2550
Views & Citations1550
Likes & Shares
Purpose: To
report a rare case of spontaneous, direct, Type A Carotid cavernous fistula in
late pregnancy.
Observation: A 30
year old woman presented to us 1month postpartum, with right-sided headache,
progressive axial proptosis, total external ophthalmoplegia and diminution of
vision which started one day prior to term normal delivery. Magnetic Resonance
Imaging (MRI) and Digital Subtraction Angiography (DSA) confirmed direct
anomalous communication between the cavernous sinus and carotid artery system.
Conclusion: Carotid
Cavernous Fistula (CCF) may be associated with life and vision threatening
implications. Meticulous clinical and radiological evaluations are critical for
accurate diagnosis of this challenging condition. Not all CCF undergo
spontaneous resolution. Treatment modalities should be individualized depending
upon the rate of flow, type of shunt and stage of pregnancy. A high index of
suspicion is deemed necessary to prevent delayed and missed diagnosis.
Keywords: Carotid cavernous fistula,
Pregnancy, Direct, Proptosis, Diminution of vision, Chemosis
Abbreviations: MRI:
Magnetic Resonance Imaging; DSA: Digital Subtraction Angiography; CCF: Carotid
Cavernous Fistula; ICA: Internal Carotid Artery; ECA: External Carotid Artery;
RE: Right Eye; LE: Left Eye
INTRODUCTION
Anomalous
communication between the carotid artery and cavernous sinus is known as
carotico-cavernous fistula (CCF) [1]. Angiographically, they can be classified
as direct; if the shunt is directly with the internal carotid artery (ICA) or
indirect (dural) if the communication is with meningeal branches of ICA or
external carotid artery (ECA) [2]. Pregnancy is a known precipitator of
spontaneous CCF [3]. Haemodynamic and hormonal changes in pregnancy can lead to
enlargement of aneurysm or devastating complications like cerebral hemorrhage
[3-5]. Indirect CCF is a documented but rare condition in pregnancy comprising
of limited number of reports in the literature [3,6,7]. A spontaneous Direct
Type A Carotid Cavernous fistula is even rarer. We report such a case of
angiographically confirmed direct CCF in a young female presenting with rapid
onset proptosis in the peripartum period.
CASE PRESENTATION
A 30 years old
woman presented to us with history of Right sided headache and outward
protrusion of Right eye (RE) since 1 month. Her symptoms started a day prior to
full term normal vaginal delivery at home. Thereafter, it progressed gradually
along with onset of proptosis, dizziness and vomiting.
There was no
anteceding history of trauma, convulsion or limb weakness. Baby was born
healthy and growing well.
Prior to presenting
to us, she was treated with intravenous antibiotics with the suspicion of
Orbital cellulitis without any improvement.
Blood pressure was recorded as 110/80 mm
Hg. Pallor was present. Systemic examination was unremarkable.
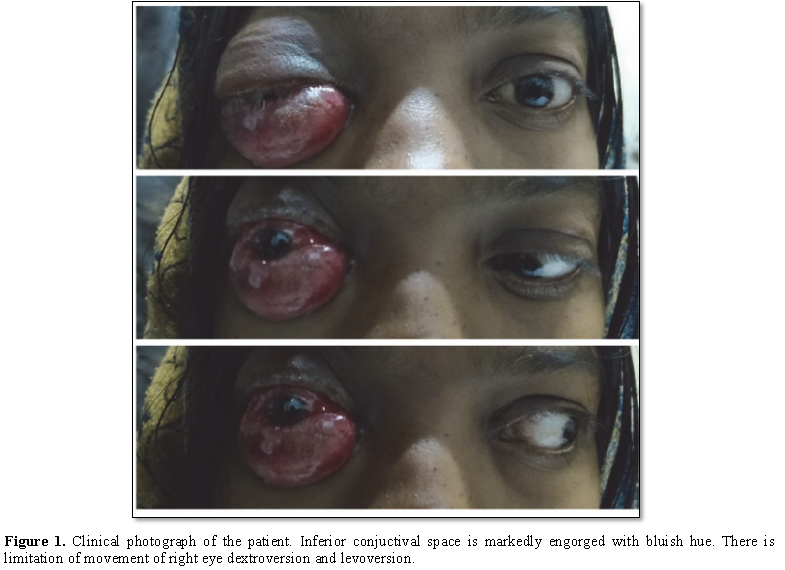
Ocular examination revealed best corrected
visual acuity of 20/200 in the RE and 20/20 in left eye (LE). There was
presence of RE proptosis measuring 25 mm on Hertels exophthalmometer. Proptosis
was axial, non-tender, non-compressible, non-pulsatile and not associated with
bruit. There was complete limitation of extra ocular movements along with
lagophthalmos. Inferior subconjuctival space was severely engorged with bluish
hue (Figure 1). Anterior segment was
unremarkable. Fundus examination revealed hyperaemic disc with well-defined
margins. Peripapillary choreo-retinal striae were noted. Goldmann applanation
tension was 17 mm Hg in both eyes.
