2698
Views & Citations1698
Likes & Shares
Background: Manipulation
under anesthesia (MUA) is an orthopedic procedure which can benefit patients
with musculoskeletal pathologies. This review article analyzes the efficacy of
manipulation under anesthesia based on existing literature. Pain, range of
motion, strength, ability to carry out activities of daily living and
likelihood of refilling an opioid prescription has been examined.
Methods: The
literature review was carried out using PubMed database and Colwiz software was
utilized as a reference manager. Initial literature review showed a total of
6,240 articles. After screening for duplicates and excluding abstracts not
relevant to our inquiry, a total of 19 studies were selected for full article
review. Finally, a total of 8 articles met our inclusion criteria and were
included in this review.
Results: Five
articles in this review studied the effects of MUA on adhesive capsulitis in
otherwise healthy patients using Constant-Murley and adjusted Constant-Murley
scores. Two articles specifically studied the effects of MUA on adhesive
capsulitis in diabetic patients using Oxford and adjusted Constant-Murley
scores. Lastly, one paper examined the effects of MUA on the likelihood of
refilling an opioid prescription.
Conclusion:
This paper proves that MUA is an efficacious
technique for treatment of adhesive capsulitis and reducing the likelihood of
refilling an opioid prescription. Although we recommend additional studies to
further prove its efficacy, we believe that this procedure holds invaluable
benefits for patients.
Keywords: Manipulation, Anesthesia, Adhesive capsulitis, Orthopedic procedure
INTRODUCTION
Manipulation
under Anesthesia (MUA) is an orthopedic procedure that has been in practice
since the 1930s. However, not much is known about the actual efficacy of this
treatment. The procedure fell out of popular use in the 1950s due to
complications from the anesthesia typically used at the time, but was revived
in the 1990s when safer agents were beginning to be utilized [1]. Today, MUA is
used as an alternative for patients suffering from musculoskeletal ailments
that have failed surgery or conservative measures such as physical therapy and
pharmacotherapy. Additional patient qualifications for MUA include those who
have experienced orthopedic trauma or surgery and have experienced excessive
scar tissue build up either as a direct result of invasion or from decreased
use of the joint itself. MUA involves sedating the patient with general
anesthesia, followed by articular and soft tissue mobilization. The movement is
carried out in a specified arc of motion until an audible sound of the
adhesions breaking is heard. This procedure is chosen not to be carried out in
conscious patients due to the possibility of eliciting pain or muscle spasms.
The primary aims of MUA are to restore patient mobility and strength, to
relieve pain in symptomatic patients and to break up scar tissue, thus
decreasing inflammation and increasing range of motion. The procedure can be
carried out by a trained and licensed chiropractor, physician, or surgeon in
either an inpatient or outpatient setting in the United States. Additionally, new
research has shown that orthopedic manipulation may lead to a reduced incidence
of refilling a prescription for an opioid analgesic [2]. A well-known crisis in
medicine today is the opioid epidemic that has become widespread throughout the
United
Although MUA is often used in practice in the United
States, little research has been done to broadly examine the efficacy of this
treatment. This review was carried out to provide an in-depth analysis of
patient reported outcomes both pre- and post-MUA based on the available
literature. By analyzing multiple studies, our aim was to reveal the benefits of MUA by looking at patient
outcomes such as active range of motion, pain scores, muscle strength and
improvement in activities in daily living after receiving this treatment.
METHODS
A literature review was carried out by utilizing the PubMed database using the
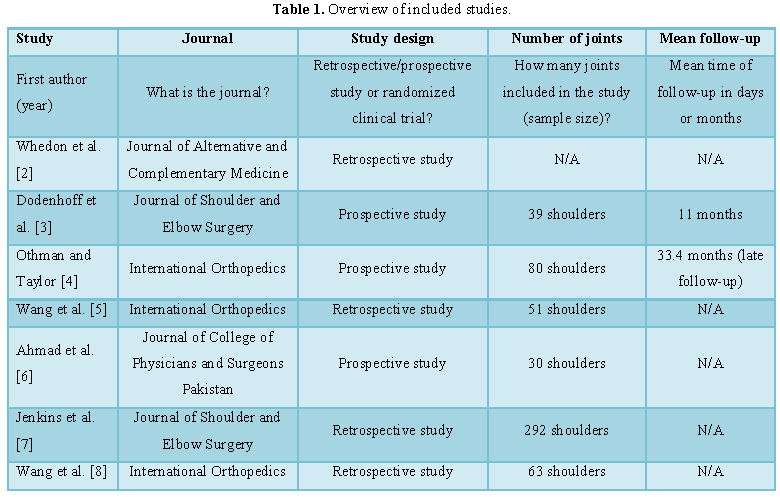
search terms found in Table 1. All
articles were searched and obtained through the Michigan State University
library website. The Preferred Reporting Items and
Systematic Reviews (PRISMA) 2009 checklist was used as a reference to carry out
this review. The article on prescription opioids was selected individually and
specifically separate from the primary literature review.
