
3865
Views & Citations2865
Likes & Shares
Methods: A prospective randomized study was started with a pilot project at the department of Anesthesiology and Intensive Care Medicine, University Hospital of Ostrava. The prospective randomized study included 111 patients after total hip arthroplasty. Analgesic therapy for the group of respondents was carried out according to the protocol for analgesic therapy.
Results: Significantly higher patient satisfaction with controlled analgesia according to the Likert scale was demonstrated. In patients with the patient-controlled analgesia method, there was a statistically significant difference in the consumption of analgesics during the first 24 h after surgery.
Conclusion: The Acute pain service system has been operating at the University Hospital of Ostrava since 2015. It takes care of 800 patients with postoperative pain annually. As part of the application of multimodal analgesia, the method of patient-controlled analgesia is also used. This method brings patients greater satisfaction, faster rehabilitation and lower consumption of analgesics during the first 24 h after surgery.
Keywords: Acute pain service, Patient-controlled analgesia, Multimodal analgesia, Satisfaction
The nurse of the APS team regularly monitors patients with postoperative pain, assesses pain, records, monitors the effect of analgesic therapy, occurrence of adverse effects. The APS informs the doctor about the occurrence of complications of analgesic treatment. The APS team monitors all patients with established analgesic therapy using a seductive anesthetic technique (central anesthetic blocks with epidural, subarachnoid catheter, peripheral blocks), patients with difficult-to-manage pain after surgery. At the same time, as part of the expansion of the patient-controlled epidural analgesia (PCEA) method, these patients are being cared for. Patients using PCEA generally obtain better pain relief compared to patients with conventional analgesia, without an increase in adverse effects. The PCA effect has been compared many times by numerous studies - the results are not always clear-cut. One of the significant benefits of this treatment is the active involvement of the patient in the treatment and the feedback for the doctors who can analyze the consumption of the analgesic and thus assess the level of postoperative pain of the patient [1].
METHODS
A prospective randomized study was started with a pilot project at the inpatient department of KARIM FN Ostrava. 24 patients were included in the pilot part of the study. After the evaluation of the pilot study, a prospective randomized study was started, 111 patients were included after total hip arthroplasty. Analgesic therapy for the group of respondents was carried out according to the protocol for analgesic therapy. After transfer to the standard department, each patient included in the study is evaluated by a satisfaction questionnaire according to the Likert scale [2], patients randomized to the PCEA group were evaluated by the Patient