2669
Views & Citations1669
Likes & Shares
Objective: The aim of this study was to determine the
prevalence and associated factors of low back pain among schoolchildren in
Ouagadougou.
Patients and methodology: It was a cross-sectional study
from the 1st to the 30th of June 2018 involving schoolchildren of 6
to 16 years old from two schools (public and private). We included all
consenting schoolchildren. We required a parental consent form duly filled and
signed. Two rheumatologists examined all the included schoolchildren. We
studied the socio-demographic characteristics, lifestyle, clinical
characteristics, weight of the schoolbag and the family history of each school
child.
Results: Three
hundred and ninety-six schoolchildren were included. One hundred and fifty-three (38.6%) had excess
schoolbag weight at 10% of body weight, thus failing to meet international
recommendations. The prevalence of low back pain was 9.01% (36 children: 17
boys and 19 girls). Their average age was 9.3 ± 1.87 years with extreme ages of
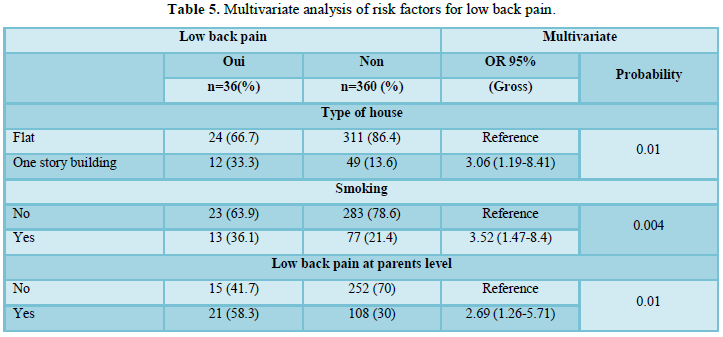
6 and 14 years. In a multivariate analysis, only the type of house (story
building), smoking by a parent and low back pain of a parent were the risk
factors for low back pain in schoolchildren with odd ratios at 3.06, 3.52 and
2.69, respectively.
Conclusion:
Educating parents about the passive smoking they
are exposing their child could reduce the prevalence of low back pain in school
settings. These data should also be considered in educational campaigns for
reducing school equipment weight.
Keywords: Prevalence, Low back pain, School children, Africa
INTRODUCTION
Low back pain is a
real public health problem because of its frequency and impact. Its prevalence
has been estimated at 18.3% in adults [1]. It has been shown that in workplace,
low back pain affects nearly 50% of hospital staff of a public health facility
in Burkina Faso [2]. Epidemiological studies have shown that it is not only an
adult pathology but also frequently reported in children and adolescents [3,4].
However, reported prevalence varies widely from one study to another, ranging
from 8% to 74% in schools [5]. In Africa, few studies have been published on
this subject. The few studies reported a prevalence of low back pain ranging
from 12.3% to 37.8% in school settings [6-9].
The risk
factors associated with low back pain in schools also vary according to the
series [4]. Individual factors (age, sex, weight and height of the schoolchild),
exposure factors (heavy load handling, prolonged postures, sitting or not,
weight of bag, distance from home to school) and social factors (low back pain
in parents, passive smoking) were mentioned. The family history of low back
pain, the way of carrying school bag, the
time
spent walking to school, the
Although the
association between schoolbag weight and low back pain is strongly debatable
[5], the international recommendations limit the weight of the schoolbag
between 10% and 15% of the body weight [10,11]. The purpose of our work was to
study the prevalence and factors associated with low back pain in schools of
Ouagadougou, Burkina Faso.
PATIENTS AND METHODOLOGY
Sampling
We performed a
cross-sectorial, descriptive and analytical study that involved school children
of 6 to 16 years old. Two schools (one public and one private) were picked
randomly in the city of Ouagadougou.
The minimum
size of our sample was calculated according to Schwartz's formula:
n0
≥ [Zα 2 f(1-f))/l2 ]g(1+t)
n0 is the
minimal size of the desired sample;
zα is a
coefficient that measures accuracy. Considering a risk error α=0.05 we will
have zα=1.96;
l is the absolute error
margin on the estimate of the proportion. For this study, it is recommended to
consider l=0.05;
f is the approximate value
of the key variable of the study. The value of f was 12.3 which is the
prevalence of low back pain according the study of Ngongang et al. [9] in
Cameroon;
g is the cluster effect or
survey plan effect, in Africa, it is between 2 and 3;
t is the expected
non-response rate. It is better to anticipate a non-response rate of 10%.
