
2998
Views & Citations1998
Likes & Shares
Results: The correlation analysis showed a significant association between gender, age, education, physical and mental health components with fatigue in the total sample. Gender was not significant with fatigue in Greek patients, and disease duration was significant in association with fatigue. In Slovak patients, age was not significantly associated with fatigue. The results of the linear regression analysis showed in the final model with both, physical and mental components, are in significant association with fatigue in the total sample, as well in Slovak and Greek patients separate. Gender was also significant in the final model, but only in the total sample. The final regression models explained between 20-62% of the total variance in our samples.
Conclusion: Although fatigue is mostly categorized as a physical symptom, our results supported the finding that a variety of factors, such as mental health. Thus, the management of fatigue needs to take into account the psychological, biochemical and physiological aspects, and the underlying mechanism of fatigue, therefore the individual approach is needed.
Keywords: Rheumatoid arthritis, Fatigue, Physical health, Mental health, Cultural differences
Abbreviations: MSC: Mental Health Summary Component; PSC: Physical Health Summary Component; RA: Rheumatoid Arthritis; SD: Standard Deviation; SF-36: The 36-item Short Form Health Survey; VAS: Visual Analogue Scale
Clinical variables were studied in association with fatigue but with unclear results. For example, disease duration in more studies was reported to not have a significant association with fatigue, which is surprising because of the progressive course of RA, and its worsening impact on patients [11,12]. Due to common comorbidities in RA, especially cardiovascular and respiratory, patients reported higher levels of fatigue. Moreover, a medication used for those comorbidities can influence it too [4]. Also, sociodemographic variables were found to play a role in experiences levels of fatigue. Gender was found to be associated with female patients and greater fatigue [1,3]. Also, patients with lower educational levels reported more fatigue [13,14]. Despite the high prevalence of fatigue in RA, the role of other factors is still unclear. Thus, we aimed to find the association between physical and mental health with fatigue, controlling for sociodemographic variables and disease duration. This study also aimed to try to determine if there are differences between these factors in Slovak and Greek patients, and also measured which patients’ group will report higher levels of fatigue.
METHODS
Sample and Procedure
The study sample was recruited at the outpatient department of rheumatology of Louis Pasteur University Hospital in Kosice, Slovakia and Municipal Clinics of the Municipality of Iraklio Attica - Athens, Greece. Inclusion criteria for participating in the study were diagnosed with RA based on the criteria of the American College of Rheumatology published in 1987 [15]. Patients who were younger than 18 years, had the existence of another physical handicap before RA and were not able to understand Slovak or Greek language were excluded from our study. Patients signed an informed consent form before the study and their participation was voluntary. The study followed Good Clinical Standards and the Helsinki Declaration.
RA patients willing to participate were asked questions about their sociodemographic background and disease duration and completed questionnaires. In total 402 Slovak patients were found to be eligible for the study, of which 105 refused to participate. The response rate of Slovak patients was 73.8%. In total 51 Greek patients were asked to participate in the study and none of them refused. The response rate of data collected in Greece was 100%. The final sample consisted of 348 patients, so the total response rate was 76.8%.
Measures
Visual Analogue Scale for fatigue
The Visual Analogue Scale (VAS) is used as an instrument for the measurement of subjective and behavioral experiences. The higher scores mean a greater level of measured variable [16]. In our case, it is used for the measurement of the intensity of fatigue.
The 36-Item Short Form Health Survey
The Short Form Health Survey 36 (SF-36) was used to evaluate how patients perceive their health status, both physically and mentally. SF-36 consist of 36 items, which are divided into 8 subscales: physical functioning, bodily pain, role limitation due to physical health, general health, vitality, social functioning, role limitation due to emotional problems, and mental health. Two summary scores can be calculated: Physical Component Summary (PCS) and Mental Component Summary (MCS). The scores range from 0-100, with higher scores meaning better physical or mental health [17]. SF-36 can be used for different patient groups' data; thus, it allows us to use it across-disease groups and in our case as a cross-country comparison.
Sociodemographic data and disease duration
Socio-demographic data were collected via an interviewer and provided basic information about gender, age, and education. Patients indicated their highest level of education achieved and it was categorized into elementary, secondary and university education. Responses to questions on disease duration were completed by the patients together with the questionnaires.
