Journal of Nursing and Occupational Health (ISSN: 2640-0845)

Research Article
Effectiveness of Motor Stimulation Exercises and Adaptive Coping Towards Functional Capacity on Post Stroke Patients
4193
Views & Citations3193
Likes & Shares
Background: Stroke is a type of disease that attacks the nervous system of humans because of damage to nerve cells in the brain due to disruption of blood supply to parts of the brain. Stroke has a physical and psychological impact. The most common physical problem in post-stroke patients is hemiparesis which can reduce the quality of life for post stroke patients. A therapy which can be given is the motor stimulation exercises and the adaptive coping.
Objective: To know the influence of motor stimulation exercises and adaptive coping towards functional capacity on post stroke patients in Sultan Sharif Mohamad Alarie General Hospital Pontianak.
Methods: Quantitative research through the quays experiment research design of pretest- posttest definition with control group. The method of sampling is non-probability sampling with the consecutive sampling technique. The research participants are 30 respondents. The data tested with the Wilcoxon test, and man Whitney test.
Result: The bivariate results of the functional capacity of the intervention group found that the mean pre-test 52.67 and post-test 79.33 showed that there was a significant effect of motor stimulation and adaptive coping exercises (p <0.05), but there was no difference in post-test functional capacity values between the intervention groups were given motor stimulation exercises and adaptive coping with the control group given motor stimulation exercises (p> 0.05).
Conclusion: The influence of motor stimulation and adaptive coping exercises on increasing functional capacity in post-stroke patients.
Keywords: Motor stimulation exercises, Adaptive coping, Functional capacity
PRELIMINARY
Stroke is a disease that causes death and disability worldwide. The American Heart Association / American Stroke Association (AHA / ASA) in heart disease and Stroke Statistics-2017 Updates, states that in America an average of every 40 seconds a person experiences a stroke and every 4 min someone dies of a stroke [1]. In 2013, the prevalence of stroke in the world amounted to 25.7 million people with stroke (71% due to ischemic stroke), 6.5 million people died from stroke (51% due to ischemic stroke), 113 million people experiencing disabilities due to stroke (58% ischemic stroke), and 10.3 million people as new cases of stroke sufferers (67% ischemic stroke) [2]. Ischemic stroke is more common than hemorrhagic stroke [3]. Basic Health Research states that the prevalence of stroke based on diagnosis by health professionals in Indonesia increased from 7 per mile in 2013 to 10.9 per mile based on doctor's diagnosis in 2018 in a population greater than 15 years [4]. West Kalimantan recorded 5.8 per mile for patients diagnosed by health professionals and 8.2 per mile for diagnosed and symptomatic strokes by health workers in 2013. Stroke has an impact that can affect a person's activities, for example making a person insecure, lowering productivity, losing enthusiasm for hobbies and many others. The impact after stroke is communication problems, emotional disturbances, pain, sleep disturbances, dysphagia, paralysis and disability, so that it can interfere with the ability of daily activities causing stroke sufferers to experience depression [5]. The most common physical problem in post-stroke patients is hemiparesis in the upper and lower extremities. Regarding these physical problems, there is rehabilitation program to overcome or restore physical function in post-stroke patients [6]. Rehabilitation is a basic therapy program for recovery of stroke patients who have impaired motor function. Post-stroke rehabilitation can be done in various methods such as electrotherapy, hydrotherapy, exercise therapy. Rehabilitation exercise therapy needs to be given to post-stroke patients in increasing motor strength to carry out daily activities [7]. Exercise therapy is expected to restore motor function in post-stroke patients to optimize function so that they can be independent in carrying out daily activities. The practice itself can use a rubber ball as an intervention [6]. Exercises that stimulate the movement of the hands can be in the form of exercising the