A total of 19 articles were selected after initial title
and abstract review. All articles collected were organized using a reference
manager. After applying the inclusion and exclusion criteria, a total of 8
articles were chosen to be used for this manuscript. Inclusion criteria
included studies that were measuring changes in range of motion, pain scores,
muscle strength, and activities of living as a result of MUA.
Articles that were not included in this paper either were observing factors
that were not in the scope of this study or only mentioned the use of MUA without
mentioning its efficacy as a treatment.
BENEFITS OF MUA ON ADHESIVE
CAPSULITIS
Multiple studies in the literature have provided data
showing that MUA can have a significant impact on active range of motion in
patients after receiving MUA. Often following trauma or surgery, reduced usage
of a certain joint can lead to the buildup of scar tissue over time, limiting
the range through which a patient can move freely and without pain.
Consequently, decreased usage of the muscles leads to atrophy and weakness over
time.
Several articles specifically studied the effects of MUA on
patients with adhesive capsulitis, also known as frozen shoulder. Frozen
shoulder has been categorized as a self-limiting illness; however the condition
can cause pain in patients and limit their range of motion. MUA is being
studied specifically as a measure of treatment that may limit the duration of
the disease and may even improve outcomes at the end of treatment. Dodenhoff et
al. [3] preferred to classify frozen shoulder into two categories: primary and
secondary. Primary frozen shoulder describes patients, who have not experienced
any event other than a general loss of movement, and secondary frozen shoulder
applies to patients who are experiencing post-traumatic stiffness or have
symptoms related to diabetes mellitus, post-myocardial infarction pain and
inflammatory disorders [3]. Shoulder recovery and improvement following MUA can
be measured with the Constant-Murley shoulder score. This score system is a
100-point scale containing parameters that define the level of pain and the
ability to carry out normal daily activities for a patient [1]. The test is
divided into four subscales: pain (15 points), activities of daily living (20 points),
strength (25 points) and range of motion in forward elevation (flexion),
external rotation, abduction, and internal rotation of the shoulder (40
points). Higher patient score is correlated with a greater quality of function
at the shoulder joint. Several studies cited in this review utilize the
Constant-Murley score to assess progress in a patient post-MUA. Dodenhoff et al.
[3] prospectively assessed 39 shoulders in 37 patients diagnosed with primary
frozen shoulder. The Constant-Murley shoulder score was implemented and found
in their results an average of 24 points pre-MUA, 63 points at 3-6 weeks
follow-up, 69 points at 3 months follow-up and 73 points at follow-ups greater
than 6 months (all values were statistically significant, p<0.01) [3]. Additionally,
89% of patients were reported to be satisfied with the results of MUA after 6
months follow-up [3]. The authors view MUA as a simple, well-tolerated
procedure with a high patient satisfaction and a low complication rate and
recommended its use in reducing the duration of morbidity from frozen shoulders
[3]. Othman and Taylor [4] conducted a study looking at 74 frozen shoulders
both pre- and post-MUA using an adjusted Constant-Murley score by excluding the
abduction strength measurement, thus creating a maximum score of 75. The
researchers chose to do this as measurement of abduction strength is difficult,
especially since most patients with frozen shoulder cannot abduct their arm to
90 [4]. Measuring abduction strength may result in falsely lower Constant-Murley
scores [4]. The average score for observed patients was 24.7 points pre-MUA,
54.9 points at 3 weeks follow-up, and 72.4 points at 33 months follow up [4].
The authors believe that manipulation does speed up recovery from frozen
shoulder and that this recovery is maintained [4]. Wang et al. [5] evaluated 47
cases with 51 frozen shoulders using an adjusted Constant score excluding
muscle strength for a maximum score of 75. The averages for the Constant scores
were as follows: 22.8 ± 4.9 (10-31) pre-MUA, 52.6 ± 9.2 (31-67) at 3 weeks
follow-up and 70.1 ± 6.2 (54-75) at 82 months follow-up with 23 shoulders
scoring a maximum of 75 points [5]. The authors agree that MUA is a simple and
non-invasive procedure that can be used for reducing the course of frozen
shoulders and improving shoulder function and symptoms efficiently [5].