Statistical analyses
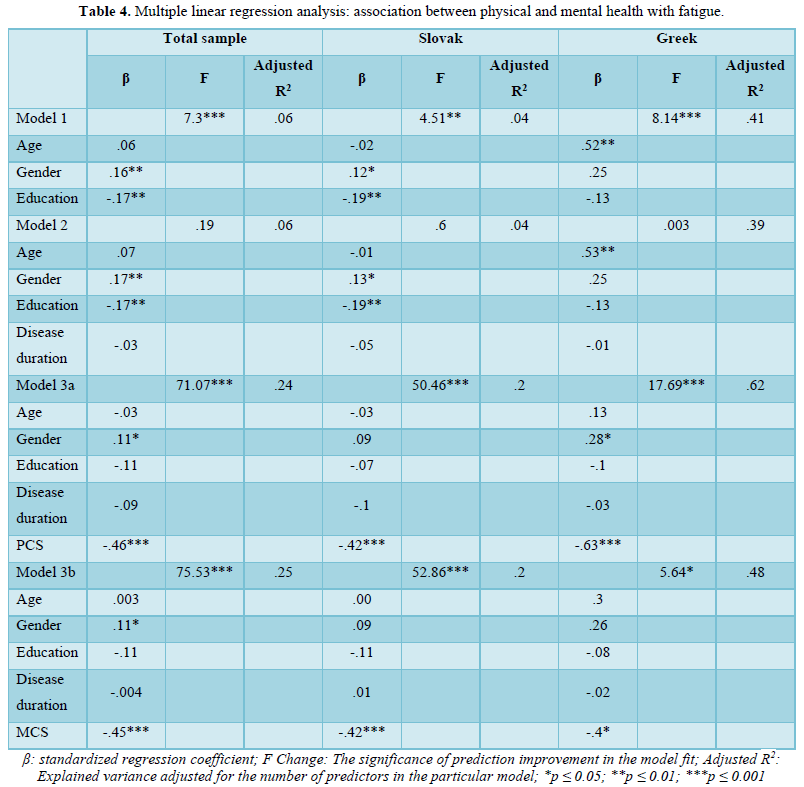
For our study, several statistical methods were used to analyze the available data. For sociodemographic data, disease duration, PSC, MSC and experience level of fatigue descriptive statistics were used. The second step was correlations of factors under study with fatigue. Lastly, we applied the enter method in the linear regression to determine the associated between physical and mental health with fatigue, controlled for sociodemographic variables and disease duration. The first model of the variables included sociodemographic data such as age, gender and education. The second model included disease duration. The final, third model included research factors that are associated with fatigue. Results were displayed for Slovak RA patients, Greek patients and patients from both countries together (total sample). All analyses were conducted using the statistical software package SPSS (version IBM SPSS 25). Multicollinearity levels over 2.5 were not present and the p-value of ≤0.05 was considered statistically significant.
RESULTS
Sample characteristics
The total sample was 348 RA patients (Table 1).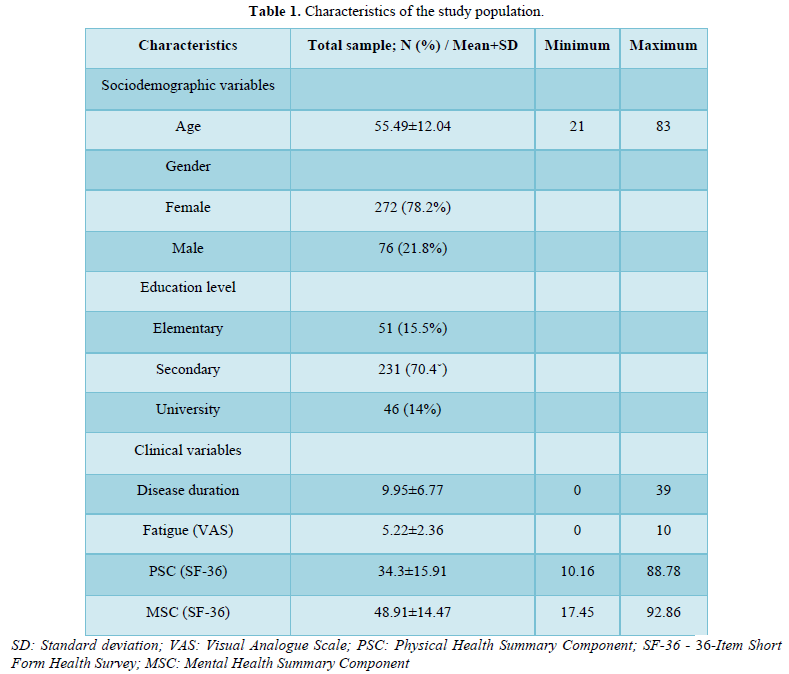
The study includes 297 patients (85.3%) from Slovakia and 51 (14.7%) from Greece. Participants were predominately females 272 (78.2% in the total sample) compared to males 76 (21.8%) as shown in Table 2.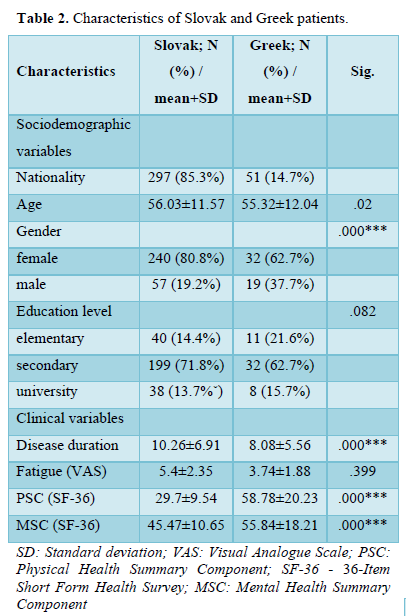
As shown, there was a significant difference in the percentage of females RA patients in Slovakia (80.8%) and Greece (62.7%). The mean age of the total sample was 55.49 years with a standard deviation (SD) of ±12.04 years, and the range of the youngest patient was 21 years old to the oldest 83 years old. The Slovak patients had a mean age of 56.03 with SD ±11.57 years. The Greek patients were significantly younger with a mean age of 52.32 and SD ±14.21 years. Achieved education level in the total sample was 51 patients finished elementary education (15.5.%), secondary accomplished 231 patients (70.4%) and university degree obtained 46 patients (14.0%). There are differences between achieved education in both countries but they are not significant. More Greek patients finished just elementary education (21.6%) compared to Slovak patients (14.4%). The Slovak patients achieved more secondary education (71.8%) compared to the Greeks (62.7%). The