INTRODUCTION
The Emergency Department (ED) sometimes termed the emergency room (ER), or the accident and emergency (A&E) Department-in a hospital or primary care facility that provide initial treatment to patients with broad spectrum of illnesses and injuries, some of which may be life threatening or requiring immediate attention [1].
Triage is the process of determining the priority of patient’s treatment based on severity of their condition. The term comes from the French verb “Trier” means to separate or Select [2,3]. A strong triage system is the backbone of efficient emergency department. It indicates that the staff is capable of differentiating critically ill from the sick, and consequently, of segregating patients who may need admission from those who will not. Thus, it’s essential for the health professionals to be well versed with the concepts of triaging. Patients shall be evaluated quickly for their vital signs, chief complaints and other key indicators to be categorised as [4]:
Category-I (Red, obvious life-threatening emergency)
Physician shall examine patient with zero delay. Cases include cardiac arrest, continuous seizures, acute severe chest pain, hematemesis, sudden loss of consciousness and major trauma with hypotension.
Category-II (Yellow, potential for life threatening emergency)
There is the possibility of occult or pending emergency condition. Patients shall be treated by physician within 10 min of arrival. Cases include dyspnoea, high grade fever, acute abdominal pain, acute confusion, severe pain, serious extremity injuries and large lacerations.
Category-III (Green, Non-life-threatening emergency)
These patients shall be seen by emergency management physician on first come first serve basis. Examples include chronic, minor, self-limiting disorders, skin disorders, mild adult upper respiratory tract symptoms and mild sore throat.
According to study conducted by Rahmati et al. [5] on recent trends in triaging, from May 2013-2014, study suggested only 54% of nursing staff received triage training while remaining 46% have little or no training in triage system. 58% of nurses use patients’ clinical signs and symptoms for triaging while 26% didn't see any need to triage patients. An astounding 60% nursing staff are unaware of scale of measurement used for triaging in their hospital. Indications of triaging are reducing the waiting time for patients and their attendants, ensuring patients’ satisfaction from hospital staff and utmost saving lives. Advantages are better health services, low mortality, increased levels of satisfaction and less wastage of time and resources.
METHODS
This was an observational study done at a tertiary care hospital in north India. Study period was 2 months and 50 patients were recruited. In this study we have assessed the satisfaction levels of patients and their attendants, capacity of emergency staff to triage patients according to acuity and we have compared the waiting time and mortality before and after the introduction of triage system in the ED. A printed patient satisfaction form was used which includes doctor kindness, nurse patience, nurse knowledge, waiting time, hygiene.
Patients were randomly included in the study and data was recorded by trained nursing staff in his/her duty period after taking consent. The ED doctors and nursing staff have been clear cut instructions how to triage patients into red, yellow and green zones according to their symptoms, vital signs and examination.
OPERATIONAL DEFINITIONS
Satisfaction level
Refers to measure of extent to which a patient is content with health care services they received after they stepped up emergency.
Triage
Refers to the assessment of a patient on arrival to the emergency department to determine the priority for medical care based on clinical urgency of the patients’ presenting condition.
Acuity
Refers to the state of urgency with which the patients reach ED.
STATISTICAL ANALYSIS
Data was entered in windows excel sheet and the analysis was done using statistical Software SPSS Statistical Software Version 23. (SPSS Inc, Chicago, IL, USA). Quantitative variables (age of patient, waiting time) were presented as average ± standard deviation (numerical variables with Gaussian distribution), median and interquartile range (numerical variables with nonparametric distributions) respectively. Proportions were represented as percentage from the sub-group total (number of individuals). To evaluate the strength of the association between two continuous variables we used Spearman’s correlation coefficient; the statistical significance of the correlation was evaluated using t-distribution test. A p-value of 0.05 was considered the threshold of statistical significance.
RESULTS
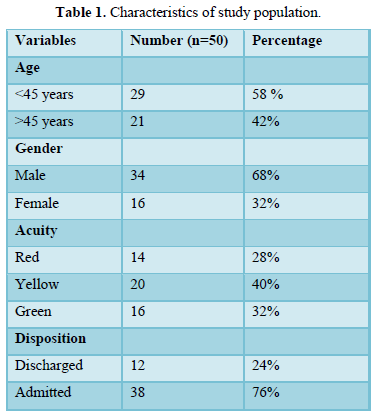
A total of 50 randomly selected patients were included and the baseline characteristics of study population are given in Table 1.
Of these 50 patients in the study population, 44 of them are satisfied in the care provided to them and have reduced waiting time of 8 min as compared to 15 min before introduction of triage system. In our hospital in triage system in emergency department both doctors and nurses used to effectively triage the patients according to the severity into three categories (red, yellow, green) and decide them to the final disposition whether to discharge or admit the patient.
In our hospital 90 percent of the staff received triage training before posting into the emergency, so this would result in high satisfactory level among the patients and their relatives when they receive the treatment.
The mortality rate is 25% as compared to 36% before the introduction of triage in the hospital. When comparing the mortality among the patients admitted to emergency department after effective triage the change was significant (25% versus 36% and p-value < 0.05 (significant)), because of effective patient care, patient doctor ratio, patient nurse ratio, severity of underlying illness, comorbidities and patient bed ratio are also taken into consideration in triaged patients.