function of gripping the fists tightly by moving the muscles to help regain control of the brain over these muscles [8]. Spherical grip techniques can be used to aid in the recovery of the arm or upper limb. The spherical grip exercise is a functional hand exercise by grasping a round object such as a ball in the palm of the hand [9]. To strengthen patient motivation to exercise in increasing functional capacity and to independent post- stroke patients in their daily activities, it is necessary to provide training in implementing post-stroke adaptive coping. This adaptive coping support encourages stroke patients to quickly adapt to existing stressors and restore optimal function after stroke [10]. Adaptive coping can support the acceleration of the rehabilitation process both physically and psychologically [11]. Coping strategies are associated with social support and affect emotional aspects. The support obtained from the family is a resource that assists patients in disease management. Another factor that influences coping strategies is individual personality traits. So that post-stroke patients can be trained to use effective coping strategies to improve the process of receiving the consequences of stroke and improve the quality of life [12]. Research conducted by Olivanic at RSUD Uline Banjarmasin in 2017 showed that out of a total of 30 respondents, 25 respondents experienced an increase in upper limb muscle strength in stroke patients after being given Range of Motion (ROM) Spherical Grip exercises [13]. A preliminary study conducted by researchers at the Sultan Syarif Mohamad Alkadrie Regional Hospital in Pontianak City with observation and interviews of nurses who served in the inpatient room. The results of interviews conducted with nurses, nurses said that strokes were among the [10] biggest diseases that occurred in the Sultan Syarif Mohamad Alkadrie Regional Hospital in Pontianak City and most of them showed sequelae such as hemiparesis. Rehabilitation that has been carried out by patients in the form of physiotherapy and traditional massage to deal with weaknesses suffered. From the above problems, the researcher is interested in conducting a study with the title of the effectiveness of motor stimulation exercises and adaptive coping on functional capacity in post-stroke patients at Sultan Syarif Mohamad Alkadrie Hospital, Pontianak City.
METHOD
This study used a quays experimental research design pre-posttest design with nonequivalent control group. The intervention group was given motor stimulation exercises and adaptive coping for 30 min a day, for 10 days. The pre-test was carried out on the first day and the post-test was carried out on the tenth day. The control group was only given motor stimulation exercises for 30 min a day for 10 days. The pre-test was carried out on the first day and the post-test was carried out on the tenth day. A sample of 30 post- stroke patients was obtained by consecutive sampling at RSUD Sultan Syarif Mohamad Alkadrie Pontianak City. The inclusion criteria in this study are; post-stroke patients in the rehabilitation phase, copayments awareness, vital signs in a stable condition, and experiencing hemiparesis. The exclusion criteria in this study were; severe stroke sufferers with complex disabilities, stroke survivors who have severe cognitive impairment, stroke survivors who have injuries to the extremities. The research instrument used was a Barthel index questionnaire to measure the value of functional capacity. The sample was divided into two groups, 15 people in the intervention group and 15 people in the control group. The statistical analysis used was univariate and bivariate.
RESULTS
- Univariate Analysis
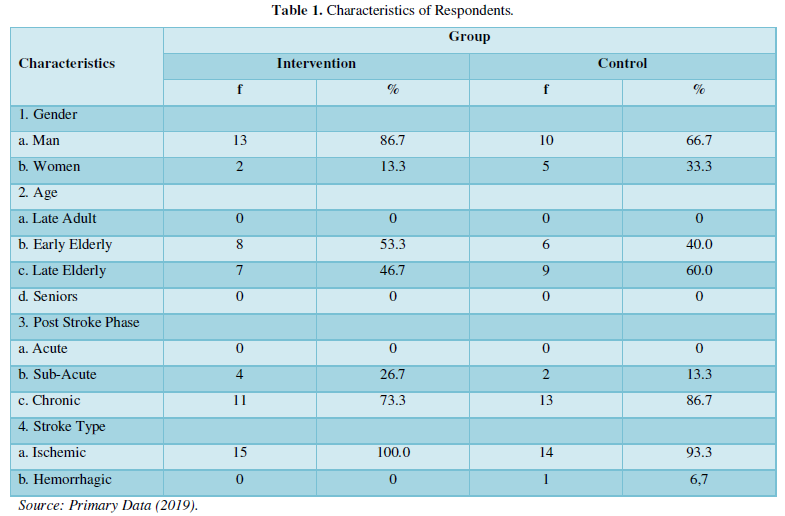
Table 1 show Characteristics of respondents in this study note that respondents in the intervention group were male (86.7%) and female (13.3%). In the control group, the sexes were male (66.7%) and female (33.3%). Based on the age of the intervention group, early elderly (53.3%), and late elderly (46.7). Control group early elderly (40%), and elderly (60%). Based on the post-stroke phase of the sub-acute (26.7%) and chronic (73.3%) intervention group. Sub-acute (13.3%), and chronic (86.7%) control groups. Type of stroke in the ischemic intervention group (100%). The control group was hemic (93.3%) and hemorrhagic (6.7%) stroke type.
