
4441
Views & Citations3441
Likes & Shares
Aim: This research was conducted as a descriptive-sectional research in order to determine the knowledge level of the nurses regarding the methods used in perioperative area cleaning to prevent surgical site infections.
Methods: The research data were obtained via face-to-face interviews with 87 nurses working in the operating room, intensive care, surgery and internal services of hospitals affiliated to a foundation university. The data were collected and evaluated statistically through the survey form prepared by the researcher after obtaining the permission of the institution and the ethics committee approval.
Results: While 60.9% of the nurses participating in the study had a bachelor's degree, 39.1% of them worked in the surgery service, 58.6% of them received training on preoperative patient preparation, the most common surgical site infection 77% of them encountered was superficial surgical site infection, 74.7% of them preferred the electric shaver the most in the perioperative area, 54% of them used the povidone iodine as the antiseptic solution for cleaning, 58.6% of them did not perform the area cleaning by himself/herself but was having it performed by a patient caretaker, 86.2% of them informed the patients. When the comparison of the scores of the information form on the preparation of the operation area was performed based on the occupational characteristics of the nurses, it was determined that the data form scores of those working in the mixed service were higher (p< .05).
Conclusion: It was concluded that the majority of the nurses encountered surgical site infection, received training on the subject, but fell short of reflecting the training received on practice. Therefore, it is recommended that the effectiveness of the training provided should be evaluated, the on-site practical training should be organized on subjects found to be incomplete and inadequate.
Keywords: Surgical site infection, area cleaning, nursing, preoperative preparation
INTRODUCTION
Surgery is one of the oldest practices in the history of medicine and is derived from the Latin term chirurgiae. It is based on surgical fixing of diseases, injuries, structural disorders in the body that do not heal through medication or other methods. Surgical treatment is one of the treatment methods that reduces mortality rate, lengthens the lifespan and improves quality of life in deviations from health. Today, scientific and technological advances have enabled the development of surgical treatment methods, accelerated the healing process, and become a life-saving treatment method for patients [1].
Surgical treatment, besides its planned and emergency types, is widely used for diagnostic, reconstructive, palliative and aesthetic purposes. The most important responsibility of the nurses involved in this process is the prevention of complications and improvement of the results by supporting the patient and family in pre-/intra and post-operative care [2]. A qualified preparation enables fewer complications, fewer complaints and earlier discharge of the patients from the hospital [3].
The period from the admission of the patients to the hospital until the operation is called the perioperative period. Within this period, the preparation of the patients as a whole in terms of physical, social and spiritual aspects is one of the most important stages of the process [3].
In a planned operation, the fact that the operation preparation is done in the best way and nursing care is well organized ensures the prevention of the complications that may occur during the postoperative period. The area cleaning that is not performed in the appropriate environment and with the appropriate method leads to the development of surgical site infection (the “SSI”) at the incision location. There are different methods of area cleaning. How and when these methods will be applied depends on the area that the surgical intervention will be performed [4].
The practices such as hair removal in the operation area, preoperative shower/bathing and using the antiseptic solution on the operating table are among the area cleaning methods The purpose of cleaning is to remove the temporary and permanent microorganisms and dirt from the surgical area and reduce the growth of microorganisms for a period of time. One of the important issues for the cleaning of the area is the protection of the skin integrity of the patient [5].
It has been found that skin cleansing made in an improper way increased the surgical site infection (the “SSI”) rate [6]. This situation prolongs the duration of the hospital stay of the patients and leads to deterioration of the quality of life. In addition, skin preparation and area cleaning affect the success of the surgical procedure [7].
The presence of hairs in the area where the surgery will be performed causes the incision line not visible adequately and makes the applications of suture and dressing difficult. In order to prevent these situations, the hairs in the region should be removed through the technique most appropriate for the patient. These techniques are the razor blade and electric shaver. Shaving with an open razor causes small cuts on the patient's skin and, also, creates an environment for the growth of microorganisms. The electric shavers contain disposable heads and causes less irritation than an open razor. When cutting the hairs, care should be taken to cut only the hairs that will affect the incision site. For this purpose, the surgical team members who are cleaning the area should know the hair removal techniques well [8].
