Journal of Womens Health and Safety Research (ISSN:2577-1388)

Research Article
The Capability of Family to Care Improves the Nutrition Fulfillment of School-Age Children
6855
Views & Citations5855
Likes & Shares
Good nutrition contributes to the growth and development of school-age children. This s tudy aims to determine the relationship between family characteristics and family health care tasks in the nutrition fulfilment with the nutritional status of school-age children. Th is study was cross-sectional and used the proportional random sampling method with 27 6 respondents. The samples were 4th to 5th grade elementary school students and their p arents in Kelurahan Pondokranggon. The statistical test was carried out using chi-square and logistic regression. The results showed that there was a significant relationship betw een the number of children in the family and the capability of the family to care for the n utritional status of school-age children. The nutritional status of school-age children is in separable from the capability of the family to perform family health care tasks, especially y the capability of the family to care.
Keywords: Capability of family to care, Nutritional status, School-age children
INTRODUCTION
As the physical growth of school-age children increases, their cognitive and social development as well as activity also increase so that supporting factors for this fulfillment are needed. One of the supporting factors is meeting the nutritional needs of school-age children. The fulfillment of the nutritional needs of school-age children is influenced by various risk factors. According to Stanhope and Lancaster, risk factors include age, biology, environment, and lifestyle. Age 6 to 12 years is an age group at risk of nutritional problems due to unbalanced income [1] Biological factor (genetic) is one of the causes of overweight. Environmental factor includes the social and physical environment [2]. The social environment includes economic factors, where there is a relationship between financial resources and needs. Families that have adequate economic resources can accommodate their health. This is also made clear in Hitchock in that economic status is a significant factor to determine health and nutritional status. Children living in poverty experience poor nutrition [1,2]. One of the social factors that affects nutritional status is family factor [3]. Family factor in this case includes the ability to provide food, family parenting, the type of food provided by the family, and the dissemination of food [4]. Family behavior and health practices in the family strongly influence family health [5]. Kaakinen also emphasized that if one family member takes the initiative to change the behavior, other family members will also make changes. Sociocultural factor also influences the nutritional status of school-age children. The sociocultural factor referred to here is the mass media. Mass media influence individuals in health behaviors. The media gives positive and negative things to what is displayed [6] (Pender, 2002). This is confirmed in the research of Batada, Seitz, Wootan, and Story, in 2008 that although families can be models and encourage healthy eating behavior, the mass media give a great influence in food selection. According to the data from Indonesia Basic Health Research (RISKESDAS) in 2013 [7] showing a national prevalence of school-age children (6 to 12 years old), the undernutrition category was 11.2% and the overnutrition was 18.8%. According to the data from Kelurahan Pondokranggon. I Public Health Center in 2013, [8] from the results of first grade screening in six schools, the data on undernutrition (0.78%), good nutrition (83.34%), and overnutrition (15.88%) were obtained. According to the results of the interview with the public health center, school- age children often got to consume snacks bought outside the school even though there were several schools that already had school canteens. Snacks that were consumed were like cilok (Indonesian meatball made from tapioca flour) with sauce. This is justified by the statement from the school teacher who said, “Even though children bring lunch from home, they still buy snacks”. Based on the aforementioned background, community nurses needed to conduct research on “the family capability to care in the nutrition fulfillment with the nutritional status of school-age children in Kelurahan Pondok Ranggon”.
METHODS
This study employed a descriptive correlation with a cross-sectional approach. The sample was chosen using the proportional random sampling method with 276 respondents. The sample were 4th to 5th grade elementary school students and their parents in East Jakarta. Before conducting the study, an ethical test and validity test of the questionnaire were conducted. The ethical principle applied by the researcher was the principle of justice through informed consent. The study was carried out from May 2014 until August 2014.
