879
Views & Citations10
Likes & Shares
Objective: To investigate surface lustrous, morphological, and compositional changes of retrieved orthodontic mini-screw implants (MSIs) and to asses potential metal ion release.
Materials and methods: Ten orthodontic mini-screw implants (Tomas-Pin SD, Dentaurum, Ispringen, Germany) placed in 5 female orthodontic patients (16.11 ± 1.68 years) to serve as anchorage for maxillary canine retraction. The MSIs were retrieved after successful service for 4 months. Digital microscope, scanning electron microscope and X-ray fluorescence spectrometer were used for analysis of surface gloss, morphology, and composition of MSIs, respectively before and after usage. At regular scheduled visits the following were recorded: unstimualated salivary pH; levels of titanium, aluminum and vanadium ions in unstimulated saliva.
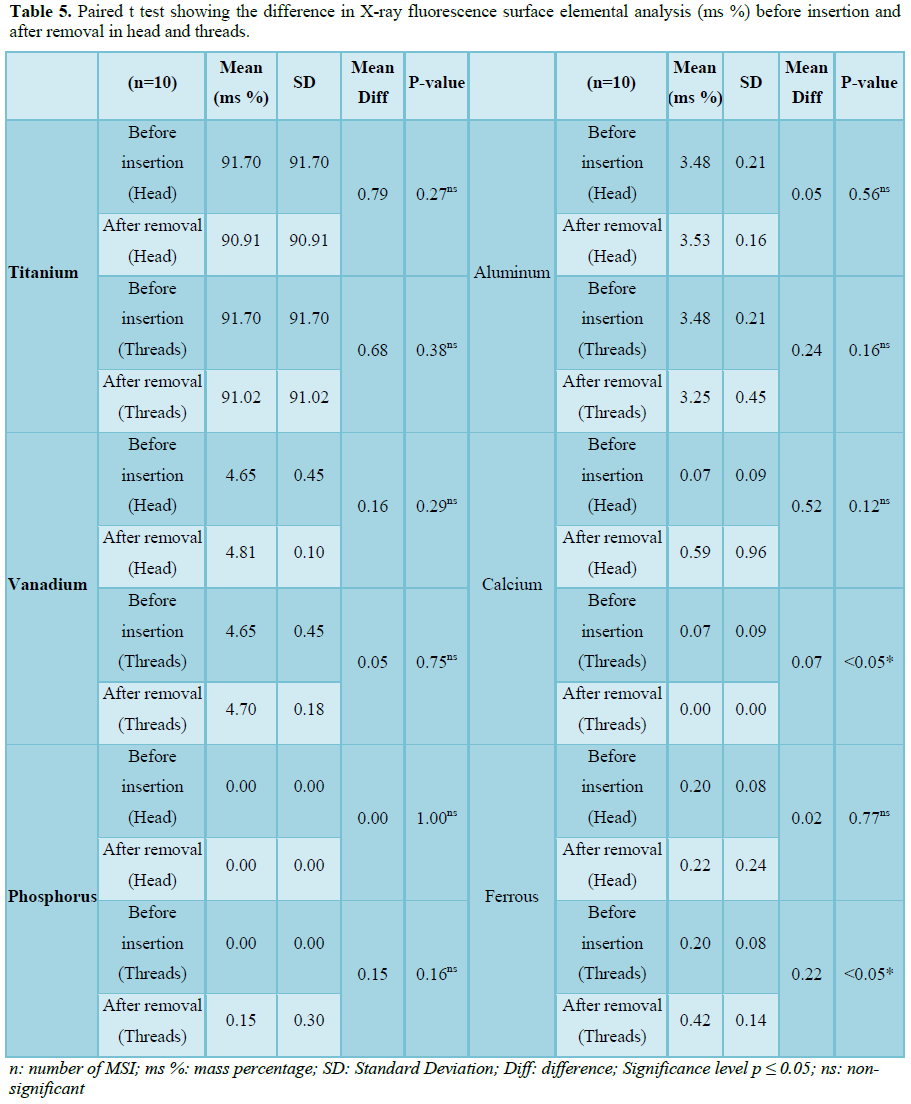
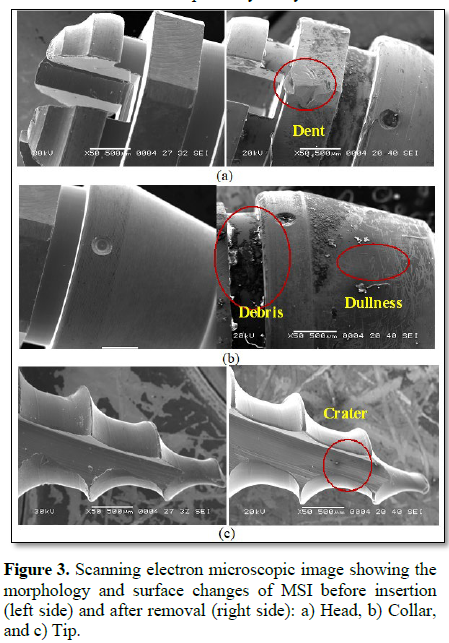
Results: Surface elemental analysis showed significant calcium mass % increase in the head portion and significant ferrous mass % increase in the thread portion of MSIs. Scanning electron microscope examination of MSIs displayed surface changes in the form of dullness, dents of threads and tips, and to less extent corrosion, craters.
Conclusion: The head portion of all MSIs showed degradation after clinical use characterized by loss of the original color and gloss. The surface analysis of retrieved MSIs differed from that of as-received MSIs, with additional elements; the most noticeable were calcium and phosphorus (contact with saliva and oral fluid) in the head portion and iron in the thread portion (contact with blood and tissue fluid) of MSI (P<0.05). Salivary contents of Ti, Al, V did not increase after insertion of MSIs.
Keywords: Canine retraction, Mini-screw implants, Metal release, Surface analysis
INTRODUCTION
Clinical studies have suggested that mini-screw implants (MSIs) may provide stable anchorage during the orthodontic treatment without requiring patient cooperation. These studies proved many successful applications in orthodontics involving; retraction of anterior teeth, correction of open bites, distalization, mesialization and intrusion of teeth [1-5].
