2728
Views & Citations1728
Likes & Shares
Orbit is a small complex anatomic space that contains important
structures, ocular globe, extrinsic muscles, cranial nerves, blood vessels,
fat, lacrimal gland. In presence of orbital tumors it is mandatory to use a
surgical approach that allows to achieve an adequate surgical field while
preserving neurological function. Neuronavigation is the set of
computer-assisted technologies used to guide or "navigate” the edges of
the tumor to allow the surgeon during resection or biopsy. This technology started
with use of CT data to get some landmarks of human anatomy defined “targets”
that could be readily used in surgery. Finally, the evolution of modern
neuroimaging technologies such intraoperative CT and MRI boosted the surgery
accuracy. In order to identify advantages and practical use of these
technologies we performed a nonsystematic review of the current literature
using the keywords “orbital tumor or orbital neoplasia or orbital mass or
orbital lesion” and “neuronavigation or navigation” published in last 10 years.
We evaluated 29 papers and we can conclude that navigation in orbital surgery
helps to reduce surgical damage while at the same time, allowing a more radical
tumor resection. CT and MRI scans are complementary in diagnosing and in
intraoperative navigation allow the surgeon to avoid and preserve vital
structures, particularly in a complex surgical procedure without real
anatomical landmarks for intraoperative orientation. Future is going towards
rapid changes and the integration with intraoperative procedures is carrying on
to new technologies further our contemporary bounds.
Keywords: Orbital tumor, Orbital surgery,
neuronavagation, Intraoperative computer tomography, Intraoperative magnetic
resonance
Abbreviations: MRI:
Magnetic Resonance Imaging; iMRI: Intraoperative Magnetic Resonance Imaging;
CT: Computer Tomography; iCT: Intraoperative Computer Tomography; NNS:
Neuronavigation System; FNAB: Fine-Needle Aspiration Biopsy; ENT: Ear, Nose and
Throat Doctors
INTRODUCTION
The orbit is a quite small, “interdisciplinary” region, being area of
interest of many specialists, such as ophthalmologists, ENT (ear, nose and
throat) doctors, endocrinologists, neurosurgeons, plastic surgeons and
maxillofacial surgeons. Orbital tumor can be a benign tumor or a malignant
tumor that can affect all components of the ocular globe, orbital walls,
extrinsic muscles, cranial nerves, blood vessels, fat, lacrimal gland. Surgical
access (in order to perform biopsy. FNAB or resection), especially in case of
intraconal lesions, may be demanding. The ocular globe and the maintenance of
its function are the major points of interest whichever treatment is used. In
case of orbital tumor the main goal of surgery is to achieve the maximum extent
of resection while preserving neurological function. In last year’s usage of
iMRI, iCT and neuronavigation systems has been proven to be highly accurate in
the resection of intracranial neoplasms [1-3]. In an effort to improve
resection safety, this combination has begun to be applied to approach orbital
tumors, providing better safety and effectiveness compared to standard
endoscopic or microscopic approach, even if prolonged surgical time has been
reported by some authors [3].
MATERIALS
AND METHODS
In order to identify advantages and disadvantages of these approaches we performed a nonsystematic review of the current English
literature using PubMed database. The search strategy was to include all
published articles involving the keywords “Orbital tumor or orbital neoplasia
or orbital mass or orbital lesion” and “neuronavigation or navigation”
published in last 10 years. No systematic or Cochrane reviews or meta-analyses
were found on the topic. In first screening 66 items were included and after
first round search we included 29 paper on the review. We excluded five case
reports [4-8] and one paper that had only abstract wrote in English [9].
DISCUSSION
Neuronavigation systems
Intraoperative navigation was
introduced in head and neck surgery more than 20 years ago in order to reduce
overall operation time, making radical tumor surgery more reliable and allowing
safer manipulations in close proximity to delicate structures. Small or
minimally invasive approaches allow only limited exposure and are a promising
field for intraoperative navigation systems. The main problem is the
topographic changes caused by surgery resulting in discrepancies between the
preoperative image data and the surgical site [10-12]. The application of
neuronavigation in cranio-orbital neurosurgery has been rarely reported
[13-15]. Enchev et al. [16] described 9 papers in the literature that describe
the application of neuronavigation in this field; most cases are concerning
with orbital reconstruction following post traumatic injury. In this survey
navigation has demonstrated to be useful to improve the accuracy in restoration
of orbital volume [17-20]. Nevertheless, at today only few studies report the
effectiveness of this technique in orbital tumors removal. Using this approach,
eventually in combination with the surface scanning systems using a Class I
laser device, thanks to the use of microsurgical techniques, orbital lesions
can be excised in very direct surgical routes, mostly without intracranial
invasion or significant external facial incisions. In addition, it has been
assessed that the so-called “brain-shift”, that in brain procedure is reported
to increase inaccuracy, is unimportant in case of orbit surgery, since in this
case the surgical targets are fixed structure (bone), so that intraoperative
anatomical localization at the state of the surgery was found to be accurate
and to remain stable during operative time [21]. Obviously, in order to prevent
major shift in the position of the orbital structures at the beginning of
surgery, the aspiration or opening of cystic components of the lesion before
finding and identifying of the borders must be avoid. Surgical time is not
significantly prolonged and due to the fact that operative manipulation and
trauma of intra orbital structures is reduced, the benefits of the procedure
balance the relative additional operative time required [21]. Sieskiewic et al.