Using the Constant-Murley score is not necessary to
evaluate the effectiveness of MUA on frozen shoulders. More traditional methods
of measuring range of motion, pain and strength can be used. Ahmad et al. [6]
observed the immediate outcome of MUA in 30 cases with adhesive capsulitis in
terms of gain of range of movement (ROM). Range of motion in patients was
measured with a goniometer. External rotation increased from 1.133° ± 0.345°
before MUA to 2.06° ± 0.868° after MUA (p<0.001) [6]. Medial rotation
increased from 1.366° ± 0.490° before MUA to 2.766° ± 0.897° after MUA
(p<0.001). Flexion increased from 1.833° ± 0.746° before MUA to 3.400° ±
0.674° after MUA (p<0.001). Abduction increased from 2.266° ± 0.639° before
MUA to 3.433° ± 0.817° after MUA (p<0.001) [6]. External rotation was the
least improved, however it is noteworthy to see that in every case patients had
a significant improvement in range of motion. A significant decrease in pain
intensity, 3.667 ± 0.808 before MUA and 2.10 ± 1.02 after MUA, was appreciated
using a numerical pain scale (p<0.001) [6].
MUA IN DIABETIC PATIENTS WITH
ADHESIVE CAPSULITIS
Diabetes mellitus is a systemic condition characterized by
a sharp increase in blood glucose, leading to damage to many different areas of
the body including the musculoskeletal system. The incidence of frozen shoulder
in the diabetic population is 10-36% compared to 2-5% in the general population
[7]. Additionally, frozen shoulder has a more severe course in diabetic
patients. Therefore, we must identify treatment options for these patients as
they tend to respond less well to conservative treatment. Jenkins et al. [7]
conducted a retrospective study analyzing data collected during a 10 year
period of referrals for frozen shoulder of both diabetic and non-diabetic
patients. They hypothesized that diabetic patients with frozen shoulder who
received MUA would have the same outcomes as the non-diabetic group [7].
Thirty-nine diabetic shoulders and 274 non-diabetic shoulders were assessed
pre-MUA with an Oxford Shoulder Score (OSS). Of the 39 diabetic shoulders, 23
were available for long-term follow up, with 229 of the 274 non-diabetic
shoulders available for long-term follow up [7]. Their study found no
significant difference in the OSS between the two groups after the initial MUA
[7]. OSS was 27 before first MUA and 41 after first MUA in the diabetic group,
and 27 before first MUA and 43 after first MUA in the control group [7].
Conclusively, they believe that MUA offers significant subjective and objective
benefit for diabetic patients with frozen shoulder [7]. These results are
important for diabetic patients as they tend to have a higher risk of
perioperative complications with more invasive techniques that may be used to
treat frozen shoulder [7]. Wang et al. [8] conducted a study observing the
outcomes of both diabetic and non-diabetic patients treated with MUA for frozen
shoulder. Using an adjusted Constant score of 75 rather than the score system
of 25 points usually used for assessment of muscle strength, the authors
retrospectively analyzed 42 non-diabetic shoulders and 21 diabetic shoulders
[8]. Their findings showed no statistical difference for pain, activity, ROM and
adjusted Constant scores between the two groups [8]. Therefore, Wang et al
concludes that MUA speeds up the recovery of frozen shoulders and improves
shoulder function and symptoms within a relatively short period of time [8].
They believe that although diabetes is a precipitating factor for frozen
shoulder, it is not correlated with a worse prognosis [8].
MANIPULATION AND OPIOID USE
Another very interesting topic that is beginning to come to
light is the relationship of manipulative services and the use of prescription
opioids in patients. The heavy use of prescription opioids began in the 1990s
and today, there are more than 650,000 opioid prescriptions being dispensed per
day [2]. Little evidence exists proving that opioids improve chronic pain,
quality of life or functioning in daily activities [2]. The opioid epidemic
cost nearly $56 billion in health care and social costs in 2007 alone [2].
Therefore, other alternative options must be explored in order to address this
ever-growing problem. Whedon et al. [2] conducted a study with the objective of
attempting to make a connection between patients who receive chiropractic
services and if that results in a lesser likelihood of refilling an opioid
prescription. They retrospectively analyzed 13,384 subjects with 6,868 being
recipients and 6,516 being non-recipients. Recipients included subjects with at
least two office visits for a primary diagnosis of low-back pain, for which the
provider was a doctor of chiropractic medicine [2]. Non-recipients included subjects
who received no services from chiropractors [2]. The authors found that among
the recipients, 19% refilled a prescription opioid compared with 35% of the
non-recipients (p<0.0001) [2]. Also, the adjusted likelihood of filling a
prescription for an opioid analgesic in 2014 was 55% lower in the recipient
group compared to the non-recipient group (p<0.0001) [2]. These findings
have the potential to have a tremendous impact on how musculoskeletal pain is
approached in medicine today. However, the authors admit that this study alone
is not enough proof to definitely link the manipulative technique of
chiropractic services with the likelihood of refilling an opioid prescription
[2]. Further studies must be carried out to further confirm the benefits that manipulation
techniques may have in reducing opioid use among patients.