RESULTS
The distribution of respondents based on the nutritional status of school-age children showed that the majority of respondents (59.8%) were in good nutrition (-2SD to 1 SD). The distribution of respondents based on the family capability to carry out family health care tasks was 59.8%. The family capability to care for the nutrition of school-age children was 54.7%, almost the same as the family who was able to modify the environment in the nutrition fulfillment (54%), and more than half of the families (58.7%) were able to utilize health services. The results of the analysis based on the role of peers showed that mostly the role of peers in the nutritional status of school-age children was good at 62.3%.
Bivariate Analysis
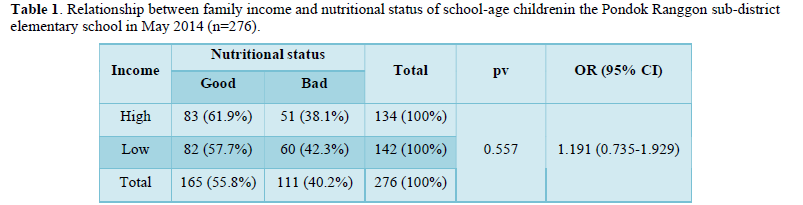
The results of the analysis showed that high family income (minimum wage: >2,440,000) had school-age children with good nutritional status of 61.9%, while the income less than the minimum wage had good nutrition of 57.7%. However, the statistical test results showed no relationship between family income and nutritional status of school-age children (p = 0.557) (Table 1).
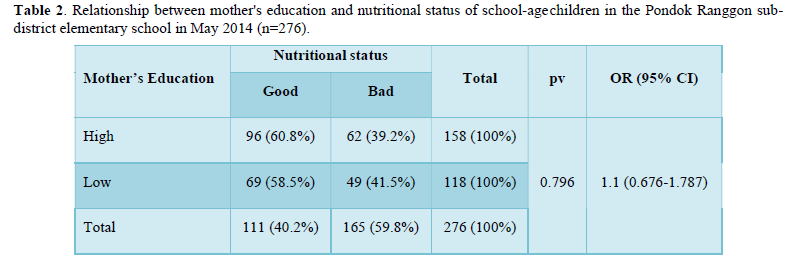
The results of the analysis showed that well-educated mothers had school-age children with good nutritional status of 60.8% and low-educated mothers had school-age children with good nutritional status of 58.5%. However, the results of the chi square test showed that there was no relationship between maternal education in the family and the nutritional status of school-age children (p=0.796) (Table 2).
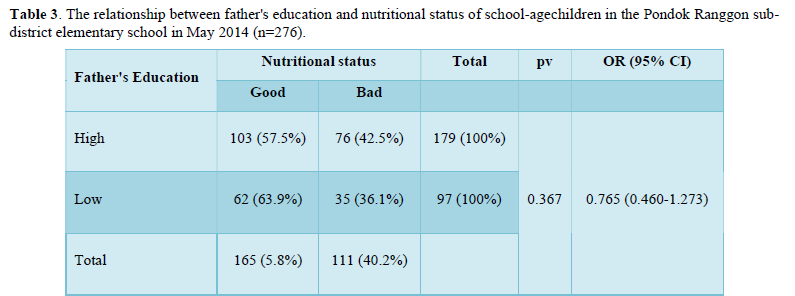
The results of the analysis showed that well-educated fathers had school-age children with good nutritional status of 57.5%, while low-educated fathers had school-age children with good nutritional status of 63.9%. The statistical test results showed no relationship between paternal education and nutritional status of school-age children (p = 0.367) (Table 3).