Various materials were used in implant systems. The implant material must be nontoxic, biocompatible, mechanically sufficient, and having high tension and corrosion resistance. Commercially pure titanium (cp Ti) was the most used material in prosthetic implants because of its; high biocompatibility, high corrosion resistance in body fluids, not allergic, high specific strength and low elastic modulus when compared with other metallic biomaterials [1,4-7].
On the other hand, orthodontic MSIs are smaller than conventional prosthetic implants and should resist high orthodontic loads. These factors contribute to the possible fracture of cp Ti MSIs during placement, use and removal. To avoid such fracture, Ti alloy implants were composed through the addition of aluminum (6Al) and vanadium (4V), (Ti-6Al-4V), for adding strength and fatigue resistance than cp Ti [4,7,8]. Unfortunately, this alloy has a low corrosion resistance and can result in corrosion of the orthodontic MSIs in body fluids [9,10].
Saliva, oral fluids, chemicals introduced into the oral cavity through food and drink, the enzymatic behavior, microbial activity, pH fluctuation, temperature fluctuation and host - mini-screw implant interaction could present a brutal condition for the titanium alloy giving rise to potential surface corrosion and metal ion release [9,10]. So, the study was conducted to investigate the effects of clinical usage on surface lustrous, morphological, and compositional characteristics of retrieved orthodontic MSIs. Also, to investigate metal ions (titanium, aluminium and vanadium) released in saliva after insertion of MSIs.
SUBJECTS AND METHODS
The sample was consisted of 10 orthodontic mini-screw implants (MSIs) placed in 5 female orthodontic patients between 14 and 18 years (16.11 ± 1.68 years). Mini-screw implants were installed to serve as anchorage for maxillary canine retraction after maxillary first premolar extraction. Patients consented to participate in the study which ran for 4 months. Ethical approval was obtained from the regional committee for medical and health research ethics, faculty of Medicine (boys), Al-Azhar University, Cairo, Egypt. The study was registered in clinical trials.gov identified by the following number (NCT03460132).
