1014
Views & Citations14
Likes & Shares
The
associations between positive mood and impulsiveness in the deaf and
hard-of-hearing individuals have not received much attention. The aim of this
paper was to study this association in a group of deaf and hard-of-hearing
polyclinic patients at a University Hospital in Sweden (n=52) that were
compared to healthy individuals (n=116). The Positive and Negative Affect
Scale, Life Orientation Test, Barratt’s Impulsiveness Scale, Locus of Control,
Situational Intrinsic Motivational Scale and a Background & Health
Questionnaire were used. The results indicated that the patient group expressed
less optimism, greater external Locus of Control, identified regulation,
external regulation, amotivation, distractiveness, and motor impulsiveness than
the healthy controls. The patients expressed also a lower level of positive
mood than the healthy controls. Regression analysis indicated that for the
patient group positive mood was predicted by optimism and motor impulsiveness
whereas amotivation and distractiveness were counterpredictive. For the control
group positive mood was predicted by optimism and counterpredicted by
identified regulation and distractiveness. This pattern of results suggests
that this group of patients seek to emerge from a condition of disempowerment
but require suitable interventional therapies to succeed.
Abbreviations: ADHD: Attention Deficit Hyperactivity
Disorder, BIS: Barratt’s Impulsiveness Scale, DSM: Diagnostic and Statistical
Manual of Mental Disorders, ICD: International Classification of Mental and
Behavioral Disorders, LOC: Locus of Control, LOT: Life Orientation Test,
MANOVA: Multivariate Analysis Of Variance, NA: Negative Affect, PA: Positive
Affect, PANAS: Positive Affect and Negative Affect Scale, SIMS: Situational
Intrinsic Motivational Scale, SSL: Swedish Sign Language
Keywords: Positive mood, Affective deaf syndrome, Deaf
and hard-of-hearing, Psychiatric diagnoses, Impulsiveness, Motivation,
Disempowerment
INTRODUCTION
Structured assessment of positive mood and mental distress in deaf and hard-of-hearing individuals is difficult for various reasons. The combination of the complex interaction of affective psychiatric disorders and low level of self-rated positive mood in psychiatric patients with communication problems due to deafness/hard-of-hearing has been termed the Affective Deaf Syndrome (ADS) [1]. At the core of deafness/hard-of-hearing lies a communication problem with the hearing community. This handicap may be important for the development of the clinical psychiatric profile of individuals with deafness/hard-of-hearing as well as the affective mood. There are some indications that self-esteem may predict positive affect for this patient group and may be identified as a protective factor [1].
Also, these patients seem to have more self-rated stress, more use of analgesics and less self-rated energy than healthy hearing volunteers. Although ADS is not yet fully understood, there are several distinguishing features, including disrupted attachment to parents, feelings of abandonment and over-protectedness. Traumatic upbringing for many individuals in this category may contribute to the syndrome. Studies of positive and negative affect may offer a key to understanding ADS.
Positive mood is a concept that depends on both positive affect (PA) as well as negative affect (NA) and is defined as (PA/NA)*100. There have been different views as to the understanding of the continuum of positive and negative affect. Garcia [2] concluded after a thorough review of the literature that positive and negative affect are best thought of as two independent dimensions of the affective system. Both PA and NA may possess explanatory value despite these scales being correlated with different factors [3]. The two dimensions are also measures of anxiety and depression – anxiety is a state of high NA whereas depression is a mixed state of high NA and low PA [4]. It has been found repeatedly that PA expresses enthusiasm, activity, control and feelings of duty, associated with a positive attitude, both over time and varying circumstance [5,6], whereas NA reflects expressions of affect, such as anger, contempt, guilt, shame, fear and depressiveness that appear to present relatively stable personality characteristics [7-9]. Negative affect has been demonstrated to predict stress, which in turn has predicted general and situational depressiveness [10].
The intrinsic-extrinsic motivation dichotomy displayed by individuals has been a matter of much investigation [11], whereby intrinsic motivation pertains to be the performance of an activity itself whereas extrinsic motivation pertains to a multitude of activities whose goals extend beyond the activity itself [12,13]. Situational motivation is that experienced by individuals within ongoing activities and/or occupations and has been examined extensively through applications of the Situational Intrinsic Motivational Scale (SIMS), a self-report measure that has been validated by [14]. Self-determination theory posits that different types of motivation underlie human behavior and on a continuum of high-low self-determinism intrinsic motivation, extrinsic motivation and amotivation are so ordered [15]. The regulation of behavior by rewards or attempts to avoid negative consequences is referred to as external regulation whereas behavior valued and perceived as chosen by an individual himself/herself is referred to as identified regulation. This latter form of motivation may still be extrinsic as the behavior is not performed for itself, exclusively, but may rather be as the means to an end [14]. SIMS has been shown to equate the operationalization of motivation with conceptual definitions that tackle the perceived reasoning that underlies task engagement [16,17].
