1287
Views & Citations287
Likes & Shares
Background: Recurrent aphthous stomatitis (RAS) is one
of the most common oral mucosal conditions. Most of the currently available
treatment modalities aim at symptomatic relief hasten healing and prevent
recurrence of ulcers. The aim of the study is to compare the efficacy of Aloe vera gel with 5% Amlexanox oral
paste in the treatment of minor RAS.
Materials and methods: 64 patients diagnosed to have
minor recurrent aphthous ulcers were randomly divided into Group A (Aloe vera gel group -32) and Group B
(Amlexanox oral paste group - 32). The base line parameters were recorded on
day of first visit which included ulcer size, pain and erythema. Evaluation of
reduction in ulcer size, pain and erythema were made on day 3 and day 7. The
recurrence rate of ulcer was evaluated for 6 months at monthly intervals.
Results: In both group A and group B, marked
improvement was observed in ulcer size, pain and erythema between baseline and
day 3, baseline and day 7 and day 3 and day 7. Both the groups were found to be
effective in reducing ulcer size, pain and erythema but Aloe vera gel group when compared with Amlexanox group has
significant reduction in ulcer size and VAS score (P=<0.001).
Conclusion: Aloe
vera proved to have multiple unique properties with very less side effects.
Aloe vera gel group when compared
with Amlexanox group has significant reduction in ulcer size and VAS score
hence proving to be clinically beneficial in treatment of minor RAS.
Keywords: RAS, Aloe vera, Amlexanox, Efficacy
INTRODUCTION
Recurrent
aphthous stomatitis (RAS) is a disorder characterized by recurring ulcers
confined to the oral mucosa in patients with no other signs of disease and can
cause pain on eating, swallowing and speaking [1,2]. The pathophysiology of
aphthous ulcers is poorly understood [3-5]. The diagnosis is primarily based on
the history and clinical criteria [5]. RAS can be clinically classified mainly
into three groups: Minor aphthae, major aphthae and recurrent herpetiform
ulcers [3,4]. Various treatment modalities of RAS include systemic therapies,
topical agents, physical therapies, laser therapy, etc. Topical agents are the
first choice of management for RAS. They are cost effective, safe and easily
available. Amlexanox (C16H14N2O4)
is one of the most extensively studied topical agents available for the
treatment of RAS. It has an anti-inflammatory, anti- allergic action which
inhibits the formation and release of histamine and leukotriene’s from mast
cells, neutrophils and mononuclear cells [4]. Aloe vera (AV- Aloe
barbadensis Miller) is one amongst the natural herbal medicine which is
used as an alternative therapy for RAS. The transparent gel derived from Aloe vera leaves contains a series of
natural components which has immunomodulators, anti-inflammatory, wound
healing, antioxidant, anti-diabetic and anti-neoplastic properties. These
properties lead the researchers to use it in management of minor RAS [6]. Since
Aloe vera is one of a novel modality
with its efficacy and rate of recurrence still under investigations, very few
studies were observed during literature search. Hence the present study is
designed to compare the efficacy of Aloe
vera gel with 5% Amlexanox oral paste in the treatment of minor RAS.
MATERIALS AND METHOD
The study
was conducted on 64 patients with minor RAS who visited our Department of Oral
Medicine and Radiology. The patients were selected according to the specific
inclusion and exclusion criteria. The following criteria were utilized to
select the patients with minor RAS: age range 18 to 50 years, presenting with
single or multiple minor RAS of less than 48 h duration, location of ulcer must
be easily accessible. Exclusion criteria comprised of pregnancy and lactation,
history of allergies to Aloe vera and
Amlexanox, patients on NSAIDs, immune modulatory agents or systemic
antibiotics, patients on any other oral topical medication, with bleeding
disorders and on corticosteroid therapy, ulcers as manifestation of systemic
diseases. The whole study process was explained to the patients before and
informed consent was obtained. The ethical clearance was obtained from
institutional ethical board. The clinical trial registry – India registration
number for this trial is CTRI/2018/05/013778. The proforma was distributed
among the study subjects, which included demographic data, medical history and
study parameters.