Ease-Of-Care Questionnaire (EOCQ) (Table 1) to assess satisfaction and understanding of the patient-controlled analgesia method. Use of the score was approved by e PROVIDE TM Online support for Clinical Outcome Assessments. During the first rehabilitation on the patient's bed, she was evaluated by the physiotherapist VAS during mobilization. Basic descriptive statistics (frequency table, median, arithmetic mean) were used to evaluate the obtained data. A two-sample non-parametric Wilcoxon test was used to evaluate the VAS of individual observed hours in PCA and non-PCA patients. Statistical tests were evaluated at a significance level of 5%, the Stata version 13 program was used for evaluation.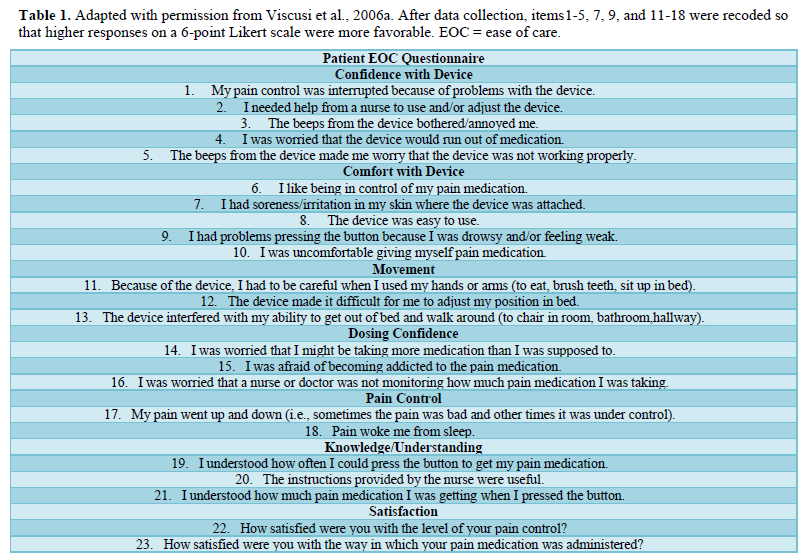
RESULTS
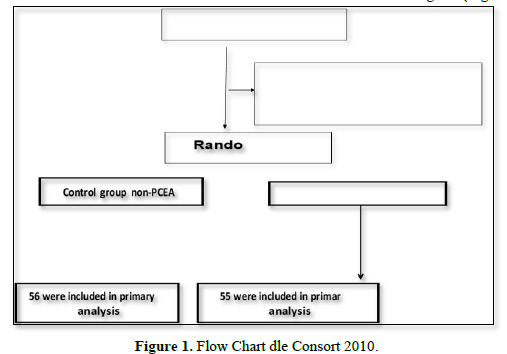
Based on the criteria for inclusion in the study, 175 patients were included in the study and 81 were excluded from the total number of 256 patients after total endoprosthesis hospitalized during the monitored period at KARIM in FNO. The reason for not being included in the study was the pharmacological anamnesis of the patients, the polymorbidity of the patients evaluated according to the ASA score. 64 patients were excluded, of which 14 were patients who refused to cooperate and 50 cases were excluded due to occlusion or malfunction of the epidural catheter. A total of 111 patients were randomized, 55 patients were included in the group analgesized according to the protocol for patient-controlled epidural analgesia (PCEA group). The control group of respondents (non-PC EA) consisted of 56 patients. Graphically represented in the Flow chart according to Consort 2010 Flow Diagram (Figure 1).
Based on the data obtained after the analysis, significantly higher satisfaction with the administration of the analgesic mixture was demonstrated in patients in the PCEA group than in patients in the non PCEA group. Patient satisfaction was evaluated according to the Likert scale score. The mean value for patients with PCEA was 2.77, while for patients with non-PCEA the mean value was 4.33. Average satisfaction in the total group was rated 3.54. A statistically significant difference (p<0.001) was found between the PCEA and non- PCEA groups (Chart 1).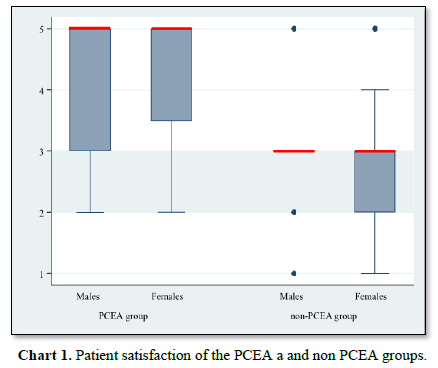
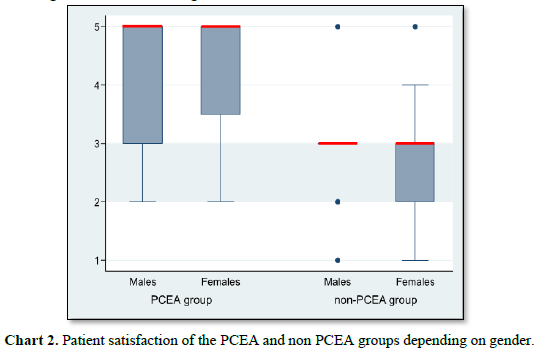
When evaluating the effect on patient satisfaction of the PCEA method of analgesia and non PCEA method of analgesia according to the gender of the respondents of both groups, a statistically significant difference was found (p = 0.014). Men predominate in the PCEA group, which was also reflected in overall higher satisfaction among men, but only in connection with inclusion in the group. No statistically significant difference (p = 0.510) was found when evaluating gender dependence on satisfaction with the chosen method of administering analgesic therapy (Chart 2).
For patients in the monitored group of PCA respondents, patient satisfaction was assessed using the validated Patient EOC Questionare score.