Sample size calculation was based on power of statistics analysis, using the standard deviation in previous studies [11-13]. The estimated sample size for a one-sample proportion test (score z-test) was calculated to be 6 orthodontic mini-screw implants.
The inclusion criteria: 1) patients indicated for bilateral extraction of maxillary first premolar, 2) Good oral and general health (Free of any disease that could affect oral conditions), and 3) All teeth should be free from caries or any metallic restorations.
Patients with history of occupational exposure to metals, seriously fractured appliance, deteriorated oral hygiene condition, and/or broken appointment that affect the progress of treatment or study protocol were excluded.
For each patient, non-metallic fixed orthodontic appliance consisted of: 1) direct bond, pre-adjusted Roth ceramic brackets (0.022" × 0.028"), 2) teflon-coated nickel titanium round arch wires (0.012", 0.014", 0.016", 0.018") for the leveling and alignment stage and teflon-coated stainless steel arch wires (0.018" or 0.016" × 0.022") for the canine retraction, 3) the arch wires were ligated by clear latex-free elastic O-ties, 4) Self-drilling (SD) orthodontic MSI (Tomas-Pin SD, Dentaurum, Ispringen, Germany) (1.6 mm in diameter, 8 mm in thread length, gingival collar (2.8 mm maximum diameter, 2 mm in height) and a head with cross slot 2.25 mm in height) was used as an anchorage for maxillary canine retraction [4].
An insertion guide was used to standardize the receptor site between maxillary first molar and second premolar. The wire was inserted into the first molar bracket with a coil at the other end of the wire to locate accurately the vertical (6-8 mm from the bracket slot apically) and anterio-posterior (center of inter-dental bone) position of the MSI. The MSI was directed perpendicular to the buccal alveolar bone surface.
Canine retraction was started simultaneously in both sides, immediately after MSIs installation, by extending elastomeric chain (clear, short) between the head of the MSIs and the maxillary canine hooks [14]. Activation was done every three weeks (the elastic chain replaced by a new one) to have standardized force all over the experimental period. The initial force should be in the range of 200-250 g to obtain the standardized canine retraction force (approximately 150 g) after the first day sharp decay of force [15].
All MSIs were removed either after four months of the experimental period and/or complete retraction of one of the canines into the extraction space by the application of counter clockwise torque load with the screwdriver supplied from the manufacturer [14]. Each MSI was placed in sterile glass rubber-seal top test tube containing 1 ml of saline solution for cleaning using vortex vibrator. After removal of MSIs, the orthodontic treatment was continued according to the proposed line of treatment for each patient.
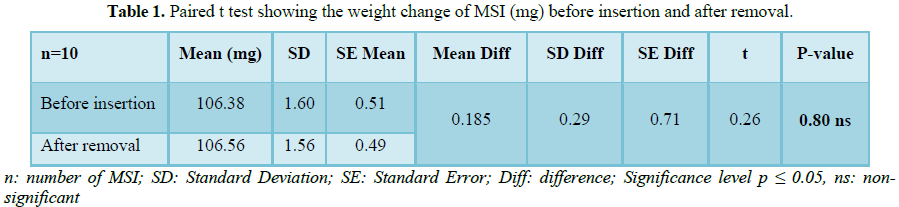
Weight changes were measured using an electronic sensitive balance by weighting each MSI before placement and after removal. Each measurement was recorded twice and the average weight to the nearest ± 0.01 mg was used as the result [16].
Saliva samples were collected immediately before MSIs insertion, one week, one month, three months and four months after MSIs insertion to measure salivary potential of hydrogen (pH) and to analyze the amount of metal ions (titanium, aluminium and vanadium) released from the MSIs.