university degree had a similar percentage of RA patients in Greece (15.7%) and Slovakia (13.7%). The mean disease duration in our total sample was 9.95 years with SD ±6.77 of a minimum of 0 years and a maximum of 39 years. Disease duration in Slovak RA patients was 10.26 ±6.91 years significantly higher compared to Greek patients who reported duration of disease of 8.08 ±5.56 years. The fatigue we measured with VAS-fatigue. In the total sample was mean of VAS fatigue was 5.22 SD ±2.36. Table 2 shows a significantly higher level of fatigue in Slovak RA patients (mean of VAS-fatigue 5.40 SD ±2.35) compared to Greek patients (mean of VAS-fatigue 3.74 SD ±1.88). There were also significantly different levels of PCS and MCS in both countries, with better results in Greek patients (PCS: 58.78±20.23; MCS: 55.84±18.21) compare to Slovak RA patients (PCS: 29.7±9.54; MCS: 45.47±10.65).
Correlations between sociodemographic variables, disease duration, physical and mental health with fatigue
Our results have shown a significant association between gender and fatigue in the total sample of both countries and Slovak patients, with greater fatigue in female patients. There was no significant association between gender and fatigue in Greek RA patients. Our results have displayed a significance between age and fatigue in the total sample of both countries and strong significance in the Greek patient's sample, with older patients experiencing higher levels of fatigue. There was no significance in Slovak RA patients between age and fatigue. Our results have shown a strong significant association between education and fatigue in the total sample of both countries and Slovak RA patients. Greek patients expressed education in significant association with fatigue too, but it was not that strong relationship. Patients with lower education had greater fatigue (Table 3).
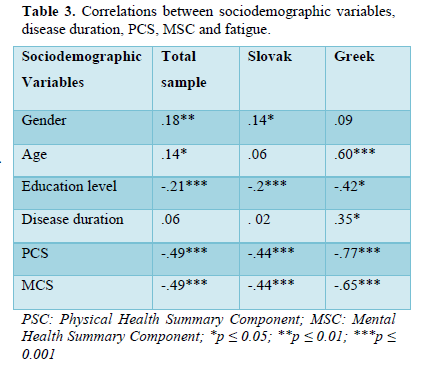
Table 3 also demonstrates the significant relationship between disease duration and fatigue, but only in Greek patients, where patients with you suffer RA longer reported higher fatigue. There is no significance in the total sample and Slovak patients in disease duration and fatigue. The PCS and MCS showed a strong significant association between them and fatigue in Slovak, Greek and total sample, with patients that reported lower physical or mental health experience greater fatigue.