Based on the analysis of the obtained data, it can be stated that the patients expressed their satisfaction with the chosen method of pain treatment using PCEA. When assessing the intensity of pain according to the VAS within 24 h. of ICU hospitalization, pain was of lower intensity in patients in the PCEA group than in the non- PCEA group. Only in three cases was the VAS value statistically significantly higher. A higher intensity of pain was reported by patients in the PCEA group 6 h after the start of analgesic therapy (p=0.021), then 10 h (p=0.011) and 23 h (p=0.029). The average VAS value in the PCEA group was 1.06 at a maximum intensity of 6, in the nonPCEA group the average VAS value was 1.02 at a maximum intensity of 8 (Chart 3).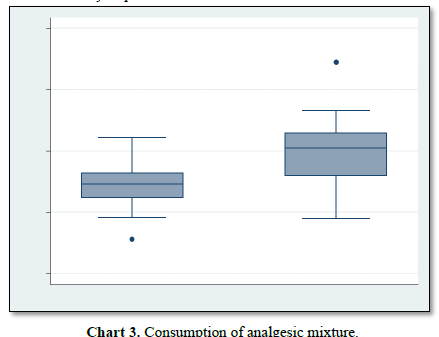
We also monitored the intensity of pain during the first rehabilitation in postoperative care after transfer to the orthopedic department. The highest VAS value at the first mobilization of the patient was 7 in the PCEA group and 9 in the non-PCEA group. From these results, it can be concluded that patients in whom analgesia was applied in postoperative care using the method of patient-controlled analgesia had a lower pain intensity during the first rehabilitation than patients who received analgesics at the request of a nurse according to a doctor's office. According to the physiotherapists, the patients of the PCEA group also cooperated better during the first mobilization with regard to the optimization of analgesia.
DISCUSSION
Data from studies abroad, but also in the Czech Republic, show a still relatively high number of patients who suffer from intense pain accompanied by acute or chronic adverse consequences after surgery [3]. Approximately 30-80% of patients experience moderate or severe pain in the first postoperative hours and days, especially after surgery on the limbs or spine [4]. Despite all efforts, postoperative pain management currently remains suboptimal and effective treatment of postoperative pain is still a problem [4]. Of the postoperative patients, 275 (72%) described the pain as severe, and 89.3% assessed it the same during movement as part of early mobilization. Strong analgesics were prescribed only in 51.5% of cases, and the most common type of analgesia was the administration of paracetamol. Untreated or insufficiently treated pain leads to delayed initiation of rehabilitation, deterioration of walking training and basic self-care, thereby limiting the patient's return to his normal daily routine. In addition, the patient is at risk of a number of health complications caused by a prolonged stay in bed, such as thromboembolic disease or pulmonary dysfunction [5]. The aim of the prospective study was to evaluate the effect of the PCEA method with analgesia administered at the request of the patient by a nurse according to the doctor's office, considering the patient's satisfaction with the chosen method of analgesia. Effective postoperative analgesia is an important factor that affects the overall postoperative course, especially with regard to the patient's satisfaction and his return to normal life [5]. The advantage of patient-controlled analgesia is the active participation of the patient in the treatment, which requires cooperation with the entire treatment team. Based on the results of the study, higher patient satisfaction with the PCEA method was demonstrated. Satisfaction ratings are often considered an important parameter of the patient's view of treatment effectiveness. A certain correlation between satisfaction and lower pain intensity can be assumed [6]. However, satisfaction ratings are quite controversial. It is known that patient satisfaction surveys tend to yield positive results because patients are reluctant to criticize the treatment process [7]. There are many patients who experience quite high levels of pain and yet report satisfaction with pain management [6,7]. Similarly, when evaluating the satisfaction and outcome of patients after surgical, orthopedic and gynecological surgery in a prospective study by Gottschalk et al [8] concluded that PCEA provides higher satisfaction independently of the maximum intensity of pain according to the VAS [8]. Patient cooperation during the treatment process is important for the success of analgesic therapy, where adequate patient education plays an important role. Chumbley [9] evaluated patient satisfaction with the PCA method in their study. They concluded that 22% of patients expressed concern about dependence on analgesic therapy, 30% of patients feared overdose of analgesics, and 43% were not adequately instructed. The conclusion of this study was the finding that a lack of information about PCA was associated with an assessment of higher pain intensity [9]. Similarly, Ahmad I, et. al. within the framework of 5 years of experience with the PCA method, he drew attention to the importance of adequate education, which can minimize the occurrence of complications with PCA [10]. A significant benefit of PCA pain treatment is the active involvement of the patient in the treatment and, at