[22] described the use of NNS associated with endoscopic trans-nasal approach
to facilitate localization and biopsy of intra orbital tumors, in particular in
case of small, retro bulbar tumors, limiting the extent of opening of medial
orbital wall and relative prolapse of intra orbital tissue into nasal cavity.
The use of neuronavigation and endoscopic trans-nasal approach has been
reported to be effectiveness also in case of intraconal cavernous hemangioma
[23]. Different techniques in order to plan NNS are described [24]. The use of
CT and MRI combined to obtain exact extension of the lesion was described: all
patients included in Hejazi’s study underwent neuronavigation assisted
microsurgical removal of the lesions [21]. Access was planned preoperatively on
a workstation monitor, and the automatic fusion of image sets (CT, MRI
T1-weighted and MRI T2-weighted) demonstrated to be important and helpful in
order to identify the exact extension of the lesions. Hejazi at al. describe
the complete removal of the lesion performed via a frameless navigation-aided
trans-conjunctival approach in the treatment of orbital lymphoma [25]. 11 cases
with lymphomas located in the intraconal front or anterior compartment of the
orbit. In seven cases, the frameless neuronavigation technique was used in
combination with the transconjunctival approach or with the pterional approach;
they described a low rate of ocular complications, including corneal injuries
in particular in patients with Corneal Dystrophies [26].
Combined neuronavigation system
With the use of intraoperative imaging-based neuronavigation the
topographic changes caused by surgery resulting in discrepancies between the
preoperative image data and the surgical site are eliminated. In addiction it
allows for control of resection; Terpolilli et al. [1] reported that in more
than half patients, included in their study, tumor removal was extended after
the intraoperative control, indicating that iCT significantly influenced extent
of excision. Finally, iCT with intraoperative navigation-guided system is
effective to assess if the orbital reconstruction re-establishes orbital volume
and globe projection in subjects with post-ablative orbital defects. In fact it
has demonstrated to be a viable tool to assist the surgeon even during the
reconstruction. Heiland et al. [10] described their experience about orbital
surgery, including removal of foreign bodies, which is an effective application
of intraoperative navigation. From their point of view, further promising
indications include extended or recurrent tumors because of altered anatomy
with lost landmarks during surgery. Software advancements should allow not only
marking of certain structures but simulation of their shifting. In combination
with intraoperative imaging, the surgical result could be verified in the sense
of quality management. Flat panel detector CT(FD-CT) and associated navigation
software have been used to safely and accurately guide percutaneous
interventions during the treatment of intra orbital vascular malformation
(low-flow and high-flow lymphatic and vascular malformations). The use of
trans-arterial or percutaneous embolization is well established for vascular
malformations and hyper-vascular masses within the head and neck. The use of CT
guidance improves accuracy, especially with regard to bony structures, although
this can be insufficient in soft tissue differentiation. In light of these
limitations, a three-dimensional image overlay technique has been developed for
FD-CT systems whereby an existing MR examination can be accurately superimposed
into a FD-CT combining the detailed bony detail of CT with the soft tissue
definition of MR [27]. Nesbit et al. [28] described their experience using
integrated cone-beam CT and fluoroscopic navigation in treatment of head and
neck vascular malformations and tumors in 27 patients, 5 of these with intra
orbital localization. This technique demonstrated to allow more accurate
trajectory planning and needle location, those are critical for the success of
embolization treatment, avoiding complications. Reinbacher et al. [29]
developed a method for a minimal-invasive biopsy of an intraconal lesion using
a 3D navigation system based on combined technique of hardware fusion between
18F-FDG Positron Emission Tomography (18F-FDG PET), magnetic resonance imaging
(MRI) and Computed Tomography (CT). They presented 6 patients with a total of 7
intra orbital lesions; all patients underwent fine-needle aspiration with
intraoperative image-guided navigation. They demonstrated that the lesion was
reached on the first pass in five lesions attempt, underlining that there has
not been an increase in operating times with the use of NNS. Intraoperative-MRI
resection control is also described. MRI imaging is advantageous due to the
absence of exposure to x-rays. However, iMRI is quite time consuming, requires
a dedicated operating theater and operating room equipment and is significantly
more costly than CT [1,30]. Future could be the use of new advanced techniques in
NNS like O-arm System (Medtronic Inc., Minneapolis, Minnesota, USA) currently
already used in trans-nasal endoscopic cranial base surgery. With the O-arm
assisted technique the images obtained localizes the tumor during the surgery
the real time, images are transferred to the neuronavigation workstation, where
they are merged with preoperative CT and/or MRI [31].