The association between physical health and fatigue
To measure the association between physical health and fatigue, we used VAS-fatigue and PSC from the SF-36 questionnaire. Table 4 shows there was a strong significance between physical health and fatigue (p ≤ 0.001) in Model 3a in Slovak patients, Greek patients and also in patients from both countries together. The final regression model explained between 20-62% of the total variance for our samples.
DISCUSSION
In this study, we aimed to evaluate the factors associated with fatigue and to compare the results gathered from the Slovak and Greek patients on those factors. Higher reported levels of fatigue were in Slovak patients, but it was not significantly different. In correlation analyses, we found lower education levels, and worsened physical and mental health associated with higher fatigue in the total sample, and also in Slovak and Greek RA patients. The physical and mental health stayed significantly associated with fatigue also in the regression analyses. Gender was significantly associated with fatigue in the total sample and Slovak patients in correlation. A significant association between age and fatigue was found in the total sample and Greek patients. The disease duration correlated weakly with Greek patients. In our results, we found that Slovak RA patients suffer more from fatigue compared to Greek patients. Patients from both countries were of similar age, but only in Greek patients it plays a significant role, and older patients reported higher fatigue. On the other hand, the female gender was significantly associated with greater fatigue only in Slovak and not in Greek patients. However, the physical and mental score was higher in Greek patients, which may be explained by the higher average life expectancy of Greeks (83 years) as compared to Slovaks, whose life expectancy is 78 years on average [18]. Another possible reason might be the cultural differences in lifestyles between Slovaks and Greeks. Greek people live in a good climate, with a high temperature and sun most days, allowing them to go out and socialize with other people more, eating mostly a Mediterranean diet [19]. It could be also explained by clinical status, but in our study, we didn't have data collected about disease activity, functional disability, comorbidities, or type of pharmacological treatment, that can influence the overall quality of life in RA patients [4,12,20], so future research is needed. In some sociodemographic data, we found discrepancies in association with fatigue in our sample compared to earlier studies. Gender has been shown to have strong significance in the correlation in our total sample of both countries and also significant in Slovak RA patients, but not in Greek patients. In the final regression model, it was significant with fatigue only in the total sample. There was a significant difference in the percentage of female patients in both countries and Greek patients were only 62.7% of females in compared to 80.8% in the Slovak sample. Nevertheless, fatigue is typically associated with the female gender [1,3], but there were studies where that did not find this significance [21,22], so future research on the subject is needed for a clearer conclusion. Age as a predictor of fatigue was significant in our total sample and was also reported as strongly significant in Greek RA patients. The regression model was age significant only in the first two models and after when physical or mental health was added it lost its significance. The Slovak group of patients did not show a relationship between age and fatigue. Therefore it seems that older age is not that strongly associated with higher levels of fatigue as previously stated [12]. Age was often connected with fatigue due to ageing, and as people get older easier they get tired, so strategies for healthy ageing are needed [23]. However, some studies found also that younger age is associated with fatigue in RA patients [20,24], so fatigue can be prevalent at any age and more studies further into the topic are required. The educational levels were found to be significantly associated with fatigue in the total sample, as well as in both of the samples separately. In the regression models, it lost its significance. There was also no statistical difference between achieved education in Slovak and Greek patients. This finding was in the line with previous studies where lower education was associated with higher experience fatigue in RA patients [13,14]. Our results showed that disease duration is not a major factor in a strong association with fatigue. Only the Greek patients showed a significant, but weak correlation between disease duration and fatigue and it was not significant in any regression model. We found fewer studies confirming this association [25], as those which do not support an association between disease duration and fatigue and RA patients experience fatigue in any stage of the disease [12,26]. In our study, we found a strong association between physical health and fatigue in Greek, Slovak and also the total sample. Also, regression analyses support our findings about the significant association, which is in the line with previous studies [8]. Studies showed that regular physical activity can help to reduce fatigue [4,8]. However, the study found that the physical impact on the health of RA patients is also a barrier to physical activity because is extremely tiring for the patient [7]. Based on those findings, we can conclude that it is a vicious circle for RA patients, making it even more important for healthcare professionals to highlight the importance of exercise and motivate patients. Also, mental health was found to be strongly associated with correlation and also in regression analyses in Slovak, Greek and the total sample. This association is particularly important because poor mental health in RA patients exacerbates fatigue severity [4,9,10,20]. Especially in the post-pandemic situation is important to focus on psychological stress in patients due to the higher prevalence caused by the COVID-19 pandemic [27,28]. It was also found that high levels of physical activity, not only reduced fatigue, but patients have more positive moods [29]. Another study described a cultural difference in fatigue association and in some countries, fatigue was mainly related to physical impact and rarely to mental [30]. As a result, when developing non-pharmacological interventions for fatigue, it is critical to keep cultural differences in mind.