the same time, feedback for doctors who can analyze the consumption of analgesics and thus assess the patient's level of postoperative pain [11]. A person tolerates pain better if he is under control and can influence it himself intensity [1]. Another significant contribution demonstrated in the work of Ciaralli [12] was the reduction of anxiety and stress of patients who thus became independent of the nursing staff. To optimize the identification of suitable patients for the method of patient-controlled analgesia, the question is whether it would not be appropriate to perform a test of the level of cognitive function. There are not enough studies to assess the effect of the method of patient-controlled analgesia with regard to the level of cognitive function of patients. Eugene [13] reviewed the cases of ten adults aged 65 years and older who were admitted to the geriatric or orthopedic services of an urban tertiary care center in New York City with acute pain and cognitive impairment or dementia and received PCA analgesia. The study concluded that patient-controlled analgesia can be used successfully in older adults with cognitive impairment. Considering the technical difficulties in selected patients, further research would help to improve pain management in this particularly vulnerable population [13]. Keita assessed the level of cognitive functions according to the Minimental examination, which did not show a difference between the observed groups. One of the requirements for the optimal course of postoperative care is early mobilization. Timely and sufficient analgesia facilitates more frequent mobilization, enables faster discharge to ambulatory care, and reduces postoperative complications. In our study, a positive effect of the PCA method on pain intensity during the first rehabilitation was demonstrated. Patients cooperated better with physical therapists. In terms of mobilization, Singelyn FJ [14] PCEA, continuous femoral blocks and patient-controlled intravenous analgesia (PCIA), where the result was that there is no statistically significant difference between the mentioned methods [14]. Vincent [15] compared in their study the effect of transdermal fentanyl patch and PCIA in patients after total arthroplasty. In this study, a higher effect of transdermal patches was demonstrated [15]. The effect of patient-controlled analgesia during the first mobilization was compared in a study by Keïta [16]. They compared a group of patients with PCA administered intravenously with an analgesic mixture with morphine and a group of patients where an analgesic mixture with morphine was administered subcutaneously at regular intervals. A group of PCA patients with an intravenously administered analgesic mixture had a lower VAS at mobilization than a group with subcutaneously administered morphine at regular intervals [16]. The indisputable importance of the PCA method is the fact that this method represents lower demands on a qualified force, which can devote more time to other nursing interventions. According to Rgon [17] PCA provides better pain management and is easier for nurses. Using a questionnaire survey, they assessed nurses' attitudes towards PCA. The conclusion was that 80% of nurses perceive the necessity of regular patient check-ups positively with regard to mutual interaction with the patient, some negatively, due to lack of time. They drew attention to the importance of adequate patient education, optimally using educational materials and an instructional video [19]. In a meta-analysis by Bainbridge [18] and the systematic review by Walder [19] randomized trials comparing nurse practitioner-administered analgesia (NCA) with intravenous PCA with opiates in postoperative pain after cardiac surgery, the authors confirmed the efficacy of PCA versus NCA. Patients were more satisfied, had lower pain intensity, and a lower incidence of unwanted complications associated with the application of opioid analgesics was demonstrated [18,19]. Similarly, the Cochrane review analyzed the effect of patient-controlled analgesia and concluded that the method of providing analgesia in the form of PCEA can be useful in patients after total hip arthroplasty, especially for optimal pain control of the patient, offering higher analgesic efficiency and lower requirements for additional analgesic doses in comparison with the method of patient-controlled intravenous analgesia. At the same time, the conclusion of the analysis was that PCEA ensures greater patient satisfaction compared to administration of analgesics at time intervals or continuous infusion according to the physician's office.
CONCLUSION
The Acute pain service system has been operating at the Ostrava University Hospital since 2015. As part of the application of multimodal analgesia, the method of patient-controlled analgesia is also used. This method to patients brings higher satisfaction, faster rehabilitation and lower consumption of analgesics during the first 24 h after surgery.
- Surprise JK, Simpson MH (2014) PCA: Is that Patient- or Provider-Controlled J Radiol Nurs 33(1): 18-22.
