Reductions in Partner Aggression for Men and Women? Behav Res Ther 50: 79-84.
- Miller WR & Rollnick S (2009) Ten things that motivational interviewing is not. Behavioural and cognitive psychotherapy 37: 129-140.
- Fritz CO, Morris PE & Richler JJ (2012) Effect size estimates: current use, calculations, and interpretation. J Exp Psychol Gen 141: 2-18.
- McHugh ML (2012) Interrater reliability: the kappa statistic. Biochemia medica 22: 276-282.
- Forsberg L, Forsberg LG, Lindqvist H & Helgason AR (2010) Clinician acquisition and retention of Motivational Interviewing skills: a two-and-a-half-year exploratory study. Subst Abuse Treat Prev Policy 5: 8.
- Hall K, Staiger PK, Simpson A, Best D, Lubman DI (2016) After 30 years of dissemination, have we achieved sustained practice change in motivational interviewing? Addict 111: 1144-1150.
- Doherty Y, Hall D, James PT, Robert SH, Simpson J (2000) Change counselling in diabetes: the development of a training programme for the diabetes team. Patient Educ Couns 40: 263-278.
- Miller WR & Rollnick S (2012) Motivational interviewing: Helping people change. Guilford press.
- Schoener EP, Madeja CL, Henderson MJ, Ondersma SJ, Janisse JJ (2006) Effects of motivational interviewing training on mental health therapist behavior. Drug Alcohol Depend 82: 269-275.
- Berger LK, Otto-Salaj LL, Stoffel VC, Hernandez-Meier J, Gromoske AN (2009) Barriers and facilitators of transferring research to practice: an exploratory case study of motivational interviewing. J Soc Work Pract Addict 9: 145-162.
- Wilkinson VR (2015) Motivational interviewing in Child, Youth and Family residences: case leaders' experiences, appraisal and skill level, and the barriers to implementation. Master's Thesis. University of Canterbury: New Zealand.
- Wood AR, Ager RD & Wood RJ (2011) Motivational interviewing: A qualitative examination of factors impacting adoption and implementation in a community-wide setting. J Soc Work Pract Addict 11: 336-351.
- de Roten Y, Zimmermann G, Ortega D & Despland JN (2013) Meta-analysis of the effects of MI training on clinicians' behavior. J Subst Abuse Treat 45: 155-162.
- Moyers TB, Martin T, Manuel JK, Hendrickson SML & Miller WR (2005) Assessing competence in the use of motivational interviewing. J Subst Abuse Treat 28(1): 19-26.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6
-
Table 7








QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Advance Research on Alzheimers and Parkinsons Disease
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Pathology and Toxicology Research
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- Journal of Allergy Research (ISSN:2642-326X)


