940
Views & Citations10
Likes & Shares
Keywords: Hypoglossal
nerve palsy, Neurinoma, MRI.
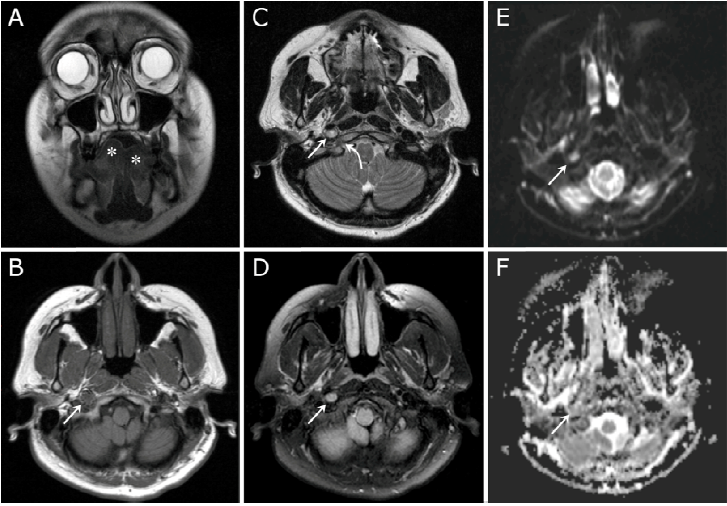
A 33-year-old female presented with deviation of her tongue towards the right side (Figure 1, A). Magnetic resonance imaging (MRI) of the head revealed a 1.0 x 0.8cm mass abutting the right internal carotid artery in close proximity to the hypoglossal canal. The mass proved relatively isointense to brain parenchyma on T1 weighted images (Figure 1, B), slightly hyperintense on T2 weighted images (Figure 1, C), with a higher signal intensity on T2-tirm imaging (Figure 1, D). A “T2 shine through” phenomenon was also noted on Diffusion Weighted Imaging (DWI) with Apparent Diffusion Coefficient (ADC) mapping (Figure 1, E and F), the findings being consistent with a hypoglossal neurinoma (schwannoma) of the carotid space segment.
The hypoglossal nerve is divided into five
segments: the medullary, cisternal, skull base, carotid space, and sublingual
segments. Because each segment is usually affected by different disorders,
localizing a lesion to a particular segment allows the physician to narrow the
differential diagnosis [1]. Cranial nerve schwannomas are usually isolated
lesions, except when they are associated with neurofibromatosis type 2
(abnormality of chromosome 22) [2]. Because of the substantial chance of nerve
palsy following resection, obtaining an accurate preoperative diagnosis with
the identification of the involved structures is crucial to the management
strategy [3]. MRI is the investigation of choice in the diagnosis of schwannoma
and the identification of the nerve of origin [3]. Evolving MRI techniques such as super selective diffusion tensor
tractography (DTT) can provide further details related to the tumor and cranial
nerve interface, including the presence or absence of penetrating fibers [4].
1. Thompson EO, Smoker WR.
Hypoglossal nerve palsy: a segmental approach. Radiographics. 1994;14(5):939-958.
2. Spilberg G, Marchiori E,
Gasparetto EL, Cabral RF, Takayassu TC, Batista RR, Vieira IG. Magnetic
resonance findings of neurofibromatosis type 2: a case report. Cases J.
2009;2:6720
3. Liu HL, Yu SY, Li GK, Wei WI.
Extracranial head and neck Schwannomas: a study of the nerve of origin. Eur Arch Otorhinolaryngol. 2011;268(9):1343-1347.
4. Wei PH,
Qi ZG, Chen G, Hu P, Li MC, Liang JT, Guo HC, Ling F, Bao YH. Identification of
cranial nerves near large vestibular schwannomas using superselective diffusion
tensor tractography: experience with 23 cases. Acta Neurochir (Wien). 2015;157(7):1239-1249.
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Chemotherapy Research Journal (ISSN:2642-0236)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- International Journal of Diabetes (ISSN: 2644-3031)
- Journal of Pathology and Toxicology Research
")
")