Impulsivity has been defined as “a predisposition toward rapid, unplanned reactions to internal or external stimuli with diminished regard to the negative consequences of these reactions to the impulsive individual or others” [18, 19]. Recent research on the relationship of impulsivity to psychiatric disorders has been based on the DSM-IV diagnostic criteria [20]. Although impulsivity is directly mentioned in the DSM-IV diagnostic criteria for several disorders and is implied in the criteria for others there has according to [18] until recently been little work on clarifying the role of impulsivity in psychiatric illness. One of the problems in studies on psychiatric patients is that although some examples of impulsive behavior are given in the DSM-IV, impulsivity is not explicitly defined. In the study by Moeller et al. [18] the overall goal of the article was to provide a definition of impulsivity that can be used to bridge the gap between clinical work and research. They also aimed at discuss the relationship between impulsivity and several psychiatric disorders.
Several disorders, in which immediate gratification is given a higher priority than long-term goals in decision-making, are characterized by high levels of impulsiveness and poor decisions, in for example, attention deficit hyperactivity disorder (ADHD), bulimia nervosa and substance-abuse disorders e.g. [21].
A study at the Psychological Institution at University of Gothenburg and Sahlgrenska University Hospital on affective profile included psychiatrically ill patients who at the inclusion in the study fulfilled the psychiatric diagnostic criteria (DSM IV-R and ICD-10 [22]) for major depressive disorder 54%, anxiety disorder 37% and a mixed group 9% including bulimia nervosa, polymorph psychosis and ADHD. At the time of the gathering of the data the patients were in a neutral mood. Eighty-three % of the patients also fulfilled the criteria for personality disorder with mainly borderline diagnoses according to DIP-Q [23]. In a study of deaf and hard-of hearing patients [1] depressive disorder was less, 43%, and anxiety disorder almost the same 33%, but ADHD was higher 21,4 %. The great difference was that in the study of deaf and hard of hearing patients we found that only 12 % fulfilled the criteria of personality disorder compared to the results of the earlier study which had 83%. Both studies indicated that patients with a psychiatric diagnosis differ from healthy controls with regard to PA, NA, depression, compulsion, anxiety and personality traits (DIP-Q) even when they did not exhibit clinical symptoms of their disorder.
The interrelationship between chronic physical illness, depression or depressive symptoms has been associated with individuals’ cognitive-emotional behavioral profiles that are linked to sets of psychosocial resources determining health outcomes [24,25]. Since depression is characterized by low levels of self-esteem, low levels and/or unstable self-esteem may offer an enduring vulnerability factor for depression [26].
Psychiatric patients with psychiatric illness and a disability with deafness or hard-of hearing have also been studied. Early reports indicate [27] that among deaf psychiatric ill persons as much as 50% of the precipitant causes of the patients revolved around early traumatic physical injuries, operations, or fear of separation from significant relationships in what they termed “traumatic injury”. The study noted that 21 % of patients displayed disturbed behavior. In a more recent study [28] a broader range of diagnoses was found than in past studies with posttraumatic stress disorder being the most common diagnosis. Compared with hearing patients, the deaf patients were less likely to be diagnosed with a psychotic or substance abuse or disorder and more likely to be diagnosed with a mood, anxiety, personality, or developmental disorder. An important finding [28] was that 75% of deaf individuals fell into the non-fluent range of communication in American Sign Language. Mood disorders and substance abuse were diagnosed infrequently in past research and traumata and their squeal have earlier hardly been addressed at all [29]. One reason for this situation may be that diagnosis assessments may not have been performed by psychiatrists assigned to the patients at a Deaf Unit, but by psychiatrists in general wards not specialized on deaf persons.
AIM OF THE STUDY
The aim of this study was to investigate the differences between attributes associated with positive mood and attributes showing an association in deaf/hard-of-hearing patients with psychiatric disorders. We expect these observations to contribute to the clinical treatment of patients affected with the affective deaf syndrome.