- Bivariate Analysis
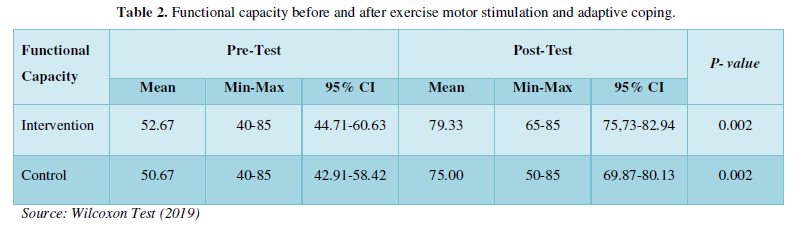
Before the bivariate analysis was carried out, the normality test was carried out which is a requirement for paired t test and unpaired t test data distribution is not normal with a significant value (p <0.05), so it can use the Wilcoxon test and the Mann Whitney test. Results Table 2 shows the results of the Wilcoxon statistical test in the intervention group obtained p value of 0.002 (p <0.05), which means that there is an effect of the value of functional capacity before the intervention of motor stimulation and adaptive coping exercises and after the intervention of motor stimulation exercises and adaptive coping. In the control group obtained p value 0.002 (p <0.05), which means there is an effect of the value of functional capacity before and after being given motor stimulation exercises. So, it can be concluded that there is an influence significant value of functional capacity between pre-test and post-test in both groups.
Table 3 shows the results of the Mann Whitney statistical test the pre-test functional capacity value between the intervention group and the control group obtained p value = 0.824 which means there is no difference in the pre-test functional capacity value between the intervention group and the control group (p> 0.05). The post-test functional capacity value between the intervention group and the control group obtained p value = 0.098, which means there is no difference in the post-test functional capacity value between the intervention group and the control group (p> 0.05). From Table 3 it can be concluded that there is no significant difference in the value of functional capacity between the intervention group and the control group both in the pre- test and post-test.

DISCUSSION
Motor stimulation exercises are one of the post-stroke rehabilitation methods to increase muscle strength and the ability to perform certain movements in the upper extremities. The results of this study found that there was a difference in the value of functional capacity between the pre-test and post-test in the intervention group and the control group. Joshi states that grip strength correlates with upper limb function and the proximal stability provided by the shoulder girdle. There is a positive correlation between hand grip activity and rotator cuff muscle activity. Hand holding activity and Grip strength is used to assess the overall functional capacity of the upper limb. Because the function of the hand (prehension activity) is the most important part of the function of the upper limb in our daily life. Thus, in upper limb rehabilitation, grip strength is used as a parameter to examine the progress or effectiveness of exercise that affects the upper limb function and ADL of chronic stroke patients [14]. In line with Horsley stated that there is a correlation between grip strength and scapular muscle strength. The representative function of the hand is to hold something. The force of the finger when holding onto something is known as grip strength and it is important in the evaluation of the motor function of the hand. Because grip strength is very positively correlated with muscle strength. grip strength can be used to evaluate changes in muscle strength effectively and economically. Grip strength has been used in many studies because of its simple measurement. Grip strength is not only the force generated by the fingers and wrist joints, it is also closely connected to the muscle strength of the forearm, and the brachial and shoulder joints [15]. This research is in line with Hentu There was an increase in the value of muscle strength after ROM exercise and rubber ball movement, where the mean value increased to 14.93 in the intervention group and 13.00 in the control group. The rubber ball used in this study is a rubber ball with a serrated and flexible surface. This proves that the provision of ROM exercises and rubber ball movements are effective in increasing the value of muscle strength6. The increase in muscle strength that occurs due to routine exercise performed by respondents can have an impact on enlarging muscle fibrils. So, with frequent exercises to enlarge muscle fibrils also get bigger. The practice of gripping the rubber ball on your own can help regain control in the brain and this exercise will stimulate muscle fibers to contract more. The rubber ball motor stimulation exercise mechanism is a modality of fine touch and pressure sensory stimulation at the end of the encapsulated organ tip receptors in the extremities. The response that will be conveyed to the sensory cortex in the brain is the sensory pathway through the cell body on the C7-T1 nerves directly through the limbic system. The processing of existing stimuli causes a rapid response to the nerves to take action on these stimuli. Fine sensory stimuli and pressure will be processed in the sensory cortex which then impulses are channeled into the motor cortex. The impulses that form in the second motor neurons in the cranial nerve nuclei and anterior horn of the spinal cord travel through the anterior roots, nerve plexuses (in the cervical and lumbosacral regions), and peripheral nerves on their way to the skeletal muscles. The impulses are conveyed to the muscle cells via the motor end plate neuromuscular link then there will be muscle movement in the extremities. This mechanism is called feedforward control in response