The sample was collected in the morning after usual breakfast and tooth brushing. The patients rinsed her mouth thoroughly with 100 ml distilled water for 1 min, expectorate and then wait for a while until saliva accumulated in her mouth. Approximately 4 ml of non-stimulated saliva was collected in a sterile, glass rubber seal-top test tube, then coded and stored at -20°C in a freezer [16,17].
Microcomputer based pH/temperature bench meter (Model 6173/6173R, JENCO Electronics, Shanghi, China) was used for analysis of salivary pH. Each measurement was recorded twice and the average pH value to the nearest ± 0.01 was used as the result [16-18].
Inductively coupled plasma optical emission spectroscopy (ICP-OES) (Prodigy High Dispersion ICP, Leeman, USA) was used to determine the initial salivary concentration of titanium, aluminium and vanadium and the concentration of these metal ions drained into the salivary solution after MSIs insertion [6,7,17-19].
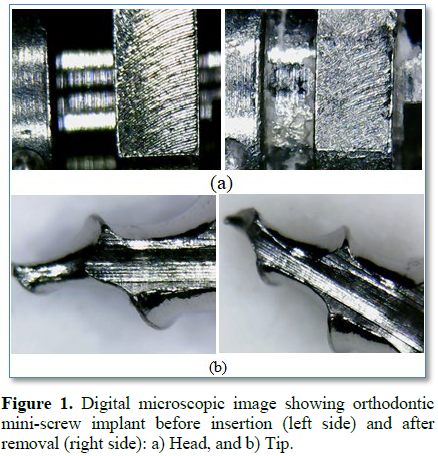
Surface color changes were evaluated by imaging MSIs before and after placement using digital microscope (DM-UM012A-1.3m USB Digital Microscope with 8 LED Lights, Guangdong, China). The images (Figure 1) were imported into image processing software (Image J, National Institute of Health NIH, USA) which detect the luminance or lightness component, ranging from (0 to 100). At least 10 points in each part of MSI (head, thread and tip) were analyzed and the average was taken as the result [11,20].
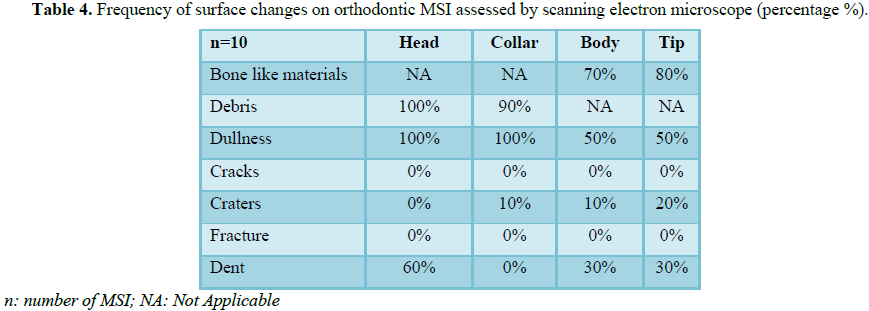
Scanning electron microscope (JEOL-JSM 5600 LV) was used for scanning MSI surfaces before and after insertion for the detection and imaging (magnification=50x) of surface roughness, craters and integument adhered to any part of MSIs (Figure 2). Operating parameters for ICP-OES: (1.2 kW) RF power, (19 L/min) coolant Flow, (34 psi Concentric) nebulizer Pressure, (0.7 l/min Argon) purge gas flow, (0.8L/m) auxiliary flow [11,21].
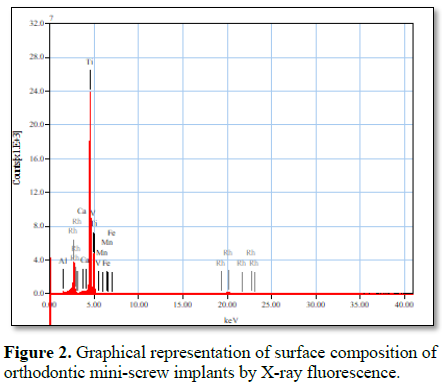
The surface’s qualitative elemental microanalysis (Figure 3) of each MSI was determined before and after usage with X-ray fluorescence spectrometer (XRF) (JEOL, JSX-3222 analyzer) [11,22].