STRENGTHS AND LIMITATIONS
The strength of our study is the comparison of two culturally different samples of RA patients. Also, our results confirm the importance of measuring fatigue during patients' rheumatology visits, due to its high prevalence. We examined the association with not only physical but also psychological factors. Furthermore, results imply that fatigue is affected by different factors, which should be taken into account when non-pharmacological interventions are developed. Lastly, our study had a high response rate of 76.8% (100% in the Greek sample and 73.8% in the Slovak sample). It is important to notice that we compared only 51 Greek patients with 297 Slovak patients. Using these numbers for comparison creates some limitations, because of the large size difference between the number of patients in each country sample. In later years it is hoped that a study of higher numbers of Greek patients should be conducted. Another limitation is the small number of male patients, which is typical for RA, and future research with more male patients is needed. Also, we didn't collect data about the patient's clinical status or pharmacological treatment, which may affect the study results.
CONCLUSION
The results revealed a statistically significant association between physical and mental health and fatigue. We also found differences in factors related to fatigue among nationalities. We focused on sociodemographic data such as gender, age, education, disease duration, and physical and mental health. In light of this data, it is suggested that fatigue, as one of the most common RA symptoms, has a multidimensional nature and should be considered and treated in accordance with its determined origins. It is also critical that physicians consider the mental health status of their patients when treating fatigue because it has been shown to be connected, so focusing solely on physical health is not enough. It is essential to consider multiple management options (non-pharmacological interventions) in order to improve morbidity, holistic health care services and the general improvement of the quality of life of the patients. Because of the contradictions in our findings and other pre-existing literature, more research on the factors that influence fatigue is needed. It may also be beneficial to research various domains of fatigue to determine which factors are associated with them and how they affect RA. Finally, based on our findings, we believe that more studies comparing patient samples from different countries would be beneficial in understanding how cultural background influences fatigue in RA patients.
- Pope JE (2020) Management of Fatigue in Rheumatoid Arthritis. RMD Open 6(1): 1-9.
- Latocha KM, Loppenthin KB, Ostergaard M, Jennum PJ, Christensen R, et al. (2020) Cognitive behavioural therapy for insomnia in patients with rheumatoid arthritis: Protocol for the randomised, single-blinded, parallel-group Sleep-RA trial. Trials 21(1): 440.
- Espinoza G, Maldonado G, Narvaez J, Guerrero R, Citera G, et al. (2021) Beyond Rheumatoid Arthritis Evaluation: What are We Missing? Open Access Rheumatol 13: 45-55.
- Katz P (2017) Fatigue in Rheumatoid Arthritis. Curr Rheumatol Rep 19(5): 25.
- Tournadre A, Pereira B, Gossec L, Soubrier M, Dougados M (2019) Impact of comorbidities on fatigue in rheumatoid arthritis patients: Results from a nurse-led program for comorbidities management (COMEDRA). Joint Bone Spine 86(1): 55-60.
- Choy EH (2019) Effect of biologics and targeted synthetic disease-modifying anti-rheumatic drugs on fatigue in rheumatoid arthritis. Rheumatology 58: v51-v55.
- Primdahl J, Hegelund A, Lorenzen AG, Loeppenthin K, Dures E, et al. (2019) The Experience of people with rheumatoid arthritis living with fatigue: A qualitative metasynthesis. BMJ 9(3): e024338.
- Louati K, Berenbaum F (2015) Fatigue in chronic inflammation-a link to pain pathways. Arthritis Res Ther 17(1): 1-10.
- Bianchi WA, Elias FR, Pinheiro G, Gayer CRM, Carneiro C, et al. (2014) Analysis of the association of fatigue with clinical and psychological variables in a series of 371 Brazilian patients with rheumatoid arthritis. Revista Brasileira de Reumatologia (English Edition) 54(3): 200-207.
