778
Views & Citations10
Likes & Shares
Spontaneous
rupture of the ureter is a very interesting and unusual phenomenon which
normally occurs due to ureteral obstruction. We present a case of spontaneous
rupture of the distal ureter, secondary to a ureteric calculus. Our patient
presented with a history of acute on chronic abdominal pain and was septic on
arrival to hospital.
Keywords:
Spontaneous, Distal ureteric calculi, Ureteric
rupture
INTRODUCTION
Spontaneous
rupture of the ureter is a rare urological occurrence with only a small number
of cases reported in the literature. It is defined as extravasation of urine
from the ureter which occurs without trauma or iatrogenic manipulation of the
ureter. It often occurs secondary to ureterolithiasis with urinary tract
obstruction and resultant increased intraluminal pressure and subsequent
rupture [1]. It may also be secondary to a tear of the ureter during passage of
the stone [2]. Published cases have reported pregnancy, ureteral strictures,
tumors, bladder outlet obstruction and retroperitoneal fibrosis among the
contributing causes. Peritoneal irritation by urine results in presentation
with an acute abdomen, sometimes without any urinary tract symptoms or
urinalysis abnormalities. Owing to its presentation it is often misdiagnosed as
appendicitis or diverticulitis [3]. Majority of reported incidents generally
involve the proximal ureter, renal fornix or pelviureteric junction [4]. It may
lead to urinoma, infection with sepsis, acute kidney injury and abscess
formation if left untreated [1]. Only hypothetical causes have been suggested
and thus, there are no recommended guidelines to aid management. Management
principles are based on the current condition of the patient including
diversion of urine, management of sepsis, followed by definitive treatment.
Placements of double-J stents or percutaneous nephrostomy for drainage provides
excellent results in the unwell patient, until definitive surgery can be performed.
Conservative management with antibiotics is recommended. Improved nutritional
status of the patient is imperative for post-operative recovery. We describe
the first reported case of spontaneous distal ureteric rupture, secondary to a
ureteric calculus.
CASE REPORT
A 25 year old
previously healthy female, presented at emergency surgical department, CHA with
complaining of severe abdominal pain associated with two episodes of vomiting
and chills and rigors. She denied any associated dysuria, hematuria or
frequency. On examination she was found to be tender in the lower abdomen. She
was given analgesia with little effect. A urinalysis revealed microscopic
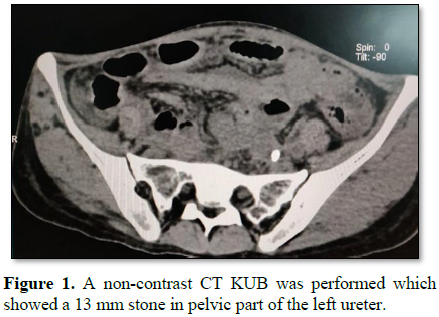
hematuria; whilst blood investigations were within normal limits. A contrast
Computed Tomography (CT) of the abdomen was performed and she was found to have
free fluid in the left retroperitoneum associated with obstruction of the left
kidney and ureter by a 13 mm calculus in left ureter distal to crossing of left
iliac vessels (Figures 1 and 2). This confirmed extravasation of
contrast medium around the left kidney and ureter. Suggestive of a perforation
of the left collecting system. A diagnosis of spontaneous left proximal
ureteric perforation secondary to urolithiasis was made. Blood tests, clinical
parameters and temperature were still well within normal limits, despite the
severity of symptoms and clinical examination. We opted to treat her with
percutaneous nephrostomy tube insertion. A 16 F urethral catheter was inserted
to avoid reflux. The patient was also started on intravenous antibiotic
piperacillin/
DISCUSSION
Spontaneous ureteral rupture is a
surprisingly rare condition. It is by definition non-traumatic in origin, and
can be difficult to diagnose unless a high index of suspicion for this
condition is maintained. The most common cause for spontaneous ureteral rupture
is obstructing ureteral calculi. Other reported rarer causes include tumor,
retroperitoneal fibrosis, pregnancy, connective tissue disorder and acute
urinary retention. The condition should be suspected in cases of ureteric colic
which develop significant acute worsening of symptoms, with increased areas of
tenderness, with or without a reactive peritonitis. Imaging is required to
confirm the diagnosis. Whilst ultrasound can be helpful in identifying a
perinephric or retroperitoneal fluid collection, the condition is best
diagnosed with a delayed CT scan post-intravenous contrast. This modality will
confirm a urinary leak and can accurately define the site of rupture. Coronal
reconstructions may further help in accurately identifying the site of leak.