The patients
were distributed as Group A (Aloe vera
gel – Forever company, Bangalore, India) or Group B (5% Amlexanox oral paste -
Lexanox oral paste, Macleods pharmaceuticals limited, Mumbai- India) through
lottery method of randomization. Group A patients were instructed to apply Aloe vera gel directly on the ulcer 3
times a day for 10 days (after meals and before bed time) and Group B patients
were instructed to apply 5% Amlexanox oral paste on the ulcer 4 times a day for
10 days (after meals and before bed time). The base line parameters were taken
and recorded on the day of the first visit. Reduction in ulcer size, pain (VAS
score) and erythema were evaluated on day 3 and day 7 and recurrence rate of
the ulcer were evaluated for 6 months at monthly intervals. Subjects were
instructed that if any allergic reactions occur they should terminate usage of
medication and inform the investigator immediately. To determine the size of
the ulcers, a calibrated William‘s periodontal probe with millimetre markings
was used to measure the ulcer size at the maximum diameter of the ulcer. Degree
of erythema was evaluated on a 4 point scale ranging from 0 to 3 based on the
methods of Greer et al. [7]. Evaluation of recurrence in both the groups was
done by monthly follow ups either by clinical examination or by telephonic
follow up (for those who could not come for follow up appointment).
STATISTICAL ANALYSIS
Both the
study group and the control group will be compared with respect to all the
baseline parameters. The mean differences in the lesion diameter and
inflammation diameter between the two groups will be compared at baseline, on
day 3, day 7 and at 1 month follow up periods using Independent sample t-test.
The mean decline in the lesion diameter and increase in inflammation diameter
at different follow up periods, differences along with their 95% CI and p value
will be presented. P value<0.05 will be considered statistically
significant. IBM SPSS statistical software, version 21 will be used for
statistical analysis.
RESULTS
A total of 64 patients (32 in Group A and 32
in Group B) who were diagnosed with minor recurrent aphthous ulcers were
enrolled in this study. There were 2 dropouts from both Group A and Group B. At
the end of the study period we had 30 patients each in Group A and Group B. All
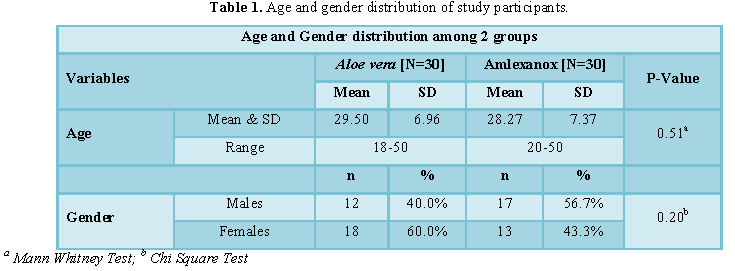
the findings were subjected for statistical analysis. The gender distribution
in the study sample of 60 patients, 12 (40.0%) being males and 18 (60.0%) being
females in Aloe vera group and 17 (56.7%)
being males and 13 (43.3%) being females in Amlexanox group, respectively (Table 1). The age range of patients in
Aloe vera group was 18-50 years and
the age range of patients in Amlexanox group was 20-50 years.
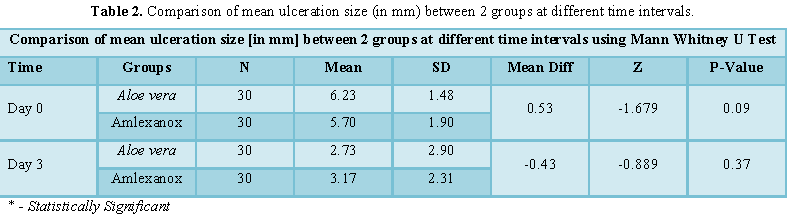
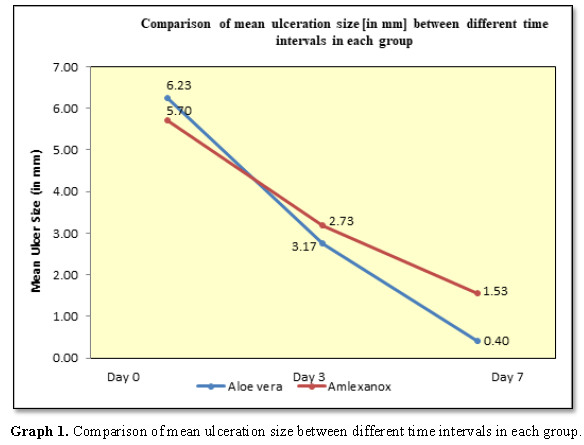
The mean ulcer size at baseline for the
patients of group A was 6.23 ± 1.48 and that of group B was 5.70 ± 1.90. After
using Aloe vera gel patients were
recalled on the day 3 and day 7. The results revealed significant reduction of
ulcer size in both Group A and Group B on day 3 (2.73 ± 2.90 and 3.17 ± 2.31,
respectively) and day 7 (0.40 ± 0.97 and 1.53 ± 1.72), respectively.