STATISTICAL ANALYSIS
The collected data was tabulated and statistically analyzed using S.P.S.S. (SPSS 18(2009); SPSS Inc., Chicago, IL, USA). The data was analyzed using t-test and ANOVA test followed by Tukey’s post hoc test when ANOVA revealed a significant difference (p ≤ 0.05).
RESULTS
The weight of MSI (mg) was increased after removal (Table 1). The mean difference was (0.185 mg). Paired t-test revealed that the difference was statistically insignificant (p=0.80).
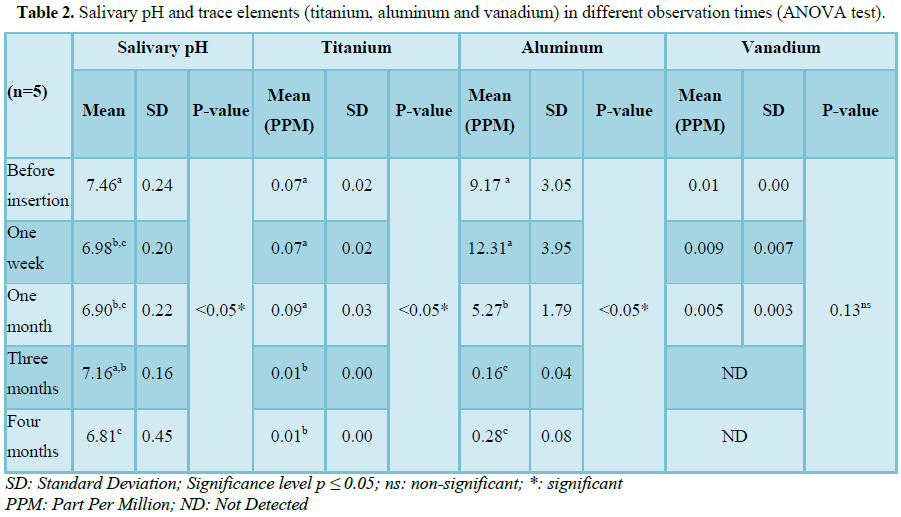
ANOVA test revealed that the difference in pH level (Table 2) was statistically significant (p<0.05*). The mean salivary pH before insertion of MSIs was 7.46 which become more acidic after one week 6.98, one month 6.90 and four months 6.81.
Tukey’s post hoc test: means sharing the same superscript letter were not significantly different
Salivary titanium concentration increased at 1 month and then significantly decreased at 3 months and after removal. ANOVA test revealed that the difference in salivary (Ti) concentration was statistically significant (P<0.05*). Tukey’s post hoc test revealed statistically insignificant increase in salivary titanium concentration at one month and statistically significant decrease after three, four months of MSIs insertion.
Salivary aluminium concentration (Table 2) increased at 1 week, then significantly decreased at 1 month, then further decreased at 3 months and after removal. ANOVA test revealed that the difference in salivary (Al) concentration was statistically significant (P<0.05*). Tukey’s post hoc test revealed statistically insignificant increase in salivary aluminium concentration at one week and statistically significant decrease after one, three and four months of MSIs insertion.
Salivary vanadium concentrations (Table 3) were gradually decreased at 1 week, 1 month and were not detectable thereafter. ANOVA test revealed that the difference in salivary (V) concentration was statistically insignificant (p=0.13).