The use of a delayed film post IV contrast is also very useful in
differentiating a ureteral rupture from an infective perinephric abscess that
can also arise from obstructing calculi. It can also differentiate from
forniceal rupture. Due to the rarity of this clinical condition, there are no
guidelines or recommendation on its’ management. We managed our patient with
insertion of a double-J ureteral stent which was then removed after 12 weeks.
On reviewing case reports of patients with this condition, the majority were
also managed with a double-J ureteral stent. Conservative management was
adopted in a smaller amount of patients. Percutaneous drainage with or without
nephrostomy/ante grade stent is another reported option [5,6]. Development of fever
or hemodynamic changes may indicate an infective process of the resulting
urinoma and antimicrobial therapy ± drainage needs to be considered. A high
serum creatinine may also be noted from reabsorption of the urinoma. On stent
removal, we performed an on table retrograde pyelogram to confirm there is no
residual leakage and also to exclude significant stricturing. A CT IVU after
stent removal may also be considered as an alternative to this approach.
Spontaneous
ureteric rupture is a rarely described medical event which is challenging to
diagnose. Urinoma or abscess formation may ensue, eventually leading to sepsis
and death. The definition of “spontaneous” has not been properly established
but our patient has never had previous ureteric instrumentation,
kidney/abdominal surgery or a history of external trauma. However, the presence
of obstructive pyonephrosis could also be secondary to a ureteral lesion, which
may eventually lead to ureteric rupture and extravasation of urine.
Due its rarity, there
are no recommended guidelines to direct management. Successful methods have
been described which include retrograde insertion of a double-J ureteric stent
and/or nephrostomy tube drainage both with the concurrent use of antibiotics
[7]. These conduits normally remain in
situ, until definitive surgery can be performed. For cases with no known
causes, conduits are removed once patients’ clinical state improves with
imaging consistent with resolution. In general, prompt intervention will reduce
both mortality and morbidity. Nevertheless, the general principles of
controlling sepsis take precedence prior to definitive surgery.
1.
Pampana E, Altobelli S,
Morini M, Ricci A, D’Onofrio S, et al. (2013) Spontaneous ureteral rupture
diagnosis and treatment. Case Rep Radiol 2013: 4.
2.
Der-Yen L, Ying-Chen F,
Da-Yi H, Sen-Ping L (2004) Spontaneous rupture of the ureter secondary to
urolithiasis and extravasation of calyceal fornix due to acute urinary bladder
distension: Four cases report. Chin J Radiol 29: 269-275.
3.
Szu-Yi L, Jiun-Nong L,
Ching-Yu H, I-Ting T (2011) Spontaneous rupture of the ureter mimicking acute
appendicitis: Two case reports. J Acute Med 1: 61-63.
4.
Pace K, Spiteri K
(2016) German Spontaneous proximal ureteric rupture secondary to
ureterolithiasis. J Surg Case Rep: 11: 1-3.
5.
Lang EK, Glorioso L III
(1986) Management of urinomas by percutaneous drainage procedures. Radiol Clin
North Am 24: 551-559.
6.
Behzad-Noori M, Blandon
JA, Negrin Exposito JE, Sarmiento JL, Dias AL, et al. (2010) Urinoma: A rare complication
from being between a rock and soft organ. El Paso Physician 33: 5-6.
7.
Porfyris O, Apostolidi
E, Mpampali A, Kalomoiris P (2016) Spontaneous rupture of renal pelvis as a
rare complication of ureteral lithiasis. Turk J Urol 42: 37-40.


QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Stem Cell Research and Therapeutics (ISSN:2474-4646)
- Dermatology Clinics and Research (ISSN:2380-5609)
- Journal of Alcoholism Clinical Research
- Journal of Spine Diseases
- Oncology Clinics and Research (ISSN: 2643-055X)
- Journal of Cardiology and Diagnostics Research (ISSN:2639-4634)
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)