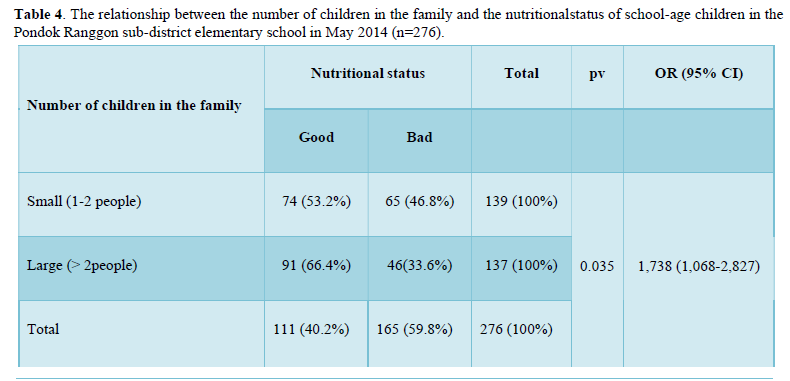
The results of the analysis showed that the number of children in large families (>2 people) that had school-age children with good nutritional status was 66.4%, while the number of children in small families (1-2 people) had good nutritional status of 53.2%. The results of the chi square test showed that there was a relationship between the number of children in the family and the nutritional status of school-age children (p=0.035). The results of the analysis also showed OR = 1,738, meaning that family with a greater number of children (>2 people) had a 1.7 times chance of having school-age children with good nutritional status compared to the number of children in small families (Table 4).
The results of the analysis of the family capability to care showed that good family capability to care for school-age children with good nutritional status was 94%, while with not good nutrition was only 6%. The results of the chi square test showed that there was a relationship between the family capability to care and the nutritional status of school-age children (p=0.00). The results of the analysis also showed OR = 6.303, meaning that the good family capability to care had a chance of 6.3 times to have school- age children with good nutritional status compared to the bad family capability to care (Table 5).
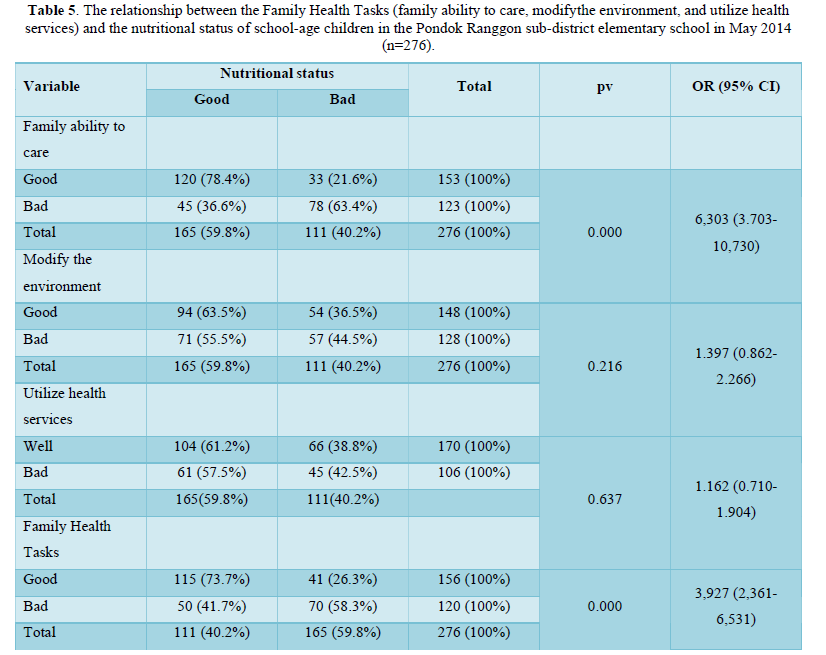
In terms of the family capability to modify the environment, the good family capability to modify a good environment had school-age children with good nutritional status of 63.5%. The results of the chi square test showed that there was no relationship between the family capability to modify the environment and the nutritional status of school-age children (p = 0.182). The results of the analysis in terms of the family capability to utilize health services showed that the family capability to utilize good health services who had school-age children with good nutritional status was 61.2% compared to the bad family capability to utilize health services who school-age children with good nutritional status was 41.7%. The results of the chi square test showed that there was no relationship between utilizing nutritional health services and the nutritional status of school-age children (p = 0.637). It can be concluded from the whole analysis process that the ability of the family to care affects the nutritional status of school-age children because it has the largest OR, which is 6,303. The ability of a family to take good care has a 6.3 times chance (CI: 3.703 - 10.730) to have a good nutritional status of school-age children compared to the ability of a family who to take a bad care.