![]() 𝑛 ≥364≥ [(1,96)2×0,123(1-0,123)/(0,05)²]
2 (1+0,1) => 𝑛
≥364
𝑛 ≥364≥ [(1,96)2×0,123(1-0,123)/(0,05)²]
2 (1+0,1) => 𝑛
≥364
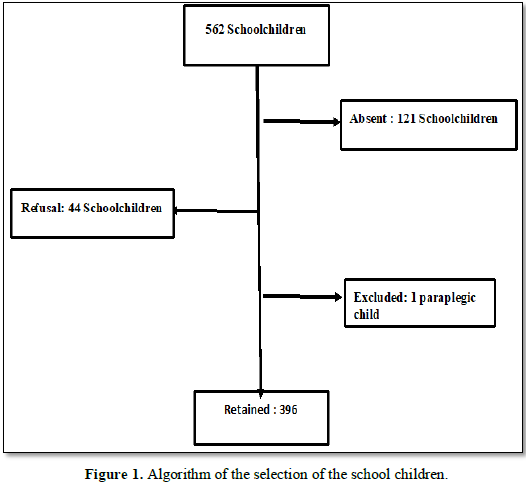
The minimum
size of our sample=364 school children. Figure
1 showed algorithm of the selection of the school children.
Criteria
Our study
included: all school children of both genders, attending the designated
institutions, in 2nd, 3rd, 4th and 5th
grades, carrying a school bag.
The following
have been excluded: any consenting school child but for whom we have not received
parental permission, any non-consenting child, any paraplegic school child. School children having difficulty to answer questions due to drug
treatment or brain disease, school children absent and those who refused to
participate, were also excluded.
Study variables and tools
The following variables were studied:
- Socio-demographic characteristics: age,
sex, class, means of transportation, type of school (private or public),
residence, type of house (flat or story building);
- The way of life: availability of running
water, domestic work, concept of field work, concept of smoking, notion of
alcoholism, practice of competitive sports, the regular way of moving from home
to school, distance from home to school, the time spent between home and school;
- The clinical characteristics: weight,
height, body mass index (BMI), pain intensity assessed by a visual analogue
scale (VAS) (mild pain: EVA=1, 2, 3; moderate pain: EVA=4, 5, 6; Severe pain:
EVA=7, 8, 9, 10);
- The weight of the bag and the percentage of the weight of the schoolbag relative to the schoolchild’s body weight
(weight
of schoolbag / weight of schoolchild) *100
- Family antecedents: notion of low back pain
of a parent, alcoholism in a parent, smoking by one of the parents.
Data collection
A letter was
sent to the managers of the selected institutions in order to first explain the
study and to have their authorizations to contact students and their parents.
Following that, we conducted an interview with the managers and teachers of the
institutions on the objectives and the progress of the study. Thirdly, we sent
the parents of the school children a letter and a request for consent and
assent. The school children from whom we have received the parents’ consent
received a copy of the questionnaire that was appropriate for their level of
understanding, helped by emoticons and diagrams to facilitate understanding,
with clear explanations given for each question to the school children. A
questionnaire was also administered to theirs parents. The school children were
then individually led by the teachers to the selected place of examination and
set up for this purpose within the school;
The physical
examination was performed individually by senior rheumatologists in the
presence of the teachers of each student respecting the privacy of each child.
STATISTICAL ANALYSES
All the data
from each schoolchild were collected on a survey sheet.
The data was recorded and processed using the Epi
Info 7 software. The data was then analyzed using the
XLSTAT 2007 software. The quantitative variables were presented according to
the central tendency and dispersion parameters and the qualitative variables in
numbers and percentages. In a bivariate analysis, the qualitative variables
were compared using the Chi2 test and Fisher’s exact probability.
Quantitative variables were compared using the Student’s T-test. The
multivariate logistic regression test was used to determine factors associated
with low back pain based on socio-demographic and clinical data. The odd ratio
and its confidence interval made it possible to quantify the association.
Differences were considered significant for (p<0.05).
ETHICAL CONSIDERATION
The study was
approved by the ethics committee of establishment of the Bogodogo teaching
hospital. The authorizations of the managers of the various institutions as
well as those of the parents of the students chosen for our study were
obtained. Only consenting students were examined. Cases of low back pain
needing treatment and any other rheumatologic infection needing treatment were
taken care at the Rheumatology ward of the Bogodogo teaching hospital. An
explanation was given to each schoolchild about his/her pathology.
Confidentiality of data was respected during data collection. The anonymity of
the data has been respected.