to pressure stimulation and gentle touch on the rubber ball [9]. Prok's research shows that the muscle strength before doing the ball gripping exercise is 2-24 kg with an average of 10.56 and after doing the ball gripping exercise it increases to 4-29 kg with an average of 14.06. hand-held therapy slowly recovered from the stroke they suffered, this shows that the activation of neural networks is use- dependent, the more often it is used, the stronger it is and the more synapses are formed9. From the research results obtained, the researcher argues that motor stimulation exercises carried out can increase functional capacity due to the process of regular motor training that experiences hemiparesis by stimulating the motor center in the brain so that it triggers normal motor activity, especially for movement. The process of movement that is carried out also increases muscle mass and improves blood circulation which functions to improve motor skills. This study uses adaptive coping support to influence patients in accepting post-stroke patients for their condition. Increase patient motivation to do exercises with a desire to recover quickly post-stroke coping is a process of controlling stressors or stimuli by the patient to maintain his integrity and restore optimal function after stroke. The adaptive coping mechanism to the stimulus will produce an adaptive behavioral response after stroke [10]. Adaptive coping also has an impact on the health process of post-stroke patients. The health of post-stroke patients has improved because of the self-acceptance response to the pain suffered. The self- acceptance response is in the form of being realistic, clever in taking lessons, and fortitude. The response shown to the patient's physical form is stable breathing, looks calmer, and the healing process is faster than the time it should be [11]. This raises a strong hope and desire to continue this life by continuing to carry out the treatment process and rehabilitation program so that there can be an increase in functional capacity [16]. Researchers argue that motor stimulation exercises and adaptive coping have the effect of motivating patients to undergo rehabilitation to increase muscle strength. Increased muscle strength can increase the patient's functional capacity to meet basic needs so that the quality of life will improve. From the results obtained, it was concluded that there was no difference in the value of functional capacity between the intervention group that was given motor stimulation exercises and adaptive coping support and the control group who was given motor stimulation exercises both in the pre-test and post-test. Stroke leaves residual symptoms, namely hemiparesis or hemiplegia which is caused by a blockage of the anterior and media cerebral arteries which causes an infection in the motor area of the frontal cortex. Hemiparesis or hemiplegia occurs contralaterally, infarction in the motor area of the cortex on the right cause’s hemiplegia to the left or vice versa [17]. Hemiparesis condition can reduce the quality of life of post-stroke patients because it is difficult to perform ADL independently and optimally. Coping strategies are associated with social and family support that affects emotional aspects. The support obtained from the family is a resource that assists patients in disease management. Another factor that influences coping strategies is individual personality traits [12]. Limitations in this study Researchers could not participate in motor stimulation and adaptive coping exercises every day, researchers followed only on day 1 and day 10. Researchers cannot observe any form of support assisted by family as a source of motivation, researchers cannot avoid family support because most respondents live with their families Researchers cannot control activities or activities that can increase the physical abilities that each respondent does in daily life -day, these activities are like doing traditional massage, exercises getting up from a sleeping position to a sitting position to a standing position, and walking exercises with arms on the weak side.
CONCLUSION OF ADVICE
Based on research and discussion on the effect of motor stimulation exercises and adaptive coping on the functional capacity of post-stroke patients in the working area of the Sultan Syarif Mohamad Alkadrie Regional Hospital, Pontianak City, it can be concluded: Characteristics of post-stroke respondents in the working area of the Sultan Syarif Mohamad Alkadrie General Hospital in Pontianak City based on gender, most of them were male, as many as 23 respondents (76.6%), based on the average age of stroke patients entering the elderly, based on the type of stroke, the most types of stroke were ischemic stroke as many as 29 respondents (96.6%) and based on the post-stroke phase most of the chronic phase was 24 respondents (80%). There was no difference in the pre-test functional capacity values between the intervention group and the control group. There are differences in the value of functional capacity in the intervention group and the control group before and after the measurement. There was no post-test difference in the functional capacity value of the intervention group and the control group. Researchers hope that further research can observe the duration of providing motor stimulation exercises and adaptive coping support, the post-stroke phase, and a longer evaluation time.