Contrast Enhanced Computed Tomography of
orbit was ordered which revealed RE proptosis, dilated tortuous vessels in
retrobulbar region, prominent Right cavernous sinus with convex lateral margin.
Further Magnetic Resonance (MRI) Imaging displayed Right CCF with dilated right superior ophthalmic vein (Hockey stick sign) [1] showing prominent flow voids with significant RE proptosis (Figure 2).
Digital Substraction Angiography (DSA) confirmed direct CCF with venous engorgement of orbit. Venous drainage via Right superior ophthalmic vein anteriorly, right inferior petrosal sinus posteriorly, superficial middle cerebral vein superiorly and minimal reflux into ipsilateral pterygoid plexus. Poor arterial collaterals to right hemisphere via PCOM and ACOM were noted (Figure 3).
Patient was advised endovascular coiling of
right CCF which she refused because of financial constraint and thereafter she
failed to turn for follow up.
DISCUSSION
CCF comprises one or more anomalous
arteriovenous communication between the cavernous sinus (CS) and the carotid
arterial system [1]. These lesions can be classified on basis of aetiology as
traumatic and spontaneous, haemodynamically as high and low flow [2]. 25% of
them are spontaneous fistulas [1]. Angiographically, it can be classified into
four types. Type A is direct connection between ICA and CS. Type B, C and D are
dural shunts in which there is anomalous connection of CS with meningeal branch
of ICA, ECA and both, respectively [2]. Spontaneous low flow system is commonly
associated with pregnancy [1]. However, our patient presented with spontaneous
high flow fistula which has rarely been reported.
Pregnancy, physical straining,
atherosclerosis and collagen vascular disease is well known precipitator of
these anomalous arterio-venous shunts [3,7]. Pregnancy is characterized by
hemodynamic and hormonal changes which make the vessel wall leaky leading to
aneurysm formation, enlargement, rupture and fistula formation [8]. Blood
pressure of our patient was constantly normal throughout pregnancy and
postpartum.
Usually 25 to 30% of the pregnant woman
present with this condition in the late third trimester or during delivery
because of increased cardiac output [3,5,9]. Similarly, in our patient, symptom
first appeared a day prior to delivery and continuously progressed thereafter.
Commonly, presenting clinical signs are
proptosis (81%), diplopia (68%), cranial bruit (49%), headache (34%) and
chemosis (87%) [9,10]. Our patient presented with proptosis, chemosis,
oculomotor paresis and visual loss. This was not associated with any history of
head injury. Such patients may be misdiagnosed with infectious and
non-infectious conditions. Headache is a common complaint among pregnant women
which should not be neglected without detailed evaluation if warranted.
There are reported instances of
complications like rapid enlargement of aneurysm or rupture of aneurysm leading
to subarachnoid haemorrhage in 1 in 10000 pregnancies [4,5,11]. Intracerebral
haemorrhage can lead to fetal and maternal morbidity and mortality [12]. Our
patient did not develop any hemorrhage.
Spontaneous resolution is known in 5 to 60%
of the cases [5,6]. Hirata et al. [3] described a case of marked regression of
a CCF 2 to 3 days after delivery and speculated that spontaneous improvement in
CCF after pregnancy was due to thrombosis related to changes in blood
coagulation that occur during pregnancy and delivery. Unfortunately our patient
did not resolve spontaneously and her symptoms progressively deteriorated till
the time of presentation.
Weather to deliver a child vaginally or by
caesarean section is still a matter of debate. Some authors have suggested
caesarean delivery to avoid valsalva maneuver induced raised intraocular
pressure [7,13].