RESULTS
General characteristics of school children
Three hundred
and ninety-six (396) schoolchildren were included in the study. Figure
1 shows the algorithm of the selection for our sample. There were 202 (51%)
boys and 194 (49%) girls, a sex ratio of 1.04. The average age of
schoolchildren was 10 ± 2.07 years with extremes at 6 and 16 years. Two hundred
and ninety-eight (75.25%) had a normal BMI, 45 (11.36%) were overweight and 53
(13.38%) were underweight. Low back pain in one parent was reported in 129
(32.58%) school children.
School bag weight
The
average weight of the backpack was 3 ± 1.48 kg. 153 (38.6%) had a bag weighing
10% or more of their body weight and 41 (10.35%) had their bags weighing more
than 15% of their body weight.
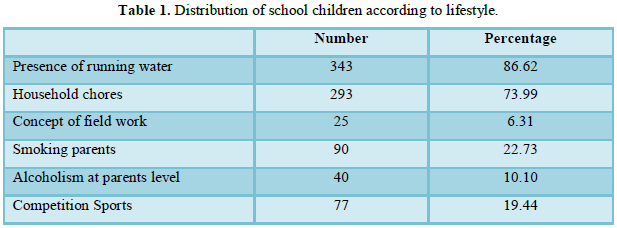
Lifestyle
Household
chores were carried out by 293 (73.99%) of the school children. Table 1 shows the distribution of
school children by lifestyle.
Characteristics of school children with low back
pain
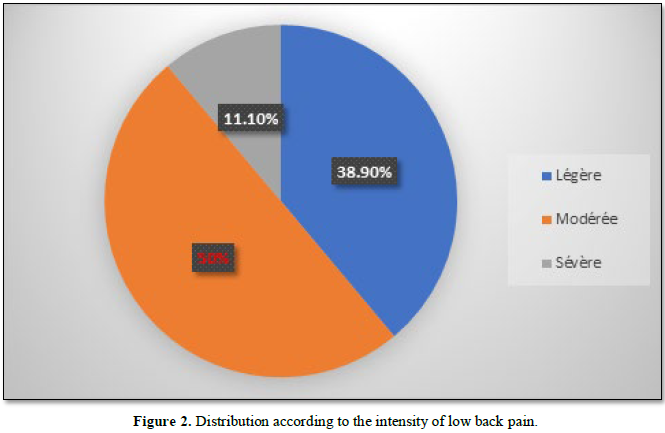
Prevalence and characteristics of school children
with low back pain: 36(9.1%) school children had low back
pain. Their average age was 9.3 ± 1.87 years with extreme ages at 6 and 14
years. In among them, 10 (28.78%) school children’s low back pain had already
required a medical consultation. 18 school children (50%) complained of low
intensity lumbago. Figure 2 shows
the distribution of children by pain intensity.
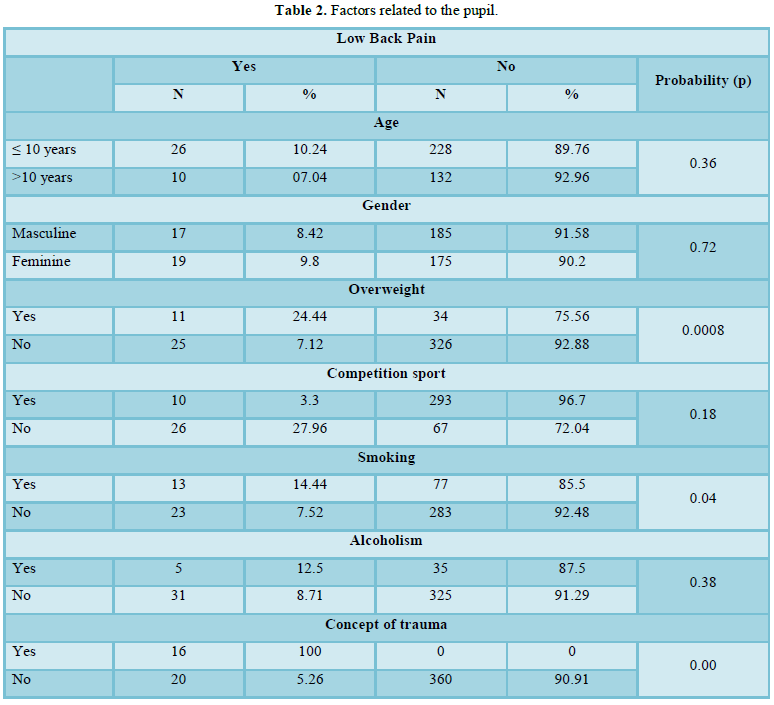
Risk factors
Factors related to the school child: 11 (24.44%) overweight children had low back pain compared to 25
(7.12%) children with normal weight (p=0.0008). The breakdown by student
factors is shown in Table 2.