The patient should take a shower after cleaning the area. Taking a shower before surgery allows the microorganisms in the body to decrease and move away. The shower should be taken with normal water and soap. Cleaning with the agents containing chlorhexidine gluconate, iodophor or hexachlorophene reduces the number of persistent microorganisms progressively. The patient should not use shampoo, hair conditioner or other hair care products while taking the shower before surgery. After the shower/bath, the body should be thoroughly rinsed and the clean clothes should be worn [9].
The cleaning of the area continues in the operating room as well. There are many antiseptic solutions used on the operating table for skin preparation. These solutions are approved by the Food and Drug Administration (the “FDA”) and accepted by the infection control committee of the health institution. When selecting a skin cleansing product, the appropriate solution for the normal skin pH value should be selected. It should also be easy to use and odorless. The antiseptic solution should not cause skin irritation or an allergic reaction. The cleaning solution should destroy the microorganisms in the fastest and most effective way and its effect should last throughout the surgery [10].
Prevention of surgical site infections is largely the responsibility of the surgical team and nurses working in the operating rooms. In order to prevent infections, it is very important that nurses take the necessary actions by making correct and true decisions and know the evidence-based recommendations [6,11].
SCOPE
The cleanliness of the surgical site is very important to prevent infections that may occur due to the surgical procedure. Informing the health workers about the subject starting from the school life period will allow the use of these methods more actively. In order to use the perioperative area cleaning during the preoperative patient preparation process, detailed studies are needed. It is considered that the results of this research will contribute significantly to the increase in the knowledge and awareness of nurses about the area cleansing.
RESEARCH QUESTIONS
In this study, the answers to the following questions were sought:
1. What are the methods used for perioperative area cleaning?
2. Do the nurses know the methods used for perioperative area cleaning?
3. Do the nurses know when the perioperative area cleaning should be performed?
4. Is there a difference between the knowledge levels of the nurses regarding the methods used in perioperative area cleaning based on their education, age, working experience and working time?
MATERIALS & METHODS
Aim of the study
This descriptive study was carried out for the ‘Assessment of Nurses’ Knowledge Level Regarding the Methods Used in the Perioperative Area Cleaning’ in the hospitals affiliated to a foundation university in Istanbul.
Population and sample of the study
The universe of the study consisted of nurses from 3 private hospitals. The sample consisted of nurses working in surgical and internal services, operating rooms, aged 18 and over, and agreed to participate in the study. In this context, 87 nurses working in relevant hospitals between 03.04.2019 - 03.05.2019 were included in the sample.
ETHICAL ASPECTS OF RESEARCH
Approval (30.01.2018/02-05) was obtained from Istanbul Bilim University Institute of Health Sciences Ethics Committee before starting the study. The permission of the institution was obtained for the application. The nurses who volunteered to participate in the research were informed regarding the purpose of the research, the facts that data obtained at the end of the evaluation would remain confidential and that they could withdraw from the research at any time they wish, and their voluntary consent was obtained.
Data collection
Data were collected between the dates 03.04.2019 and 03.05.2019 using the face-to-face interview method through the questionnaire consisting of ‘Nurse Information Form’ containing the socio-demographic characteristics of the nurses and the 'Information Form on the Preparation of the Operation Area' that was developed by the researcher. Each interview lasted approximately 15-20 min.
Data collection tools
The questionnaire, which was prepared by using the literature information [4,11-15] consisted of ‘Nurse Information Form’ containing the socio-demographic characteristics of the nurses and the ‘Information Form on the Preparation of the Operation Area’. In order to perform the study, the necessary approvals (30.01.2018/02-05) were obtained from 3 centers, where the study was performed, and Istanbul Bilim University Clinical Research Ethics Committee.