- Pennington P, Caminiti S, Schein JR, Hewitt DJ, Nelson WW (2009) Patient Assessment of the Convenience of Fentanyl HCI Intophoretic Transdermal System (ITS) Versus Morphine Intravenous Patient-Controlled Analgesia (IV PCA) in Management of Postoperative Pain After Major Surgery. Pain Manag Nurs 10(3): 124-133.
- Malek J, Sevcik P (2014) Treatment of postoperative pain. additional Prague: Mladá Fronta. pp: 135.
- Pöpping DM, Zahn PK, Van Aken HK, Dasch B, Boche R, et al. (2008) Effectiveness and safety of postoperative pain management: A survey of 18,925 consecutive patients between 1998 and 2006 (2nd revision): A database analysis of prospectively raised data. Br J Anaesth 101: 832-840.
- Catrina CC, Sindura B, Steven DK, Susan HO, Christine MV, et al. (2012) Patient-controlled versus scheduled, nurse-administered analgesia following vaginal reconstructive surgery: A randomized Am J Obstet Gynecol 207(5): 433-436.
- Pellino TA, Ward SE (1998) Perceived Control Mediates the Relationship between Pain Severity and Patient Satisfaction. J Pain Symptom Manage 15: 110-116.
- Jamison RN, Taft K, O'Hara JP, Ferrante FM (1993) Psychosocial and Pharmacologic Predictors of Satisfaction with Intravenous Patient-Controlled Anesth Analg 77: 121-125.
- Gottschalk A, Freitag M, Liehr K, Domke A, Schuster M, et al. (2004) Does Patient Satisfaction Correlate with Pain Level During Patient-Monitored Epidural Evaluation of data from Postoperative Pain service. Der Schmers 18: 145-150.
- Ali M, Winter DC, Hanly AM, O'Hagan C, Keaveny J, et al. (2009) Prospective, randomized, controlled trial of thoracic epidural or patient-controlled opiate analgesia on perioperative quality of life. Opioid Manag 5(5): 307-312.
- Chumbley GM, Hall GM, Salmon P (1998) Patient-Controlled Analgesia: An Assessment by 200 patients. Anesthesia 53: 216-221.
- Ahmad I, Thompson A, Frawley M, Hu P, Heffernan A, et al. (2010) Five-year Experience of Critical Incidents Associated with Patient Controlled Analgesia in An Irish University Ir J Med Sci 179(3): 393-397.
- Ciaralli I (2009) Patient controlled analgesia. Paediatr Child Health 10(19): 83-84.
- Eugene L, Eugenia LS, Carrington MR (2009) Can he cognitively impaired safely use patient-controlled analgesia? J Opioid Manag 5(5): 307-312.
- Singelyn FJ, Ferrant T, Malisse MF, Joris D (2005) Effect in intravenous patient-controlled analgesia with morphine, continuous epidural analgesia, and continuous femoral nerve sheath block on rehabilitation after unilateral total-hip Reg Anesth Pain Med 30(5): 452-457.
- Vincent M, Vincent L, Vincent B, Antoine P, Anna R, et al. (2008) Postoperative analgesia after total hip arthroplasty: Patient controlled analgesia versus transdermal fentanyl patch. J Clin Anesth 20(4): 280-283.
- Keïta H, Geachan N, Dahmani S, Couderc E, Armand C, et al. (2003) Comparison between Patient Controlled Analgesia and Subcutaneous Morphine in elderly patients after total hip replacement. Br J Anaesth 90(1): 53-57.
- Rgon MA, Walsh SK (2007) I think PCA is great, But-Surgical nurses ‘perceptions´ of patient-controlled analgesia PCA. Int J Nurs Pract 13: 276-283.
- Bainbridge D, Martin JE, Cheng DC (2006) Patient-controlled versus nurse- controlled analgesia after cardiac surgery: A meta-analysis. Can J Anaesth 53: 492-499.
- Walder B, Schafer M, Henzi I, Tramèr MR (2001) Efficacy and Safety of Patient-Controlled Opoid Analgesia for Acute Postoperative Pain: A Quantitative Systematic Acta Anaesthesiol Scand 45: 795-804.
-
 Table 1
Table 1





QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Chemotherapy Research Journal (ISSN:2642-0236)
- Journal of Allergy Research (ISSN:2642-326X)