Statistically significant difference between Group A and Group B was observed
in day 7 (P=0.001) (Table 2).
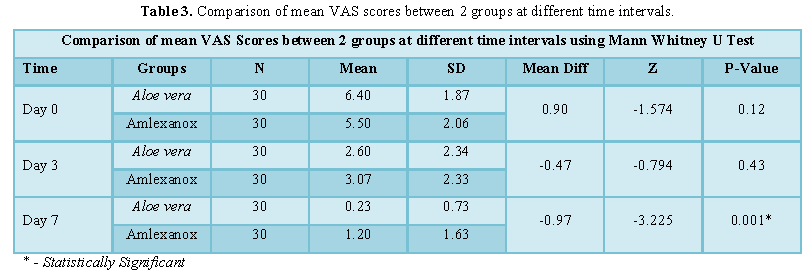
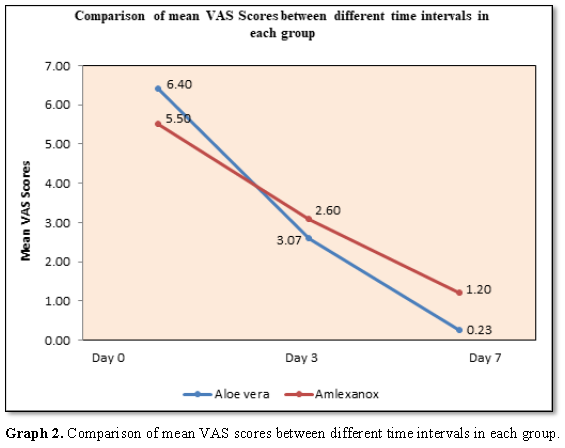
The mean pain score at baseline for the
patients of Group A was 6.40 ± 1.87 and that of Group B was 5.50 ± 2.06. A
marked reduction in pain in both Group A and Group B was noted on day 3 (2.60 ±
2.34 and 3.07 ± 2.33) and day 7(0.23 ± 0.73 and 1.20 ± 1.63), respectively.
Statistically significant difference between Group and Group B was observed in
day 7 (P=0.001) (Table 3).
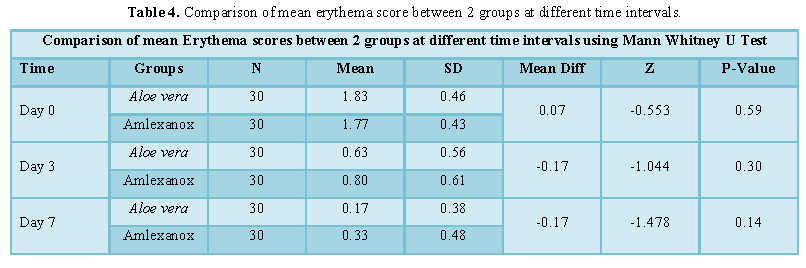
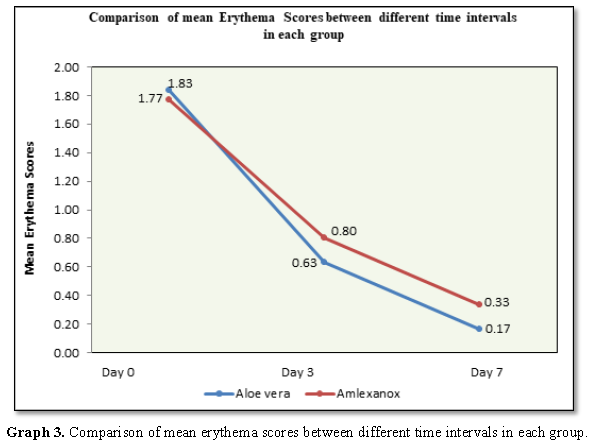
The mean erythema score at baseline for Group
A was 1.83 ± 0.46 and that of Group B was 1.77 ± 0.43. A slight reduction in
erythema in both Group A and Group B was noted on day 3 (0.63 ± 0.56 and 0.80 ±
0.61 and day 7(0.17 ± 0.38 and 0.33 ± 0.48), respectively. No statistically
significant difference was observed in day 3 and day 7 in erythema reduction
between Group A and Group B (Table 4).