RECOMMENDATION
The results of this study can be useful for hospitals, especially in medical rehabilitation clinics that provide post-stroke rehabilitation services. The results of motor stimulation exercises and adaptive coping support can be an alternative post-stroke rehabilitation program in restoring extremity motor function. Patients and families can add knowledge and as an independent rehabilitation program carried out by patients and families.
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, et al. (2017) heart disease and Stroke Statistics-2017 Update: A Report from the American Heart Association. Circulation 135(10): e146-e603.
- Feigin VL, Norrving B, Mensah GA (2017) Global Burden of Stroke. Circ Res 120(3): 439-448.
- Venketasubramanian N, Yoon BW, Pandian J, Navarro JC (2017) Stroke Epidemiology in South, East, and South-East Asia: A Review. J Stroke 19(3): 286-294.
- Ministry of Health (2018) Basic Health Research 2018. Jakarta: Ministry of Health, Republic of Indonesia.
- Lingga L (2018) All About Stroke: Life Before and Pascastroke. Jakarta: Elex Media Komputindo.
- Hentu AR (2018) Effectiveness of Rom and Rubber Ball Exercises on Increasing Grasping Strength and Grasping Function in Stroke Patients at RSUD Sleman. Health Sci Media 7(2): 149-155.
- Winstein CJ, Stein J, Arena R, Bates B, Cherney LR, et al. (2016) Guidelines for Adult Stroke Rehabilitation and Recovery. Stroke J Am Heart Assoc 47(6): 68-169.
- Chaidir RZ (2014) Effect of Range of Motion Exercise on Upper Extremity with Rubber Balls on Muscle Strength of Non-Hemorrhagic Stroke Patients in Stroke Ward, RSSN Bukittinggi. pp: 1-6.
- Prok WG (2016) The Effect of Active Handling Ball Exercise on Stroke Patients Measured with a Handgrip Dynamometer in the Medical Rehabilitation of Prof. Dr. RD Kandaou Manado 2016. e-Clinic (Eci): 71-75.
- Dharma KK (2018) Family Empowerment to Optimize the Quality of Life of Post- Stroke Patients. Yogyakarta: Deepublish.
- Styana ZD (2016) Islamic Spiritual Guidance in Fostering Adaptive Spiritual Responses for Stroke Patients at the Jakarta Cempaka Putih Islamic Hospital. Dakwah Sci J 36(1): 45-69.
- Visser MM, Aben L, Heijenbrok-Kal MH, Busschbach JJV, Ribbers GM (2014) The relative effect of coping strategy and depression on health-related quality of life in patients in the chronic phase after stroke. J Rehabil Med 46: 514-519.
- Olviani YM (2017) Effect of Active-Assistive Range of Motion (ROM) Exercise on Increased Strength of Upper Extremity Muscles in Stroke Patients in the Inpatient Room for Neurological Diseases (Seruni) RSUD Ulin Banjarmasin. Health Dyn 8(1): 250-257.
- Joshi S, Sathe T (2018) Correlation Between Grip Strength and Scapular Muscle. Int J Adv Res Ideas Innov Technol 4(3): 2111-2117.
- Horsley I, Herrington L, Hoyle R, Prescott E, Bellamy N (2016) Do changes in handgrip strength correlate with shoulder rotator cuff function? Shoulder Elbow 8(2): 124-129.
- Omu O, Reynolds F (2014) Religious Faith and Self- Efficacy Among Stroke Patients in Kuwait: health professionals' views. Disabil Rehabil 36: 1529-1535.
- Price SA (2012) Pathophysiology of Clinical Concepts of Disease Processes 6th Jakarta: EGC.
-
 Table 1
Table 1 -
Table 2
-
Table 3



QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- BioMed Research Journal (ISSN:2578-8892)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Advance Research on Alzheimers and Parkinsons Disease
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)