Statistical analysis
The data obtained from the study was analyzed statistically and interpreted. Descriptive statistics such as frequency, arithmetic mean, standard deviation and percentage were used in analyzing the data. In gap analyses, Mann Whitney-U test was used for two independent variables, Kruskal-Wallis test was used for more than two independent variables, and Spearman Correlation test was used for correlation analysis.
LIMITATIONS OF RESEARCH
One of the limitations of the study was that the study was carried out in 3 hospitals affiliated to a foundation university in Istanbul. The results can also be performed in other hospitals in Istanbul.
Besides obtaining the information regarding the area cleaning from the sample using the self-report method, the facts that the research design is in the descriptive type and that the practices regarding the subject of the nurses could not be observed in the clinical field are among the limitations of the research.
RESULTS
It was determined that the average age of the nurses participating in the study was 26.45 ± 5.888, 80.5% of them were female, 60.9% of them have bachelors' degree, their total working time was 5.46 ± 5.818 years, 39.1% of them were working in the surgical service, 20.7% of them in the operating room, the average working time in these units was 4.95 ± 5.644, the daily average of the number of patients prepared for the operation in the units they work is 5.36 ± 12.287, 58.6% of them received training on preoperative patient preparation, the most common surgical site infection 77% of them encountered is superficial surgical site infection.
It was found that 74.7% of the nurses who participated in the study prefer the electric shavers the most in the perioperative area cleaning, allocate 12.57 ± 15.076 minutes on average for cleaning, 66.7% of them did not follow the current publications about the area cleaning, 54% of them use the povidone iodine as the antiseptic solution for cleaning, 58.6% of them does not perform the area cleaning by himself/herself but have it performed by a patient caretaker, 86.2% of them informs the patients before the process (Table 1).
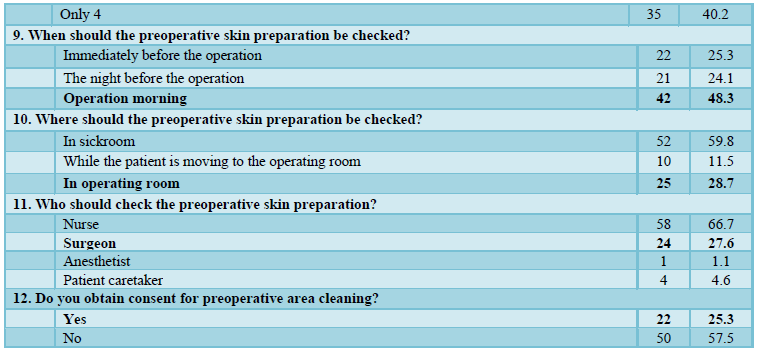
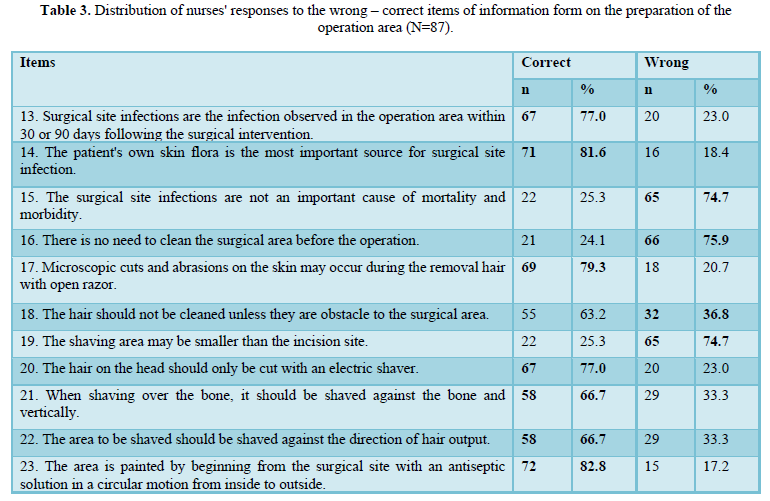
According to the information form on the preparation of the operation area, 57.5% of the nurses knew exogenous risk factors, 77% of them knew that washing hands is needed to prevent surgical site infections and the area should be cleaned immediately before the surgery, 55.2% of them knew that the body bath was should be performed on the morning of the operation, 25.3% of them stated that they obtained the consent of the patient before area cleaning, 48.3% of them performed the skin preparation check in the operation morning, and 28.7% of them stated that this control should be performed by the surgeons in the operating room. Also, it was found that 77% of the nurses knew that the surgical site infections could develop within 30 to 90 days after the surgery, 81.6% of them knew that the patient's skin flora is important in the formation of surgical site infection, and 79.3% of them stated that if an open razor is used for area cleaning that may cause the microscopic cuts and abrasions on the skin, and that the average score of the information form on the preparation of the operation area was 1.307 ± 2.766 (Tables 2 and 3).