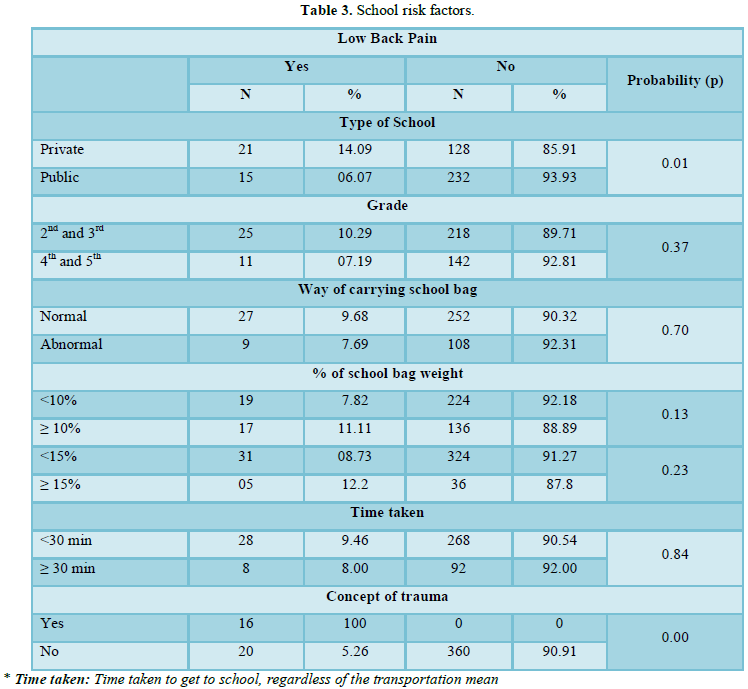
School factors: The
prevalence of low back pain was significantly higher in the private school
(14.09%) than in the public school (6.07%) (p=0.01). Table 3 summarizes the school risk factors for low back pain.
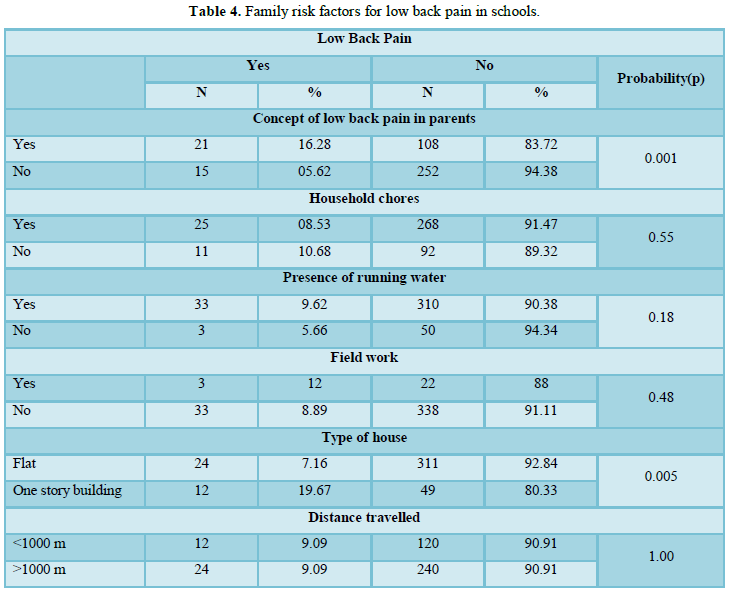
Family factors: Among
children with a family history of low back pain, 21 (16.28%) had low back pain
compared to 15 (5.62%) in among those with no family history of low back pain
(p=0.001).
The distribution of
children with low back pain according to family risk factors for low back pain
is shown in Table 4.
Multivariate analysis of risk factors: In a multivariate analysis, children who lived in one-story homes and
had parents smoking with low back pain had significantly higher risks of having
low back pain than other children (Table
5).
DISCUSSION
The prevalence of low back pain was 9.1% in
our series. In a univariate analysis, overweight, family history of smoking,
school type (private), low back pain of a parent and type of home (one story
house) were the factors associated with low back pain in schools. In a
multivariate analysis, only the type of house (one story house), smoking by a
parent and low back pain of a parent were the risk factors for low back pain in
school children with odd ratios of 3.06, 3.52 and 2.69, respectively.