CONCLUSION
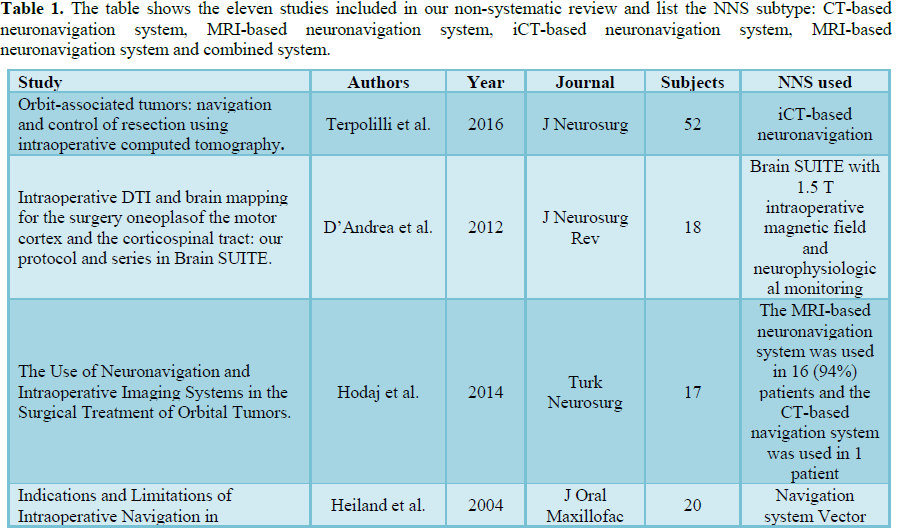
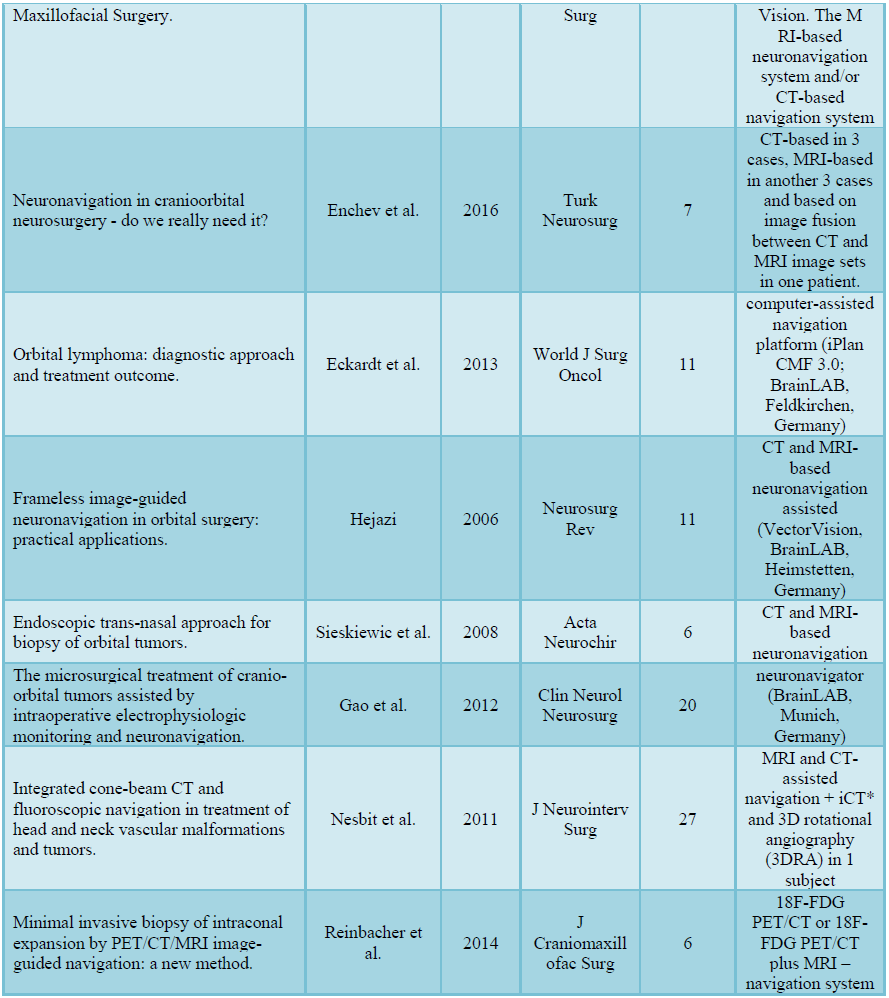
In presence of orbital tumors it is mandatory to use a surgical approach that allows achieving an adequate surgical field while preserving neurological function. NNS eventually combined with intraoperative imaging provide better safety and effectiveness compared to standard endoscopic or microscopic approach in more complex cases. In Table 1, are listed all the studies included in our review that use NNS, we have excluded five case report [4-8], one paper that had only the abstract wrote in English [9] and case series that include less than five patients and we have indicated the NNS subtype; for example CT-based or MR-based neuronavigation system. Neuronavigation system was considered accurate for the studies included in this nonsystematic review. However, the quality of these eleven papers show that randomized clinical trials are needed to compare NNS to conventional planning in the surgery intra orbital tumors, in terms of accuracy and operating time to get a high level of evidence to allow us to draw certain indications (Table 1).
1.
Terpolilli
NA, Rachinger W, Kunz M, Thon N, Flatz WH, et al. (2016) Orbit-associated
tumors: Navigation and control of resection using intraoperative computed
tomography. J Neurosurg 124: 1319-1327.
2.
D’Andrea
G, Angelini A, Romano A, Di Lauro A, Sessa G, et al. (2012) Intraoperative DTI
and brain mapping for the surgery oneoplas of the motor cortex and the
corticospinal tract: Our protocol and series in BrainSUITE. Neurosurg Rev 35:
401-412.
3.
Hodaj
I, Kutlay M, Gonul E, Solmaz I, Tehli O, et al. (2014) The use of
neuronavigation and intraoperative imaging systems in the surgical treatment of
orbital tumors. Turk Neurosurg 24: 549-557.
4.
Eckardt
AM, Rana M, Essig H, Gellrich NC (2011) Orbital metastases as first sign of