Barrow et al. [2] proposed the following as
indications for treatment of a spontaneous CCF: (1) visual deterioration; (2)
obstructive diplopia related to vascular engorgement and enlargement of the
extra-ocular muscles or neural compression within the cavernous sinus; (3)
intolerable bruit or headache; and (4) malignant proptosis with untreatable
corneal exposure.
The timing of treatment should be decided
according to the presentation. Cases presenting with complication in early or
mid-third trimester may warrant need for immediate delivery, even preterm [12].
It has been suggested that pregnancy towards term should be dealt with delivery
of child first followed by treatment as involves exposure of infant to
irradiation. Timing of treatment following delivery may vary as early as 1 day
post-partum to 7 weeks post-delivery [7,14]. Detachable balloon and Endovasular
coiling is a documented successful treatment option [7,14]. There is a case
report of successful treatment with craniotomy and occlusion of ICA during
pregnancy but the patient delivered preterm [12].
CONCLUSION
Spontaneous, direct CCF during pregnancy is
a rare condition. It may be associated with life and vision threatening
implications. Meticulous clinical and radiological evaluations are critical for
accurate diagnosis of this challenging condition. Not all CCF undergo
spontaneous resolution. Treatment modalities should be individualized depending
upon the rate of flow, type of shunt and stage of pregnancy. A high index of
suspicion is deemed necessary to prevent delayed and missed diagnosis.
1.
Das
JK, Medhi J, Bhattacharya P, Borah N, Bhattacharjee K, et al. (2007) Clinical
spectrum of spontaneous carotid-cavernous fistula. Indian J Ophthalmol 55:
310-312.
2.
Barrow
DL, Spector RH, Braun IF, Landman JA, Tindall SC, et al. (1985) Classification
and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg 62:
248-256.
3.
Hirata
Y, Matsukado Y, Takeshima H, Seto H (1988) Postpartum regression of a
spontaneous carotid-cavernous fistula - Case report. Neurol Med Chir (Tokyo)
28: 673-676.
4.
Weir
BK, Drake CG (1991) Rapid growth of residual aneurismal neck during pregnancy.
Case report. J Neurosurg 75: 780-782.
5.
Lin
TK, Chang CN, Wai YY (1992) Spontaneous intracerebral hematoma from occult
carotid-cavernous fistula during pregnancy and puerperium. Case report. J
Neurosurg 76: 714-717.
6.
Toya
S, Shiobara R, Izumi J, Shinomiya Y, Shiga H, et al. (1981) Spontaneous
carotid-cavernous fistula during pregnancy or in the postpartum stage. J
Neurosurg 54: 252-256.
7.
Yeung
SW, Suen SSH, Yu SCH, Lao TT, Leung TY, et al. (2013) Spontaneous carotid
cavernous fistula complicating pregnancy. Hong Kong Med J 19: 258-261.
8.
Marshman
LA, Aspoas AR, Rai MS, Chawda SJ (2007) The implications of ISAT and ISUIA for
the management of cerebral aneurysms during pregnancy. Neurosurg Rev 30: 17.
9.
Walker
AE, Allegre GE (1956) Carotid-cavernous fistulas. Surgery 39: 411-422.
10.
Meyers
PM, Halbach VV, Dowd CF, Lempert TE, Malek AM, et al. (2002) Dural carotid cavernous
fistula: Definitive endovascular management and long-term follow-up. Am J
Ophthalmol 134: 85-92.
11.
Ortiz
O, Voelker J, Eneorji F (1997) Transient enlargement of an intracranial
aneurysm during pregnancy: Case report. Surg Neurol 47: 527-531.
12.
Raskind
R, Johnson N, Hance D (1977) Carotid cavernous fistula in pregnancy. Angiology
28: 671-676.
13.
Lawrence
MS (2003) Effects of bending, lifting and valsalva maneuver on intraocular
pressure. Invest Ophthalmol Vis Sci 44: 1297.
14.
Dogan
S, Salman MC, Deren O, Geyik S (2012) Carotid-cavernous fistula in term
pregnancy due to spontaneous rupture of carotid-cavernous aneurysm. J Obstet
Gynecol 38: 427.


QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Clinical Case Studies and Reports (ISSN:2641-5771)
- Journal of Spine Diseases
- International Journal of AIDS (ISSN: 2644-3023)
- Dermatology Clinics and Research (ISSN:2380-5609)
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- International Journal of Surgery and Invasive Procedures (ISSN:2640-0820)
- Stem Cell Research and Therapeutics (ISSN:2474-4646)