DISCUSSION
In our study we recruited 50 patients presented to the emergency department of a tertiary care hospital in north India, and triaged them into three categories (red, yellow and green) based on the severity of illness, haemodynamic parameters and pre-existing comorbidities.
We divided them into two age groups above and below the 45 years of age for easy evaluation of the study. In our study there are 29 patients below age of 45 years and 21 patients were above age of 45 years. Patients attending to emergency department when triaged majority of them fall into yellow category followed by green and red, this implies immediate resuscitate measures should be undertaken in the triage system to save the lives of patients and this is also implication for need of effective staff in the triage with good training, these findings were correlated with a study conducted [6].
Waiting time to see the patient was also decreased with the introduction of triage system from 15 min to 8 min these findings were in par with the study conducted [7].
After effective triaging most of the patients 38 out of 50 required admission to the hospital which also tells that the most important thing for emergency patients is to categorise and to treat them accordingly. This will also reduce the waiting time for the serious patients and to give the initial treatment.
The above findings correlate with a study conducted [8] in which they expand hospital capacity, stopping to regulate hospitals to the extreme, providing care only to patients with emergencies, providing alternatives for primary care of the uninsured, stopping to board admitted patients in the emergency department, using evidence- based guidelines to address imaging over utilisation, changing admitting patterns, expanding the role of ancillary ED staff and hallway care.
When coming to the satisfactory levels among the patients and their relatives most of them were satisfied (44 patients versus 6 patients) with the treatment given and with the staff in the triage department. Among these 6 patients they were not satisfied due to prolong waiting period for interaction with the staff in the triage department these findings were similar to study conducted [9] among which impatience is the most important factor among patients and relatives.
In our emergency department most of the staff over 90 percent were well trained in triaging the patients based on clinical findings and haemodynamic parameters.
At last when comparing mortality to the admitted patients the mortality change was significant (p value <0.05) before and after triage because the in-hospital mortality depends on the other factors like availability of beds, patient care, doctor patient ratio as well as nurse patient ratio, when these patients were triaged. These findings were similar to study conducted [10]. So, by keeping all above factors in mind its concluded that effective triaging system and highly trained staff in triage helps to achieve high satisfactory levels among the patients and their relatives, decrease the waiting time to see high risk patients, decrease mortality and helps to provide specialized treatment to high risk patients.
LIMITATIONS
1. Small sample size
2. Single centre study
3. Other Comorbidities which play a role in mortality of these patients are not taken into account.
CONCLUSIONS
1) Effective triaging results in high satisfaction among the patients and their relatives in view of treatment and care they received.
2) Triage system in emergency leads to decrease in waiting time for high risk patients.
3) Staff in the triage should be highly trained in-patient care and in categorising patients into different groups (red, yellow and green) based on severity of illness and haemodynamic parameters.
4) Mortality was significantly reduced after introduction of triage system because of improved quality care to more serious patients.
1. Oredsson S, Jonsson H, Rognes J, Lars L, Nasim F, et al. (2011) A systematic review of triage-related interventions to improve patient flow in emergency departments. Scand J Trauma Resusc Emerg Med 19: 43.
2. Koenig KL, Schultz CH (2010) Koenig and Schultz’s disaster medicine: Comprehensive principles and practices. Cambridge University Press.
3. Jenkins JL, McCarthy ML, Sauer LM, Gary BG, Edbert BH, et al. (2008) Mass-casualty triage: Time for an evidence-based approach. Prehosp Disaster Med 23: 3-8.
4. Bhalla MC, Frey J, Rider C, Nord M, Hegerhorst M (2015) Simple triage algorithm and rapid treatment and sort, assess, lifesaving, interventions, treatment and transportation mass casualty triage methods for sensitivity, specificity and predictive values. Am J Emerg Med 33: 1687-1691.
5. Rahmati H, Azmoon M, Meibodi MK, Zare N (2013) Effects of triage education on knowledge, practice and qualitative index of emergency room staff: A quasi-interventional study. Bull Emerg Trauma 1: 69-75.
6. Derlet RW, Richards JR (2008) Ten solutions for emergency department crowding. West J Emerg Med 9: 24-27.
7. Kumar A, Lakshminarayanan D, Joshi N, Vaid S, Bhoi S, et al. (2019) Triaging the triage: Reducing waiting time to triage in the emergency department at a tertiary care hospital in New Delhi, India. Emerg Med J 36: 558-563
8. Hong WS, Haimovich AD, Taylor RA (2018) Predicting hospital admission at emergency department triage using machine learning. PLoS One 13: e0201016.
9. Rowe BH, Channan P, Bullard M, Bltiz S, Saunders D, et al. (2006) Characteristics of patients who leave emergency departments without being seen. Acad Emerg Med 13: 848-852.
10. Richardson DB (2006) Increase in patient mortality at 10 days associated with emergency department overcrowding. Med J Aust 184: 213-216.

 Table 1
Table 1