metastatic spread in breast cancer: Case report and review of the literature.
Head Neck Oncol 3: 37.
5.
Scolozzi
P, Bijlenga P (2017) Removal of recurrent intraorbital tumour using a system of
augmented reality. Br J Oral Maxillofac Surg 55: 962-964.
6.
Lübbers
HT, Jacobsen C, Könü D, Matthews F, Grätz KW, et al. (2011) Surgical navigation
in cranio-maxillofacial surgery: An evaluation on a child with a
cranio-facio-orbital tumour. Br J Oral Maxillofac Surg 49: 532-537.
7.
Netuka
D, Masopust V, Belšán T, Profantová N, Beneš V (2013) Endoscopic endonasal
resection of medial orbital lesions with intraoperative MRI. Acta Neurochir
155: 455-461.
8.
Novelli
G, Gramegna M, Tonellini G, Valente G, Boni P, et al. (2016) Orbital
osteoblastoma: Technical innovations in resection and reconstruction using
virtual surgery simulation. Craniomaxillofac Trauma Reconstr 9: 271-276.
9.
Lagrèze
WA, Rössler J, Illerhaus G, Maier W, Grosu A (2011) Therapy of tumors of the
anterior orbit. Ophthalmologe 108: 519-530.
10.
Heiland
M, Habermann CR, Schmelzle R (2004) Indications and limitations of
intraoperative navigation in maxillofacial surgery. J Oral Maxillofac Surg 62:
1059-1063.
11.
Siessegger
M, Mischkowski RA, Schneider BT, Krug B, Klesper B, et al. (2001) Image guided
surgical navigation for removal of foreign bodies in the head and neck. J
Craniomaxillofac Surg 29: 321-325.
12.
Marenco
M, Vellone V, Scuderi L, Moramarco A, Cascone P, et al. (2015)
Neuronavigational approach for orbital neurofibroma excision: A case report. J
Clin Exp Ophtalmol 6: 6.
13.
Kamizono
K, Yoshida S, Cho B, Matsumoto N, Fukushima J, et al. (2015) Safe and rapid
contouring of fibro-osseous lesions in the orbital area using navigation with
minimally invasive cranial bone registration. J Laryngol Otol 129: S62-S68.
14.