On comparison of mean ulceration size ,VAS
scores and erythema scores between different time intervals in each group
signifies that within group A statistically significant difference were
observed between baseline and day 3 (P value=<0.001), baseline and day 7
(P=<0.001)) and day 3 and day 7 (P=<0.001) and within Group B
statistically significant difference were observed between baseline and day 3
(P value=<0.001), baseline and day 7 (P=<0.001) and day 3 and day 7
(P=<0.001) (Graphs 1-3).
DISCUSSION
The primary goals of therapy for RAS are
relief of pain, reduction of ulcer size and duration and the restoration of
normal oral function. Secondary goals include reduction in the frequency and
severity of recurrence and maintenance of remission [8]. A wide range of
treatments ranging from topical agents to systemic medications, physical
modalities, natural remedies, home remedies and homeopathic remedies have been
tried in the treatment of RAS [9]. The present study aimed at evaluating the
efficacy of Aloe vera gel with 5%
Amlexanox oral paste in reducing the size, pain and erythema of minor RAS. In
our study, female predominance was noted in both the groups which accounts for
51.65%. This is in accordance with Rajmane et al. study where majority of
patients were females. Females are more prone to stress and emotional
situations which can affect their immune response. They seek medical examination
more frequently than males. The hormonal changes during pregnancy and
menstruation also play a role [10]. Maximum number of patients belonged to
21-30 years of age group which correlated with the study done by Kareem et al.
in which about 80% of patients develop the condition before 30 years of age.
The highest incidence is among young people, however the severity and frequency
of ulcers decreases with age [11]. A high prevalence and severity of the
disease has been found in students with a high socio-economic background. This
is because psychological stress acts as a triggering factor for RAS and is
typically observed during stressful situations such as school exam and any
other significant changes in life [12]. This is in accordance with Abdullah et al
study where majority of patients were students [13].
The ulcer size in both Group A and Group B
showed marked improvement between the baseline and day 3, baseline and day 7
and day 3 and day 7. This is in accordance with Babaee et al. study where Aloe vera gels were found to be
effective in reducing ulcer size [14]. There was significant difference between
Aloe vera gel and Amlexanox oral
paste in reducing the size of the ulcer in day 7 (P=0.001, respectively).
According to literature, Glucomannan, a mannose-rich polysaccharide and
gibberellin, a growth hormone, interacts with growth factor receptors on the
fibroblast, thereby stimulating its activity and proliferation, which in turn
significantly increases collagen synthesis after topical application of Aloe vera [15].
Both Group A and Group B had marked reduction
in VAS scores between baseline and day 3, baseline and day 7 and day 3 and day
7. However on comparing both groups, Aloe
vera gel showed a significant difference in pain reduction in day 7 (P=0.001,
respectively).This indicates that Aloe
vera gel has a significant therapeutic effect in reducing the VAS score
which is in accordance with the Babaee et al. study where Aloe vera gel were found to be effective in alleviating ulcer pain
[16]. According to literature, Aloe vera
inhibits the cyclooxygenase pathway and reduces prostaglandin E2 production
from arachidonic acid. Recently, the novel anti-inflammatory compound called
C-glucosyl chromone was isolated from gel extracts which helps in relieving pain
[15].