DISCUSSION
High- and low-income families have a similar contribution in determining the nutritional status of school-age children. According to the researcher's analysis, the nutritional status was influenced by various factors. It is not only the status of family income, but also family knowledge in processing the right food for school-age children that can be obtained through information from printed and electronic media related to balanced nutrition for school-age children. A significant relationship between education and the nutritional status of school-age children was also not found. According to the researcher's analysis, the fulfillment of school-age children's nutrition was not only due to educational factors. However, it could be influenced by observational factor, imitating and changing one's own behavior. It could also be influenced by the availability of maternal time in paying attention to the nutritional needs of school-age children, in this case, mothers who did not work.
The results of the analysis showed that the number of children in large families (>2 people) mostly had school-age children with good nutritional status of 66.4%. This is contradictory in theory. [1] Allender and Spradley stated that the smaller the number of children in one family, the better the nutritional status of the child associated with the availability of food. According to the researcher's analysis, the number of children in the family was not the main factor determining the nutritional status, but was influenced by multifactor such as income, work, education, positive experiences, and mass media influence. The results of this study indicated that the family capability to care was the dominant factor in influencing the nutritional status of school-age children. The state of nutritional status was inseparable from the family capability to perform care where care is associated with family health behaviors. Behavior is related to the level of knowledge, skills, and attitudes possessed by the family. Lack of knowledge on how to care means the lack of family capability to prevent and fulfill balanced nutrition. In theory, family also becomes a role model in other family members positively and negatively [5]. Family behavior and practices also affect health which includes feeding practices and the type of food consumed [5]. Food-related dissemination and family eating behavior also affect the nutritional status of school-age children.
CONCLUSION
Low and high family income equally play a role in the nutritional status of school-age children. Nutritional status is not absolutely influenced by family income, because not all families use their family income wisely in fulfilling nutrition. With low income but wise financial management, nutritional status will be fulfilled.
Most parents (mother and father) had higher education, namely senior high school. The results showed no relationship between education and the nutritional status of school-age children. The nutritional status of school-age children was not only influenced by education, but also by the maternal time availability. Families found and got information about nutrition through the media. Nutritional status was influenced by various factors. This could be due to the family knowledge about the nutrition of school-age children, the influence of mass media, and positive experiences from mothers. The family capability to care was the dominant variable affecting the nutritional status of school-age children. The nutritional status of school-age children can be improved through improving the knowledge and skills of families in providing balanced food to school-age children.
- Allender, Rector, Warner. (2010) Community health nursing: Promoting and protecting the public health, 7th Philadelphia: Lippincott.
- Hittchock JE, Phyllis ES, Sue AT (1999) Community health nursing. Caring in action. New York. Del mar Publisher. pp: 639-649.
- Lancaster S (2010) Community public health nursing. 6th USA. Mosby Company. pp: 594-613.
- Taylor JP, Evers S, McKenna M (2005) Determinants of healthy eating in children and youth. Can J Public Health 3: S20-S26, S22-S9.
- Kaakinen J, Gedaly DV, Coehlo D, Hason S (2010) (Eds.) Family Health Care Nursing: Theory, Practice, and Research; 4th
- Nola JP (2002) Health Promotion in Nursing 5th edn. USA. Prentice hall; pp: 192-202.
- Gomes C (2013) Family and women decide child Sci Res 5(7): 1132-1140.
- James (2013) Nursing care of children: principles and practice. 4th St. Louis: Elsevier.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5





QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Proteomics and Bioinformatics (ISSN:2641-7561)
- Journal of Microbiology and Microbial Infections (ISSN: 2689-7660)
- Food and Nutrition-Current Research (ISSN:2638-1095)
- Journal of Genetics and Cell Biology (ISSN:2639-3360)
- Advances in Nanomedicine and Nanotechnology Research (ISSN: 2688-5476)
- Journal of Astronomy and Space Research
- Journal of Biochemistry and Molecular Medicine (ISSN:2641-6948)