LIMITATIONS OF MUA STUDIES
One of the major limitations in assessing the efficacy of
MUA is the unavailability of an objective way to evaluate pain improvement in
patients. Additionally, not all studies use the same methods to assess pain and
therefore it is difficult to compare multiple studies in this manner. In the
study on opioids, there were many factors that were unavailable to the
researchers, such as fill dates for the prescription or diagnoses available in
the pharmacy data [2]. Also, the conclusions drawn from this study alone are
not sufficient to definitely link the use of chiropractic services to the
likelihood of filling an opioid prescription [2]. Another limitation of MUA
studies is that research has not been conducted to compare a group of patients
who receive MUA for frozen shoulder and a group who do not receive MUA.
Therefore, we cannot say for sure whether MUA truly speeds up recovery from a
frozen shoulder, or if the illness would resolve on its own in the same amount
of time. Studies must be carried out comparing MUA and non-MUA groups in
examining their progress in range of motion over time to further legitimize the
efficacy of MUA. Future studies on MUA could be improved in a number of ways.
The studies mentioned in this review have a variable range of follow-up
periods, some lasting as few as six weeks. We recommend a follow-up period of
at least 6 months to assess the efficacy of MUA. Additionally, many of the
studies did not mention how MUA affected their activities of daily living. This
is an extremely important variable that needs to be further explored in order
to improve patient care, as range of motion alone does not explain how MUA has
affected their lives in a positive or negative way.
DISCUSSION
MUA is a procedure that requires further studies to determine
whether it should be used in future clinical practice, but has proven to be
useful in many different areas of orthopedic medicine. In this manuscript we
attempted to gather all of the highest quality evidence available in order to
investigate its efficacy. However, we realize that larger sample sizes are
required in order to accurately measure whether it is superior to other methods
of standard treatment. Hence, if MUA proves to be as successful for treating
the listed ailments as other measures of treatment today, we may see a major
change in the way orthopedics are practiced in the future. Due to MUA being a
non-invasive procedure, patients may see a lesser financial burden in the
future due to decreased hospital stay among other financial factors. Wang et al.
[5] found that there was less improvement in Constant-Murley scores in patients
with postoperative frozen shoulders. They believe this may be influenced by the
initial injury or initial operation. Studies should be conducted comparing the
efficacy of MUA on shoulders that have undergone surgical intervention and
those that have not. Manipulation under anesthesia can provide numerous
benefits for qualified patients. The literature thus far has shown its efficacy
in practice and should be considered by physicians for patients who suffer from
chronic musculoskeletal stiffness and pain. We believe that further studies
must be carried out to examine its effectiveness compared to other techniques
and practices in the medical field.
1. Wikipedia
(2009) Manipulation under anesthesia. Available online at: https://en.wikipedia.org/wiki/Manipulation_under_anesthesia
2. Whedon
JM, Toler AWJ, Goehl JM, Kazal LA (2018) Association between utilization of
chiropractic services for treatment of low-back pain and use of prescription
opioids. J Altern Complement Med 24: 552-556.
3. Dodenhoff
RM, Levy O, Wilson A, Copeland SA (2000) Manipulation under anesthesia for
primary frozen shoulder: Effect on early recovery and return to activity. J
Shoulder Elbow Surg 9: 23-26.
4. Othman
A, Taylor G (2002) Manipulation under anaesthesia for frozen shoulder. Int
Orthop 26: 268-270.
5. Wang
JP, Huang TF, Hung SC, Ma HL, Wu JG (2007) Comparison of idiopathic, post-trauma
and post-surgery frozen shoulder after manipulation under anesthesia. Int
Orthop 31: 333-337.
6. Ahmad
D, Hashim JA, Asim HM (2014) Outcome of manipulation under anesthesia in
adhesive capsulitis patients. J Coll Physicians Surg Pak 24: 293-294.
7. Jenkins
EF, Thomas WJ, Corcoran JP, Kirubanandan R, Beynon CR, et al. (2012) The
outcome of manipulation under general anesthesia for the management of frozen
shoulder in patients with diabetes mellitus. J Shoulder Elbow Surg 21:
1492-1498.
8. Wang
JP, Huang TF, Ma HL, Hung SC, Chen TH, et al. (2010) Manipulation under
anaesthesia for frozen shoulder in patients with and without non-insulin
dependent diabetes mellitus. Int Orthop 34: 1227-1232.
-
 Table 1
Table 1
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Journal of Allergy Research (ISSN:2642-326X)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- BioMed Research Journal (ISSN:2578-8892)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)