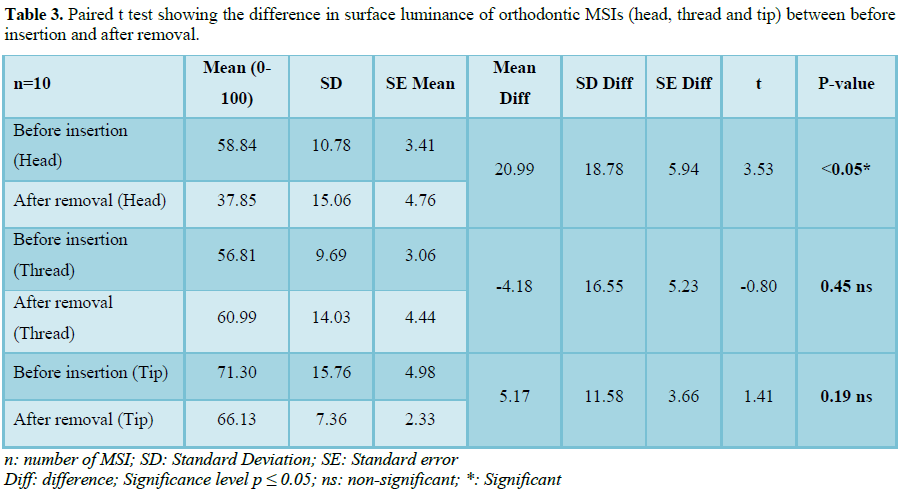
The difference in surface luminance or lightening (indicator of surface finish and gloss) between before insertion of MSIs and after removal in three different parts of MSIs (head, threads and tip) had been shown in Table 4. The table showing statistically significant difference in the luminance of the head of MSIs (P<0.05*) and non-significant difference in the thread (p=0.45) and tip (p=0.19) of MSIs.
Surface elemental composition analysis of MSIs (X-ray fluorescence spectrometer) revealed insignificant increase (paired t-test) in calcium ms % in head portion and phosphorus ms % in thread portion of MSIs (Table 5). Paired t test also revealed statistically significant increase in ferrous ms % on the thread portion of MSIs.
DISCUSSION
The weight gain of orthodontic MSI after four months of clinical use could be attributed to the accumulation of food debris on the head of MSIs and foreign body adherence on the threads of MSIs. To our knowledge after searching the scientific literature, no data were available for evidence about the weight changes of orthodontic mini-screw implants after usage.
Saliva has a dynamic structure that could be affected by many physiologic variables. Temperature, quantity and quality of saliva, salivary pH, plaque and amount of protein in saliva, physical and chemical properties of food and liquids and general and oral health conditions were factors that could influence orthodontic MSI corrosion in the oral cavity [19].
In an effort to report these concerns, in the current study, the saliva was collected from the same patients who did not have any health problems or any caries in the mouth and good oral hygiene. All the samples were taken in the morning before breakfast and the patients rinsed their mouths thoroughly with distilled water before the collection. Salivary pH was measured for each patient before insertion of MSIs, one week, one month, three months and four months of MSIs insertion in order to analyze a reported factor that could increase corrosion of titanium alloy MSIs. Although the changes in salivary pH were statistically significant, it was considered within the neutral pH condition [3].
Metal ions released were analyzed using inductively coupled plasma optical emission spectrophotometry (ICP-OES) which was a common, documented and very sensitive method used for trace element analysis in the literature. [19,23].
The clinical usage of orthodontic mini-screw implants appeared to do not significantly affect the salivary concentrations of titanium, aluminium and vanadium. These were assured by the insignificant increase in the salivary concentrations of titanium and aluminium after one week of MSI insertion. The decrease in salivary concentrations of titanium, aluminium and vanadium could be attributed to the precipitation of calcium/phosphorus minerals from the body fluid into the titanium surface, which decreases the ion release [24].
Retrieved MSIs presented loss of gloss and surface finish, resulting in a dull surface in head portion of all 4 examined zones. It was assumed that insertion and removal of MSIs causes the surface to wear out to some extent. Blunting of threads and tip (less sharp thread and tip compared with as-received screws) was also linked to wear during the process of insertion and removal [11,25,26].
Titanium alloys used to manufacture MSIs were less resistant to corrosion because the alloys represent discontinuities in the protective oxide film [25]. The surface milling and polishing defects during the manufacturing process were seen in the form of stripes and scratches.