The prevalence of low back pain in schools
ranges from (8% to 74%) depending on the age group and the weight of the school
bag [5-7,12]. The prevalence reported in our series appears to be the lowest in
sub-Saharan Africa; indeed, in Cameroon, Chiedjio [9] reported a prevalence of
12.3% in a population of 1,075 school children with an average age of 11 years;
in Uganda, Mwaba et al. [8] reported a prevalence of 37.8% of low back pain in
a population of 532 school children with an average age of 13.6 years; Ayanniyi
et al. [6] found a prevalence of 25% of low back pain in 3185 school children
with an average age of 15 years and predominantly adolescents (64% between 14
and 16 years) in Nigeria. The difference observed in terms of prevalence with
our series (9.1%) could be due to the profile of the study populations
(elementary and average courses, average age of 10 years ± 2.07 years) but also
to the specific risk factors. children, their environment and the weight of the
schoolbag. According to the literature, the intensity of low back pain was mild
to moderate [6].
Risk factors for low back pain in school children
are controversial [4,12-15]. Single-story home, passive smoking and low back
pain of a parent were the risk factors associated with low back pain in our
series after logistic regression and multivariate analysis; the weight of the
school bag was not statistically associated with low back pain.
The role of the
weight of the school bag is very controversial in the occurrence of low back
pain in school [5]. 153 school children (38.6%) had excess bag weight at (10%)
of body weight, thus failing to meet international guidelines [10,11]; this
frequency varies from (30.8% to 70%) in some African, European and American
series [6-9]. In a recently published systematic review, Yamato et al. [5] did
not find evidence of the role of the weight of the school bag in the occurrence
of low back pain in children and adolescents. The diversity of methodologies
used, the age groups studied and especially the scarcity of randomized and controlled
studies or longitudinal studies have been the limits of this review and cannot
lead to definitive conclusions [5]. Also, the hypothesis of excess weight of
the school bag (WESM) in the onset of low back pain in schools imposes a weight
limitation of the school bag to (10% or 15%) of the body weight by health
professionals [10].
Interestingly, the prevalence of low back
pain was higher in private schools than in public ones. Giutsi et al. [15] also
reported a higher prevalence of low back pain (68.5%) in private schools than
in public schools (9.3%). This association between low back pain and type of
school disappears in our series after a multivariate analysis. However, further
studies are needed to investigate the risk factors that may explain this high
prevalence of low back pain in the private sector.
Tobacco is known to be a risk factor for the
development of low back pain in adults [16]. Passive smoking has been a risk
factor (OR) in our series and in that of Cameroon [9] justifying awareness rising
of parents about passive smoking of children. Although the mechanism is not
well known, the association Between current smoking and the incidence of low
back pain was stronger in adolescents (OR 1.82, 95% CI, 1.42-2.33) than in
adults (OR 1.16, 95% CI, 1.02-1.32) [17].
Our study focused on low back pain in
schools. Some publications have shown that musculoskeletal disorders (63.4%)
associated with wearing a backpack predominate more on the shoulders (27.3%)
than on the back (15%) [18]. For other authors, the weight of the bag would be
associated with pain in the shoulders and wrists [11]. Other studies are needed
in our context to understand the psycho-social factors [4,19], all
musculoskeletal disorders, their impact on school results and their association
with the weight of the schoolbag for better management [20]. Our study, which
aimed to assess the prevalence and risk factors of low back pain in schools,
has limitations; in spite of a rigorous clinical examination, it is possible
that rough forms of juvenile ankylosing spondylitis are disregarded. Ankylosing
spondylitis is, however, a rare condition in our context because of the low
prevalence of carriage of HLA B27 [21].
CONCLUSION
Despite the
international recommendations, over a third of school children had schoolbag
with excess weight. Low back pain seems to be more common in the private
schools than in public ones. Factors such as the type of home, smoking by a
parent and low back pain of a parent were associated with a risk of developing
low back pain in schools. These data should be considered in educational campaigns for reducing
school equipment weight.
COMPLIANCE OF ETHICAL STANDARDS
Conflict of interest
None of the authors
have any potential conflict of interest.
Informed consent
We declare that
all school children and their parents gave informed consent prior to inclusion
in this study.
Ethical approval
This
cross-sectional study was approved by an institutional research ethics board.
1. Hoy
D, Bain C, Williams G, March L, Brooks P, et al. (2012) A systematic review of
the global prevalence of low back pain. Arthritis Rheum 64: 2028-2037.
