Short Communication
An Unusual Case of Megakaryocytic Blast Crisis of Chronic Myeloid Leukemia
2975
Views & Citations1975
Likes & Shares
INTRODUCTION
Chronic myeloid leukemia (CML) is an acquired myeloproliferative neoplasm characterize by a cytogenetic abnormality, the t (9;22); leading to the chromosome Phi or its molecular expression the BCR-ABL gene.
The natural history of untreated CML is biphasic or triphasic: an initial indolent chronic phase (CP) is followed by an accelerated phase (AP), a blast phase (BP), or both. Although tyrosine kinase inhibitors are highly effective in the treatment of CML, some patients evolve into a blast crisis.
Megakaryocytic blast crisis is rare manifestation of CML, we report here an unusual case of megakaryocytic blast crisis. The morphology with a careful study of the blood smear as well as the flow cytometry were decisive to make the diagnosis. This last was perform using an 8 color-BD FacsLyric cytometer and positivity of CD41 and CD61 confirmed the megakaryocyte lineage.
CASE PRESENTATION
A 59-year-old woman BCR-ABL positive, diagnosed 2 years ago and under Dasatinib, was referred to our hospital for back pain, disorientation and fever. Physical examination revealed splenomegaly type 2 and pallor.
The blood count showed severe normocytic anemia: Hb=58g/L and MCV = 90FL; high leukocytosis (405 × 109/L) and low platelet count (89 × 109/L).
Blood examination showed hyper cellularity with marked increase in granulocytes and their precursors. The megakaryocytic lineage was present in the blood film with very atypical morphology.
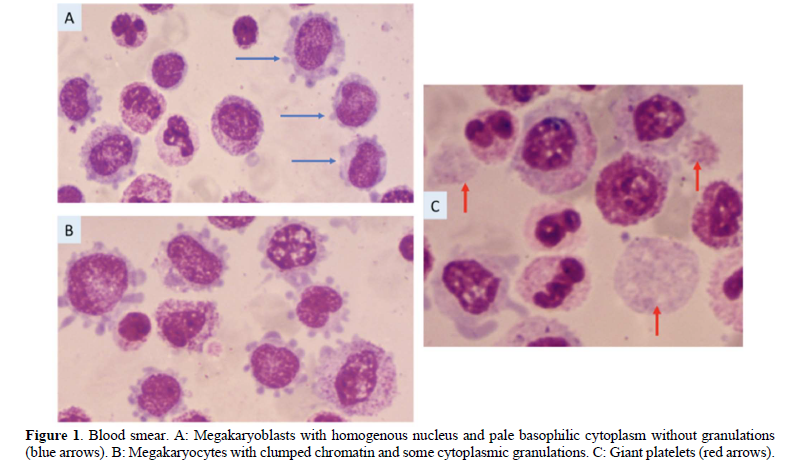
In Figure 1A, the 3 cells (blue arrows) are megakaryoblasts (17%) with a high N:C ratio, their nucleus is homogeneous and the nucleoli are not visible. The cytoplasm, basophilic, is agranular with cytoplasmic protrusions (blebs) that appear ragged but well defined.
In Figure 1B, similar cells are visible but they seem to be megakaryocytes (22%) with clumped chromatin and granulations are seen in their cytoplasm which is less basophilic. Many circulating giant platelets are also seen in the blood smear (Figure 1C).
The flow cytometry, on peripheral blood, confirmed the megakaryocytic lineage with the positivity of CD61 (51%) and CD41 (58%). The expression of myeloid markers such as CD117, CD33 and CD11b were weak.
Bone marrow aspiration revealed a hyper cellularity with the same cytological findings as in peripheral blood and no fibrosis was observed on bone marrow biopsy. Cytogenetic as well as molecular biology were not performed at this time. Palliative care (transfusions, antibiotics) was introduced as a first step but the patient passed away few days later.
In CML blast crisis with a significant megakaryoblastic component is rare and bone marrow fibrosis is often marked and leading to peripheral cytopenia [1,2].
This case of megakaryocytic blast crisis with a high cellularity is quite uncommon: lack of fibrosis, hyper cellularity and atypical morphology of megakaryocytes. This atypical appearance of megakaryocytes makes necessary confirmation of their nature by immunophenotyping to demonstrate platelet membrane antigens.
FUNDING
None
CONFLICT OF INTEREST
None
REFERENCES
-
Khemka R, Gupta M, Jena NK (2019) CML with Megakaryocytic Blast Crisis: Report of 3 Cases. Pathol Oncol Res 25(3): 1253-1258.
-
Kagotho E, Chang H (2020) CML in megakaryocytic transformation and extramedullary infiltration. Blood 135(7): 514.
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Chemotherapy Research Journal (ISSN:2642-0236)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- International Journal of Diabetes (ISSN: 2644-3031)
- Journal of Pathology and Toxicology Research
- Journal of Cancer Science and Treatment (ISSN:2641-7472)