These tiny defects can be a starting point for electrochemical attack when mini-screws were inserted in the body [27]. Although titanium alloys have been considered highly corrosion resistant because of the stable passive titanium oxide layer on the surface, they were not inert to corrosive attack. When the stable surface oxide layer broken down or removed and cannot reform on parts of the surface, titanium can be corrosive, as many other base metals [28].
The current study revealed statistically insignificant difference in the main component of orthodontic mini-screw implants (titanium, aluminium and vanadium), statistically insignificant increase in the amount of calcium in the thread portion of MSI and statistically significant increase ferrous ms % in the head of MSI. These results indicate substantial changes in the surface profile of mini-screw implants including adsorption of a calcified integument from the contact of the material with saliva, food, blood, biological fluids and tissue fluids. The presence of iron and calcium derives from the contact of implant surface with blood and agrees with research on biomedical materials including cardiac valves and orthopedic prostheses [11,25].
CONCLUSION
1) Despite the statistically significant decrease in salivary pH, it was considered within the neutral pH.
2) Salivary contents of Ti, Al, V did not increased after insertion of MSIs.
3) The head portion of all MSIs showed degradation after clinical use characterized by loss of the original color and gloss.
4) Scanning electron microscope examination of MSIs displayed surface changes in the form of dullness, dents of threads and tips and to less extent corrosion, craters.
5) The surface elemental composition of retrieved MSIs differed from that of as-received MSIs, with additional elements; the most noticeable were calcium (contact with saliva and oral fluid) in the head region, iron and phosphorus in the thread region (contact with blood and tissue fluid) of MSI (P<0.05).
1. Ricardo CB, Roberta TB (2015) In vitro study of human osteoblast proliferation and morphology on orthodontic mini-implants. Angle Orthod 85: 920-926.
2. Zhang L, Zhao Z, Li Y, Wu J, Zheng L, et al. (2010) Osseo-integration of orthodontic micro-screws after immediate and early loading. Angle Orthod 80: 354-360.
3. Galeotti A, Uomo A, Spagnuolo G, Paduano S, Cimino R, et al. (2013) Effect of pH on in vitro biocompatibility of orthodontic mini-screw implants. Prog Orthod 14: 1-7.
4. Huang LH, Shotwell JL, Wang HL (2005) Dental implants for orthodontic anchorage. Am J Orthod Dentofacial Orthop 127: 713-722.
5. Jasoria G, Shamim W, Rathore S, Kalra A, Manchanda M, et al. (2013) Mini-screw implants as temporary anchorage devices in orthodontics: A comprehensive review. J Contemp Dent Pract 14: 993-999.
6. Morais LS, Serra GG, Palermo EFA, Andrade LR, Muller CA, et al. (2009) Systemic levels of metallic ions released from orthodontic mini-implants. Am J Orthod Dentofacial Orthop 135: 522-529.
7. Safiya S, Manjunath G (2013) Mini-implant materials: An overview. J Dent Med Sci 7: 15-20.
8. Kosayadiloka K, Tangjit N, Luppanapornlarp S, Santiwong P (2017) Metal ion release and cytotoxicity of titanium orthodontic mini-screws. Key Eng Mater 730: 141-147.
9. Mikulewicz M, Chojnacka K (2011) Release of metal ions from orthodontic appliances by in vitro studies: A systematic literature review. Biol Trace Elem Res 139: 241-256.
10. Blaya MG, Blaya CS, Mello P, Flores EMM, Hirakata LM (2011) Titanium alloy mini-screws for orthodontic anchorage: An in vivo study of metal ion release. Rev Odonto Cienc 26: 209-214.
11. Eliades T, Zinelis S, Papadopoulos MA, Eliades G (2009) Characterization of retrieved orthodontic mini-screw implants. Am J Orthod Dentofacial Orthop 135: 10.e1-7.
12. Martín-Cameán A, Puerto M, Jos Á, Azqueta A, Iglesias-Linares A, et al. (2015) Preliminary study of genotoxicity evaluation of orthodontic mini-screws on mucosa oral cells by the alkaline comet assay. Toxicol Mech Methods 25: 487-493.