When the comparison of the scores of the information form on the preparation of the operation area is performed based on the occupational characteristics of the nurses, it was found that there is a significant difference and the data form scores of those working in the mixed service were higher (p<0.05), whereas, no difference was determined in receiving training about the preoperative preparation, location of the training, duration of the training, following the current approaches regarding the perioperative area cleaning and the scores of the information form on the preparation of the operation area (p> 0.05) (Table 4).
DISCUSSION
Many factors originating from the hospital and health care workers cause surgical site infections. Among these factors, the level of education of the nurses providing the patient with the care service is an important factor. It is known that the nurses who have been trained in preparing the patients for the operation in the preoperative period are more successful in preventing surgical site infections. The age average and educational status of the 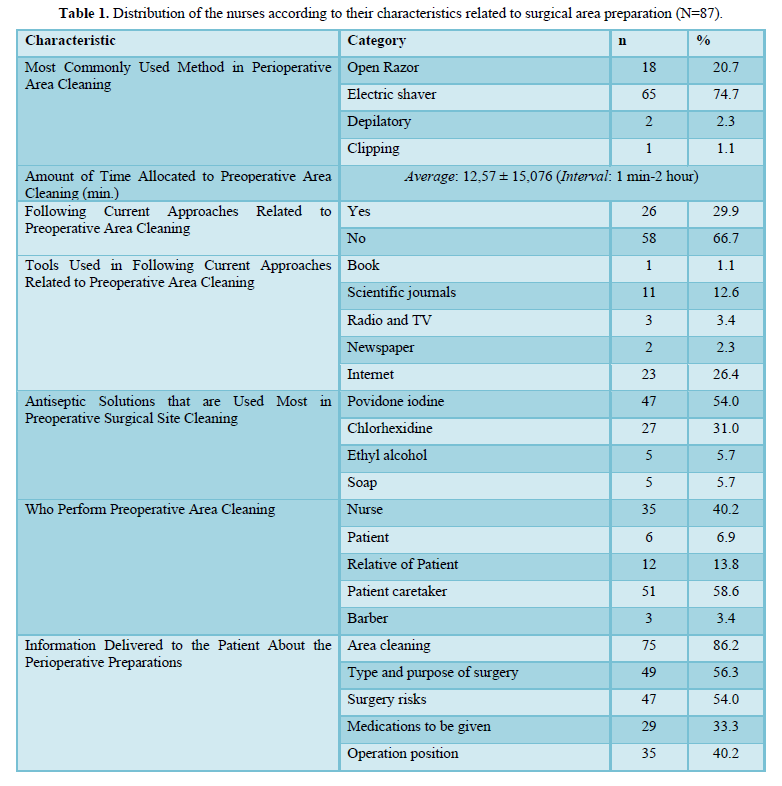
nurses are indicative of their professional experience and competency. As the average age increases, professional experience increases and the training received affects this experience positively. It was determined that 80.5% of the nurses participating in the study