2. Ouédraogo
DD, Ouédraogo V, Ouédraogo LT, Kinda M, Tiéno H, et al. (2010) Prevalence and
factors associated with low back pain among hospital staff in Ouagadougou
(Burkina Faso). Med Trop (Mars) 70: 277-280.
3. Kamper
SJ, Henschke N, Hestbaek L, Dunn KM, Williams CM (2016) Musculoskeletal pain in
children and adolescents. Br J Phys Ther 20: 275-284.
4. Kamper
SJ, Yamato TP, Williams CM (2016) The prevalence, risk factors, prognosis and
treatment for back pain in children and adolescents: An overview of systematic
reviews. Best Pract Res Clin Rheumatol 30: 1021-1036.
5. Yamato
TP, Maher CG, Traeger AC, William’s CM, Kamper SJ (2018) Do schoolbags cause
back pain in children and adolescents? A systematic review. Br J Sports Med 52:
1241-1245.
6. Ayanniyi
O, Mbada CE, Muolokwu CA (2011) Prevalence and profile of back pain in Nigerian
adolescents. Med Princ Pract 20: 368-373.
7. Bejia
I, Abid N, Ben Salem K, Letaief M, Younes M, et al. (2005) Low back pain in a
cohort of 622 Tunisian school children and adolescents: An epidemiological
study. Eur Spine J. 14:331-336.
8. Mwaka
ES, Munabi IG, Buwembo W, Kukkiriza J, Ochieng J (2014) Musculoskeletal pain
and school bag use: A cross-sectional study among Ugandan school children. BMC
Res Notes 7: 222.
9. Ngongang
A (2016) Prevalence and factors associated with low back pain in children in
school settings in the city of Doula (Thesis). Cameroon: University of Douala.
125 P. Available at http://www.em-consulte.com/en/article/1100123
10. Dockrell
S, Simms C, Blake C (2013) Schoolbag weight limit: can it be defined? J Sch
Health 83: 368-377.
11. Dianat
I, Javadivala Z, Asghari-Jafarabadi M, Asl Hashemi A, Haslegrave CM (2013) The
use of schoolbags and musculoskeletal symptoms among primary school children:
Are the recommended weight limits adequate? Ergonomics 56: 79-89.
12. Spiteri
K, Busuttil ML, Aquilina S, Gauci D, Camilleri E, et al. (2017) Schoolbags and
back pain in children between 8 and 13 years: A national study. Br J Pain 11:
81-86.
13. Onofrio
AC, da Silva MC, Domingues MR, Rombaldi AJ (2012) Acute low back pain in high
school adolescents in Southern Brazil: Prevalence and associated factors. Eur
Spine J 21: 1234-1240.
14. Watson
KD, Papageorgiou AC, Jones GT, Taylor S, Symmons DP, et al. (2003) Low back
pain in school children: The role of mechanical and psychosocial factors. Arch
Dis Child 88: 12-17.
15. Giusti
PH, De Almeida HL Jr, Tomasi E (2008) Weight excess of school materials and its
risks factors in South Brazil. A cross sectional study. Eur J Phys Rehabil Med
44: 33-38.
16. Shemory
ST, Pfefferle KJ, Gradisar IM (2016) Modifiable risk factors in patients with
low back pain. Orthopedics 39: e413-416.
17. Shiri
R, Karppinen J, Leino-Arjas P, Solovieva S, Viikari-Juntura E (2010) The
association between smoking and low back pain: A meta-analysis. Am J Med 123:
87.e7-35.
18. Dockrell
S, Simms C, Blake C (2015) Schoolbag carriage and school bag-related
musculoskeletal discomfort among primary school children. Appl Ergon 51:
281-290.
19. Trevelyan
FC, Legg SJ (2011) Risk factors associated with back pain in New Zealand school
children. Ergonomics 54: 257-262.
20. O'Sullivan
P, Smith A, Beales D, Straker L (2017) Understanding adolescent low back pain
from a multidimensional perspective: Implications for management. J Orthop
Sports Phys Ther. 47: 741-751.
21. Díaz-Peña
R, Ouédraogo DD, López-Vázquez A, Sawadogo SA, López-Larrea C (2012) Ankylosing
spondylitis in three Sub-Saharan populations: HLA-B*27 and HLA-B*14
contribution. Tissue Antigens 80: 14-15.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Journal of Allergy Research (ISSN:2642-326X)
- Chemotherapy Research Journal (ISSN:2642-0236)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)