13. Patwari M (2013) Cytotoxicity of orthodontic temporary anchorage devices in vitro. Proquest Dissertations and Thesis 197: 1-60.
14. Jasoria G, Shamim W, Rathore S, Kalra A, Manchanda M, et al. (2013) Mini-screw implants as temporary anchorage devices in orthodontics: A comprehensive review. J Contemp Dent Pract 14: 993-999.
15. Ravi K, Balasubramaniam MR, George M, Duraisamy S (2010) Comparison of canine retraction using slide friction less ligature modules with conventional modules - An in vivo study. J Dent Sci 1: 150-155.
16. Kader HM, Aref MI, Hussein FA (2008) Coating failure of commercial orthodontic magnets and DNA fragmentation of oral mucosa cells. Aust Orthod J 24: 32-40.
17. Kumar RV, Rajvikram N, Rajakumar P, Saravanan R, Deepak VA, et al. (2016) An accurate methodology to detect leaching of nickel and chromium ions in the initial phase of orthodontic treatment: An in vivo study. J Contemp Dent Pract 17: 205-210.
18. Lara-Carrillo E, Montiel-Bastida NM, Sánchez-Pérez L, Alanís-Tavira J (2010) Effect of orthodontic treatment on saliva, plaque and the levels of Streptococcus mutans and Lactobacillus. Med Oral Patol Oral Cir Bucal 15: e924-929.
19. Mikulewicz M, Wołowiec P, Loster B, Chojnacka K (2015) Metal ions released from fixed orthodontic appliance affect hair mineral content. Biol Trace Elem Res 163: 11-18.
20. Leo´n K, Mery D, Pedreschi F, Leo´n J (2006) Color measurment in L* a * b* units from RGB digital images. Food Res Int 39: 1084-1091.
21. Burmann PFP, Ruschel HC, Vargas IA, Verney JCK, Kramer PF (2015) Titanium alloy orthodontic mini-implants: Scanning electron microscopic and metallographic analyses. Acta Odontol Latinoam 28: 42-47.
22. Muguruma T, Iijima M, Brantley WA, Yuasa T, Ohno H, et al. (2011) Relationship between the metallurgical structure of experimental titanium mini-screw implants and their torsional properties. Eur J Orthod 33: 293-297.
23. Peitsch T, Klocke A, Kahl-Nieke B, Prymak O, Epple M (2007) The release of nickel from orthodontic NiTi wires is increased by dynamic mechanical loading but not constrained by surface nitridation. J Biomed Mater Res 82A: 731-739.
24. El-wassefy NA, El-Fallal AA, Taha M (2015) Effect of different sterilization modes on the surface morphology, ion release and bone reaction of retrieved micro-implants. Angle Orthod 85: 39-47.
25. Patil P, Kharbanda OP, Duggal R, Das TK, Kalyanasundaram D (2015) Surface deterioration and elemental composition of retrieved orthodontic mini-screws. Am J Orthod Dentofacial Orthop 147: S88-100.
26. Mattos CT, de Oliveira Ruellas AC, Elias CN (2010) Is it possible to re-use mini-implants for orthodontic anchorage? Results of an in vitro study. Mater Res 13: 521-525.
27. Sebbar M, Bourzgui F, Aazzab B, Elquars F (2011) Anchorage mini-screws: A surface characterization study using optical microscopy. Int Orthod 9: 325-338.
28. Abey S, Mathew MT, Lee DJ, Knoernschild KL, Wimmer MA, et al. (2014) Electrochemical behavior of titanium in artificial saliva: Influence of pH. J Oral Implantol 40: 3-10.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Cardiology and Diagnostics Research (ISSN:2639-4634)
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- Oncology Clinics and Research (ISSN: 2643-055X)
- Journal of Renal Transplantation Science (ISSN:2640-0847)
- International Journal of AIDS (ISSN: 2644-3023)
- Journal of Cell Signaling & Damage-Associated Molecular Patterns
- Journal of Spine Diseases