were women, their age average was 26.45 ± 5.888, 66.7% of them were single, 60.9% of them have bachelors’ degrees, their average total working time in the profession was 5.46 ± 5.818 years, their average working time in the unit where they worked was 4.95 ± 5.464, 14.9% of them was working in the internal service, 39.1% of them was working in the surgical service, 20.7% of them was working in the operating room, 19.5 % of them was working in the mixed service. In a study conducted [16], it was stated that the average of the service year of the nurses in the clinic they worked was 5.11 ± 3.93, 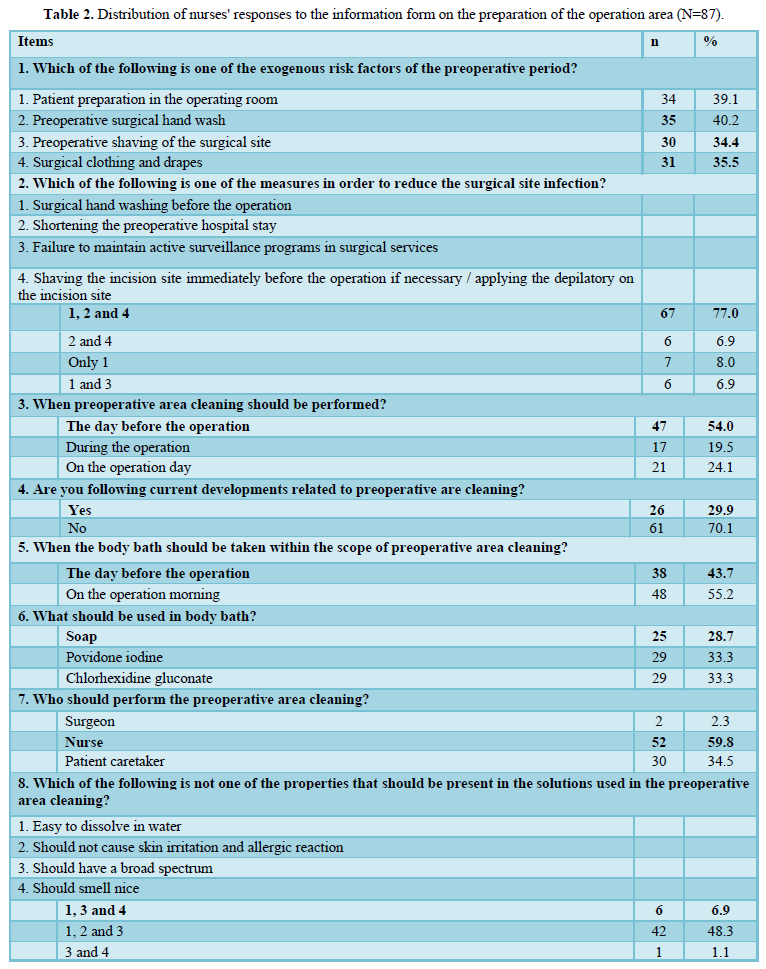
24.6% of them was working in the general surgery clinic and 53.8% of them were responsible for the care and treatment of 5-15 patients per day. Literature information supports our research. The nurses’ working year and the unit they work in allows that they are more competent about the preoperative period preparations. Likewise, the number of cases that the nurses prepare for the operation during the day is also an important factor in the enhancement of this competency. The frequency of use of the information is very important in making the preoperative preparatory training received in the schools permanent. As a matter of fact, according to the results of the research, the nurses are making preparations for operation at an average of 5.36 ± 12.287 days.