Lee
KY, Ang BT, Ng I, Looi A (2009) Stereotaxy for surgical navigation in orbital
surgery. Ophthalmic Plast Reconstr Surg 25: 300-302.
15.
Yu H,
Shen SG, Wang X, Zhang L, Zhang S (2013) The indication and application of
computer-assisted navigation in oral and maxillofacial surgery-Shanghai's
experience based on 104 cases. J Craniomaxillofac Surg 41: 770-774.
16.
Enchev
Y, Tzekov C, Ferdinandov D, Cekov A, Spiriev T (2011) Neuronavigation in
cranioorbital neurosurgery - Do we really need it? Turk Neurosurg 21: 119-26.
17.
Bell
RB, Markiewicz MR (2009) Computer-assisted planning, stereolithographic
modeling and intraoperative navigation for complex orbital reconstruction: A
descriptive study in a preliminary cohort. J Oral Maxillofac Surg 67:
2559-2570.
18.
Markiewicz
MR, Dierks EJ, Potter BE, Bell RB (2011) Reliability of intraoperative
navigation in restoring normal orbital dimensions. J Oral Maxillofac Surg 69:
2833-2840.
19.
Bruneau
M, Schoovaerts F, Kamouni R, Dache S, De Witte O, et al. (2013) The mirroring
technique: A navigation-based method for reconstructing a symmetrical orbit and
cranial vault. Neurosurgery 73: 24-28.
20.
Eckardt
AM, Lemound J, Rana M, Gellrich NC (2013) Orbital lymphoma: Diagnostic approach
and treatment outcome. World J Surg Oncol 11: 73.
21.
Hejazi
N (2006) Frameless image-guided neuronavigation in orbital surgery: Practical
applications. Neurosurg Rev 29: 118-122.
22.
Sieskiewic
A, Lyson T, Mariak Z, Rogowski M (2008) Endoscopic trans-nasal approach for
biopsy of orbital tumours. Acta Neurochir (Wien) 150: 441-445.
23.
Gazioglu
N, Abuzayed B, Tanriover N (2011) Neuronavigation-guided endoscopic endonasal
excision of an intraorbital intraconal cavernous hemangioma. J Craniofac Surg
22: 1802-1805.
24.
Gao D,
Fei Z, Jiang X, Zhang X, Liu W, et al. (2012) The microsurgical treatment of
cranio-orbital tumors assisted by intraoperative electrophysiologic monitoring
and neuronavigation. Clin Neurol Neurosurg 114: 891-896.
25.
Hejazi
N (2006) Intra orbital lymphomas: Neurosurgical experiences and management
strategies. J Neurosurg Rev 29: 123-129.
26.
Sacchetti
M, Macchi I, Tiezzi A, La Cava M, Massaro-Giordano G, et al. (2016)
Pathophysiology of corneal dystrophies: From cellular genetic alteration to
clinical findings. J Cell Physiol 231: 261-269.
27.
Cooke
DL, Levitt M, Kim LJ, Hallam DK, Ghodke B (2010) Intra orbital access using
fluoroscopic flat panel detector CT navigation and three-dimensional MRI
overlay. J Neurointerv Surg 2: 249-251.
28.
Nesbit
GM, Nesbit EG, Hamilton BE (2011) Integrated cone-beam CT and fluoroscopic
navigation in treatment of head and neck vascular malformations and tumors. J
Neurointerv Surg 3: 186-190.
29.
Reinbacher
KE, Pau M, Wallner J, Zemann W, Klein A, et al. (2014) Minimal invasive biopsy
of intraconal expansion by PET/CT/MRI image-guided navigation: A new method. J
Craniomaxillofac Surg 42: 1184-1189.
30.
Walter
U, Niendorf T, Graessl A, Rieger J, Krüger PC, et al. (2014) Ultrahigh field
magnetic resonance and colour Doppler real-time fusion imaging of the orbita
hybrid tool for assessment of choroidal melanoma. Eur Radiol 24: 1112-1117.
31.
Lauretti
L, D'Alessandris QG, Rigante M, Ricciardi L, Mattogno PP, et al. (2018) O-arm
in endonasal endoscopic cranial base surgery: Technical note on initial
feasibility. World Neurosurg 117: 103-108.
-
 Table 1
Table 1 -
Table 2
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Dermatology Clinics and Research (ISSN:2380-5609)
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- International Journal of Anaesthesia and Research (ISSN:2641-399X)
- Oncology Clinics and Research (ISSN: 2643-055X)
- Journal of Renal Transplantation Science (ISSN:2640-0847)
- International Journal of Clinical Case Studies and Reports (ISSN:2641-5771)
- International Journal of Surgery and Invasive Procedures (ISSN:2640-0820)