In our study we have observed obvious
improvement in erythema associated with RAS in both the study groups between
baseline and day 3, baseline and day 7 and day 3 and day 7 but there was no
statistically significant difference between the groups in any of the follow up
visits (P=0.59, P=0.30, P=0.14, respectively). Amlexanox due to its
anti-inflammatory property is equally effective as Aloe vera in reducing the erythema. This in accordance with the
study done by Katti et al. [16]. During the study period, periodic phone calls
were made to the participants to confirm the use of the interventions. Aloe vera gel and Amlexanox oral paste
were well tolerated by the patients during the study period without any major
side effects.
CONCLUSION
The results of the study suggests that both
treatment groups were found to be effective in healing of ulcers, reducing the
pain and erythema. Aloe vera gel group when compared with Amlexanox
group has significant reduction in ulcer size and VAS score hence proving to be
clinically beneficial in treatment of minor RAS. However, studies on a larger
series of patients for a longer duration may be required in order to determine
the true therapeutic effects of Aloe Vera and to compare their efficacy in the
management and recurrence of minor RAS.
1. Preeti L, Magesh KT, Rajkumar K,
Karthik R (2011) Recurrent aphthous stomatitis. J Oral Maxillofac Pathol 15:
252-256.
2. Scully C, Gorsky M, Lozada-nur F
(2003) The diagnosis and management of recurrent aphthous stomatitis: A
consensus approach. JADA 134: 200-207.
3. Vivek V, Nair BJ (2011) Recurrent
aphthous stomatitis: Current concepts in diagnosis and management. J Indian
Acad Oral Med Radiol 23: 232-236.
4. Boras VV, Savage NW (2007)
Recurrent aphthous ulcerative disease: Presentation and management. Aust Dent J
52: 10-15.
5. Porter SR, Hegarty A, Kaliakatsou
F, Hodgson TA, Scully C (2000) Recurrent aphthous stomatitis. Clin Dermatol 18:
569-578.
6. Vogler BK, Ernst E (1999) Aloe
vera: A systematic review of its clinical effectiveness. Br J Gen Pract 49:
823-828.
7. Mansour G, Ouda S, Shaker A,
Abdallah HM (2014) Clinical efficacy of new Aloe
vera and myrrh‐based oral mucoadhesive gels in the management of minor
recurrent aphthous stomatitis: A randomized, double‐blind, vehicle‐controlled
study. J Oral Pathol Med 43: 405-409.
8. Aljbab AA, Almuhaiza M, Patil SR,
Alanezi K (2015) Management of recurrent aphthous ulcers: An update. Int J Dent
Oral Health 20: 2.
9. Akintoye SO, Greenberg MS. (2014)
Recurrent aphthous stomatitis. Dent Clin N Am 58: 281-297.
10. Patil S, Reddy SN, Maheshwari S,
Khandelwal S, Shruthi D, et al. (2014) Prevalence of recurrent aphthous
ulceration in the Indian Population. J Clin Exp Dent 6: e36.
11. A-kareem SAL, Ahmed KM (2015)
Prevalence of Aphthous ulceration in patients attending oral diagnosis clinics
at School of Dentistry/University of Sulaimani for four academic years
(2010-2014). IOSR J Dent Med Sci (IOSR-JDMS) 14: 80-84.
12. Byahatti SM (2013) Incidence of
recurrent apthous ulcers in a group of student population in Libya: A
questionnaire study. Arch Cran Oro Fac Sc 1: 26-30.
13. Abdullah MJ (2013) Prevalence of
recurrent aphthous ulceration experience in patients attending Piramird Dental
Specialty in Sulaimani City. J Clin Exp Dent 52: e89.
14. Babaee N, Zabihi E, Mohseni S,
Moghadamnia AA (2012) Evaluation of the therapeutic effects of Aloe vera gel on minor recurrent
aphthous stomatitis. Dent Res J 9: 381-385.
15. Renu T, Jyoti G, Sheikh A,
Rajneesh P (2012) Aloe vera and its
uses in dentistry. Indian J Dent Adv 4: 652-658.
16.
Meng
W, Dong Y, Liu J (2009) A clinical evaluation of amlexanox oral adhesive
pellicles in the treatment of recurrent aphthous stomatitis and comparison with
amlexanox oral tablets: A randomized, placebo controlled, blinded, multicenter
clinical trial. Trials 10: 30.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Allergy Research (ISSN:2642-326X)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Advance Research on Alzheimers and Parkinsons Disease