It was found that 58.6% of the nurses participating in the study received preoperative training, 9.2% of them received it from a course, 33.3% of them from a seminar, 16.1% of them from the Directorate of Health, and 39.1% of them received for 5 hours or less and experienced an average of 74.81 ± 96.002 surgical site infections per day. Researchers [11] emphasized that the most important factor in the prevention of surgical site infections is the comprehensive training of the health care workers about the preoperative period preparations and the application of the training received in the clinical field. Likewise, another study [7] mentioned the link between education and surgical site infections. These results indicate that although the majority of nurses are experiencing the surgical site infection, it proves that reflecting the training on practice is insufficient. On the other hand, the fact that the nurses encountered the surgical site infection has enabled them to experience the precautions that should be taken.
It was found that 74.7% of the nurses who participated in the study were using the electric shavers in the perioperative area cleaning, allocate 12.57 ± 15.076 minutes on average for the area cleaning, 29.9% of them were following the current approaches about the perioperative area cleaning, preferred to use the povidone iodine the most as the antiseptic solution for the operative area cleaning, and the chlorhexidine, ethyl alcohol, and soap solutions are preferred the most respectively after the said solution. Another study [11] stated that open razors and electric shavers are mostly used in the preoperative area cleaning. According to the national and international preoperative area cleaning guidelines, skin preparation plays an important role in preventing surgical site infections. Skin preparation requires a shower or bath, hair removal, removal of foreign substances, and removal of infectious agents from the incision site and surrounding area. The patient should be cleaned on the day of operation and only the hairs that will prevent the operation should be cleaned. A surgical razor with a disposable blade should be preferred for this procedure and this cleaning should be done outside the operating room.
According to the study, it was determined that 40.2% of nurses stated that the preoperative area cleaning is performed by the nurses, 6.9% of them stated that by patients themselves, 13.8% of them stated that by patient’s relatives, 58.6% of them stated that by the patient caretaker, and 3.4% of them stated that by the barber. The results obtained contradict the theoretical knowledge obtained during nursing education. The fact that such an important issue, preoperative site cleaning, is applied outside the supervision of the nurse can cause an increase in surgical site infection and undesirable cuts in the skin.
When the distribution of the information delivered by the nurses participating in the study to the patient about the preoperative preparations was examined, it was determined that 86.2% of them was delivering information regarding the area cleaning, 56.3% of them regarding the type and purpose of the surgery, 54% of them regarding the risks of the operation, 33.3% of them regarding the medicines to be given during the operation, 40.2% of them regarding the surgical position. In another study conducted [16], 72.3% of the nurses stated that preoperative training was given in the clinic and 61.5% of them stated that these trainings were given by the patient's doctor and nurse. Likewise, it is reported [17] that 68.93% of the patients were informed about the operation in the perioperative period. In our study, the fact that the majority of nurses perform preoperative patient training indicates that the nurses fulfill their roles and functions related to training and meet patients' information needs.
It was determined that 57.5% of the nurses knew the exogenous risk factors of the preoperative period correctly.
It was found that 77% of the nurses participating in the study responded correctly by giving the answers of preoperative surgical hand washing, shaving the incision site just before the operation and using an electric shaver for this purpose, 54% of them the answer of performing area cleaning on the day before the operation, 55.2% of them the answer of performing the body bath in the morning of the operation day. Likewise, it was determined that only 28.7% of the nurses who participated in the study stated that body bath should be done with soap, 33.3% of them with povidone iodine, 33% of them with chlorhexidine gluconate, and 48.3% of them stated that the control of preoperative skin preparation should be performed in the morning of the operation day, 28.7% of them stated that this control should be performed in the operating room, and 25.3% of them was taking consent regarding the preoperative area cleaning.
In another study [11], the result that the preoperative area cleaning should be performed just before the operation was reached. National and international guidelines state that the hair on the surgical area should not be removed unless it is necessary to prevent surgical site infections. Additionally, if hair removal is necessary, since using a razor blade will increase the possibility of infection by causing injury to the skin, it is recommended to remove only the hair that will prevent the operation on the day of the surgery. Similarly, the cleaning should be performed with a surgical razor with a disposable blade and this cleaning should be outside the operating room.