- Druce KL, Basu N (2019) Predictors of fatigue in rheumatoid arthritis. Rheumatology 58: v29-v34.
- Gossec L, Ahdjoudj S, Alemao E, Strand V (2017) Improvements in fatigue in 1536 patients with rheumatoid arthritis and correlation with other treatment outcomes: A post hoc analysis of three randomized controlled trials of abatacept. Rheumatol Ther 4(1): 99-109.
- Uhlig T, Provan SA (2018) Treating Fatigue in Rheumatoid Arthritis: Does Patient Age Matter? Drugs Aging 35(10): 871-876.
- Esbensen BA, Stallknecht SE, Madsen ME, Hagelund L, Pilgaard T (2020) Correlations of fatigue in Danish patients with rheumatoid arthritis, psoriatic arthritis and spondyloarthritis. PLoS One 15(8): e0237117.
- Lapcevic M, Vukovic M, Gvozdenovic BS, Mioljevic V, Marjanovic S (2017) Socioeconomic and therapy factor influence on self-reported fatigue, anxiety and depression in rheumatoid arthritis patients. Rev Bras Reumatol Engl Ed 57(6): 545-556.
- Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, et al. (1988) The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 31(3): 315-324.
- Wewers ME, Lowe NK (1990) A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Health 13(4): 227-236.
- Ware JE, Sherbourne CD (1992) The MOS 36-Item Short-From Health Survey (SF-36). Med Care 30(6): 473-483.
- Worldometer (2020) Demographics. Avalible online at: https://www.worldometers.info/demographics/
- Simopoulos AP (2001) The Mediterranean diets: what is so special about the diet of Greece? The scientific evidence. J Nutr 131(11): 3065S-3073.
- Van HD, Fransen J, Bleijenberg G, Van RP (2010) Physical and psychosocial correlates of severe fatigue in rheumatoid arthritis. Rheumatology 49(7): 1294-1302.
- Stebbings S, Herbison P, Doyle TC, Treharne GJ, Highton J (2010) A comparison of fatigue correlates in rheumatoid arthritis and osteoarthritis: Disparity in associations with disability, anxiety and sleep disturbance. Rheumatology 49(2): 361-367.
- Davis MC, Okun MA, Kruszewski D, Zautra AJ, Tennen H (2010) Sex differences in the relations of positive and negative daily events and fatigue in adults with rheumatoid arthritis. J Pain 11(12): 1338-1347.
- Soutschek A, Bagaïni A, Hare TA, Tobler PN (2022) Reconciling psychological and neuroscientific accounts of reduced motivation in aging. Soc Cogn Affect Neurosci 17(4): 398-407.
- Olsen CL, Lie E, Kvien TK, Zangi HA (2016) Predictors of Fatigue in Rheumatoid Arthritis Patients in Remission or in a Low Disease Activity State. Arthritis Care Res (Hoboken) 68(7): 1043-1048.
- Szady P, Baczyk G, Kozlowska K (2017) Fatigue and sleep quality in rheumatoid arthritis patients during hospital admission. Reumatologia 55(2): 65-72.
- Silva CF, Catia D, Ricardo JO, Eduardo S, José A, Pereira S (2019) Depression, disability and sleep disturbance are the main explanatory factors of fatigue in rheumatoid arthritis: A path analysis model. Clin Exp Rheumatol 38: 314-321.
- Itaya T, Torii M, Hashimoto M, Tanigawa K, Urai Y, et al. (2021). Prevalence of anxiety and depression in patients with rheumatoid arthritis before and during the COVID-19 pandemic. Rheumatology 60(4): 2023-2024.
- Bhatia A, Kc M (2021) Increased risk of mental health disorders in patients with RA during the COVID-19 pandemic: A possible surge and solutions. Rheumatol Int 41(5): 843-850.
- Sturgeon JA, Finan PH, Zautra AJ (2016) Affective disturbance in rheumatoid arthritis: Psychological and disease-related pathways. Nat Rev Rheumatol 12(9): 532-542.
- Mortada M, Abdul SA, Gossec L (2015) Fatigue in Egyptian patients with rheumatic diseases: A qualitative study. Health Qual Life Outcomes 13: 134.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4




QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Journal of Allergy Research (ISSN:2642-326X)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Pathology and Toxicology Research
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)