It was determined that 77% of the nurses who participated in the study answered correctly the item of “Surgical site infections are the infection observed in the operation area within 30 or 90 days following the surgical intervention”, 81.6% of them answered correctly the item of “The patient's own skin flora is the most important source for surgical site infection”, 74.7% of them answered correctly the item of “The surgical site infections are not an important cause of mortality and morbidity”. Likewise, 75.9% of them responded correctly by saying that the item of ‘There is no need to clean the surgical area before the operation’ is wrong, 79.3% of them answered the item of ‘Microscopic cuts and abrasions on the skin may occur during the removal hair with open razor’ correctly, 36.8% of them responded correctly by saying that the item of ‘The hair should not be cleaned unless they are obstacle to the surgical area’ is wrong, 74.7% of them responded correctly by saying that the item of ‘The shaving area may be smaller than the incision site’ is wrong, 77% of them answered the item of ‘The hair on the head should only be cut with an electric shaver’ correctly, 66.7% of them answered the items of ‘When shaving over the bone, it should be shaved against the bone and vertically’ and ‘The area to be shaved should be shaved against the direction of hair output’ correctly, 82.8% of them answered the item of ‘The area is painted by beginning from the surgical site with an antiseptic solution in a circular motions from inside to outside’ correctly. In another study [18], similar results with our study were obtained. According to Dönmez, preoperative skin preparation includes shower/bath, hair removal and skin preparation on the operating table. Patients should take a shower or bath with soap or skin antiseptic the night before the operation. The aim of preoperative showering/bathing is to reduce the number of microorganisms on the patient’s skin, the risk of endogenous and exogenous contamination, and the permanent flora. In order to prevent the SSI, it is recommended that patients take a shower or bath with 4% chlorhexidine gluconate the night before or the morning of the operation. After the shower/bath, the patient should be thoroughly rinsed, dried with a clean and dry towel, and should wear clean clothes. The shampoo, hair conditioner or other hair care products should not be used while taking shower before the surgery. According to Donmez, the hairs in the intervention area should be cleaned by taking some precautions if it is an obstacle for the surgical incision, and prevents the suture and dressing. In national and international studies and published guidelines, it is determined that hair cleaning should not be performed unless it is obligatory. If necessary, it should be performed with the electric razors and depilatories. In cleanings performed with the open razors, there may be abrasions, cuts, and irritations on the skin, which allow the growth of microorganisms causing the formation of the SSI. Therefore, open razors should not be used for hair cleaning. Instead of an open razor, the electric shavers with a disposable head that do not impair skin integrity can be used. Hair removal should be performed in sickrooms since it will disrupt the sterilized environment in the operating room. The most appropriate time for hair removal is the morning of surgery. As the time between the hair removal and operation prolongs, the risk of the SSI increases. Scientists [19] stated that the use of an open razor for perioperative area cleaning will cause skin irritation, cuts, and SSI formation and that the safest method is the electric shaver. According to another study [20] in order to prevent the SSI, besides hair removal, the antimicrobial prophylaxis has long-term protective effects.
According to the study, when the scores of the information form on the preparation of the operation area is compared based on the occupational characteristics of the nurses, it was found that there is a significant difference based on the unit they worked (p<0.05). According to the results of the analysis, the surgical area preparation scores (14.18 ± 3.321) of the nurses working in the mixed services were statistically significantly higher than the surgical area preparation scores (11.46 ± 2.332) of the nurses working in only the internal service (p<0.05). This is an expected result since the nurses working in mixed service are more likely to encounter surgical cases than those working in the internal service. Surgical site infections are one of the most important problems of surgery in terms of increased mortality, morbidity, length of hospital stay and hospital costs. The patient's own skin flora is the most important source for the SSI and the microorganisms can easily spread from poorly prepared skin to the wound. Therefore, knowing all the risk factors that cause surgical site infection, performing the area cleaning with an electric shaver, which is an effective method, on the morning of the operation and taking the necessary precautions will reduce the SSI incidence. For this purpose, it is recommended that the clinic support nursing practices is supported, that the protocols are established, that the nurses follow the current approaches about skin preparation, and that the nurses are supported and rewarded in order for them to take responsibility related to the subject [21].
ACKNOWLEDGEMENT
The authors would like to thank all participants for their involvement.
CONFLICT OF INTERESTS
No conflict of interests has been declared by the authors. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
ETHICAL ASPECTS OF RESEARCH
Approval (30.01.2018/02-05) was obtained from Istanbul Bilim University Institute of Health Sciences Ethics Committee before starting the study.
1. Kara E (2009) Surgical Field Infections and Antibiotic Prophylaxis in Surgery. J Accum Health 1: 28-32.
2. Aydın M, Erduran M (2012) Surgical field ınfections associated with health care. Dergipark 1: 28-33.
3. Çakırcalı E (2000) Basic principles and applications in patient care and treatment. İzmir.
4. Baskan S (2000) Risk factors in surgical field ınfections. J Hosp Infect 4: 233-239.
5. Kaymakçı Ş (2015) Ensuring asepsis in the operating room. Operating Room Nursing. Meta Printing Printing Services, İzmir, pp: 423-444.
6. Uslu Y, Yavuz M (2015) Preoperative hair removal: Systematic review. JEUFN 2: 67-77.
7. Kalkan N, Karadağ M (2017) Current approaches in the prevention of surgical field ınfections and prevention ınterventions for nurse’s algorithm. J Health Sci 4: 280-289.
8. Wooding TJ, Mancaster K (2015) Preoperative hair removal to reduce surgical ınfection. Best Pract 2015: 1-4.
9. Pala N (2010) Precautions taken by the operating room nurses in the prevention of surgical field ınfections from the operating room. Istanbul University Institute of Health Sciences.
10.Tanner J, Gould D, Jenkins P, Hilliam R, Mistry N, Walsh S (2012) A fresh look at perioperative body washing. J Infect Prevent.
11. Sepit D (2007) Preoperative hair removal application to reduce surgical zone ınfections. J Nurs Res 4: 16-20.
12. Çakmakçı M (1999) Operating room and surgical ınfections. J Hosp Infect 2: 140-146.
13. Terzi C (2006) Surgical field ınfections. J Ankem 3: 187-193.
14. Tayran N (2008) Prevention from surgical field ınfections. J Hosp Infect 60: 181-182.
15. Aygin D, Marul F (2016) Innovations in surgical field ınfection definitions and current practices in preoperative hair removal. Turk J Health Sci 3: 28-36.
16. Gürlek Ö, Yılmaz M (2013) Preoperative patient education application status of nurses working in surgical clinics. Anatol J Nurs Health Sci 16: 8-15.
17. Özbayır T, Demir F, Candan Y, Çoşkun İ, Dramalı A (2003) Investigation of the Impressions of Patients in the Perioperative Period. J Atatürk Univ School Nurs 6: 14-23.
18. Dönmez YC (2016) Preoperative skin preparation. Turkiye Klinikleri. J Surg Nurs 2: 11-6.
19. Tanner J, Narrie P, Melen K (2011) Preoperative hair removal to reduce surgical site ınfeciton. CDSR 11: 22-41.
20. Alp E (2005) Infection control in surgical clinics. ANKEM 19: 165-169.
21.Özbayır T (2010) Internal and Surgical Care. Nobel Bookstore, Adana, pp: 309-344.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4




QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- BioMed Research Journal (ISSN:2578-8892)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- International Journal of Diabetes (ISSN: 2644-3031)
- Advance Research on Alzheimers and Parkinsons Disease
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Rheumatology Research (ISSN:2641-6999)