MATERIALS AND METHODS
Psychiatric patients with severe hearing impairment and deafness were recruited from the University Hospital in Gothenburg. Data were collected during a 12-month period from August 2014 until August 2015. The group consisted of 52 patients, 10 men and 42 women with a mean age of 42.63 years (SD = 12.74; range = 21-71). The diagnostic assessments were performed by a psychiatrist assigned to the Deaf Unit. The specialist team consisted of a psychiatric consultant, a psychologist, an occupational therapist, a social counselor and a specialist nurse and it has many years of established expertise in clinical treatment of deaf people. The team worked with interpreters using the Swedish Sign Language (SSL). All patients completed the questionnaire themselves and explanations of the questions were available in the SSL for those who needed that information. Only patients who were able to understand the questions were included, thus 10 % with severe mental retardation were not included in the study. Except for two patients all were willing to take part in the study. The patients were in their habitual psychiatric state with neutral mood and no clinical symptoms of depression, anxiety or psychosis. All had undergone psychiatric and/or psychological treatment before the study.
A healthy control group was recruited from the same socio-economic area as the patients. The healthy volunteers were not paid for their participation. The group had to sign an agreement of participation and that they had received information that they could stop the participation of the study at any moment. The number of healthy controls were 116 participants, 41 men and 75 women with a mean age of 46.13 years (SD = 13.57; range = 19-75). Each participant was asked to complete a battery of psychometric test instruments as well as a Background and Health Questionnaire.
The ethics protocol of Sahlgrenska University Hospital was applied and maintained for patients and healthy controls. The agreement included total anonymity of results for both groups. The patients were in their habitual psychiatric state. Most had been treated by medication and psychotherapy for some period before the study. Their hearing loss ranged from very severe to total loss of hearing. The SSL was used when needed and was offered by trained translators who also outside the study helped the same patients with interpretation.
A Background and Health Questionnaire including age, gender, partnership, number of children and age of children, years of education after the obligatory nine-year education, smoking and drinking habits, pain, sleeping problems, physical exercise, television hours/day, percentage of sedentary work, self-evaluation of general health, use of mood-enhancing drugs and analgesics, length, weight and waist measurement were completed according to the description and procedure outlined in [30].
Positive Affect and Negative Affect Scale (PANAS).The instrument [7] provides a self-estimation of affect, both positive and negative. It consists of 10 adjectives for the Negative Affect (NA) dimension (Negative affect: Cronbach’s α = .83) and 10 adjectives for the Positive Affect (PA) dimension (Positive affect: Cronbach’s α = .88). The test manual [7, 8] postulates that the adjectives describe feelings (Affect) and mood level. Participants were instructed to estimate how they felt during the last few days. The response alternatives were presented on a five-grade scale that extended from where 1= not at all to 5= very much. The negatively-charged adjectives were summated to provide the NA score and the positively-charged adjectives were summated to a PA score. The PANAS-instrument has been validated through studies analyzing conditions associated with general aspects of psychopathology [31]as well as a multitude of other expressions of affect [32]. The PANAS in our study showed high reliability in the whole sample (Chronbach’s α .88 for both PA and NA). Positive mood defined as (Positive affect/Negative affect)*100 = .88 (Chronbach’s α.)
Life orientation Test (LOT). This instrument measures individual’s degree of dispositional optimism. The instrument is based on a general model, regarding self-regulated behavior, which indicates that optimism exerts meaningful behavioral consequences based on the model [33]. It was constructed originally to study the extent to which personality trait optimism was associated with the ability to develop suitable ‘coping strategies’ in connection with severe psychological and physical handicaps (e.g., tinnitus). The instrument consists of 12 statements and the response alternatives are presented on a five-graded scale extending from 0 = “strongly disagree” to 4 = “strongly agree”. LOT is a suitable scientific instrument with an estimated internal consistency off .76 (Chronbach’s α) and a test-retest reliability of .79 (Pearson’s r), indicating that the test result is stable over time [33]. The LOT test requires about 5 minutes for completions. When this instrument was used in this study the internal consistency was found to be .76 (Chronbach’s α).
Barratt’s Impulsiveness Scale (BIS-11, modified and translated).BIS is a questionnaire released in 1995 to assess the personality/behavioral construct of impulsiveness [34]. This scale uses the word impulsiveness rather than the more general term impulsivity. It is the most widely cited instrument for the assessment of impulsiveness that has been used to advance our understanding of this construct and its relationship to other clinical phenomena for 50 years [35].Participants respond to statements on a 4-point scale. “Rarely/Never” – “Occasionally” –“Often” –“Almost Always/Always”, whereby 16 out of the 25 items express impulsiveness such as “I do things without consideration”, or “I act impulsively, and, conversely, 9 out of 16 items express non-impulsiveness, such as “I have good self-control”, or “I plan for the future”. Nine of the twenty-five items are scored formulated to express ‘non-impulsiveness’ there by providing a reverse order, avoiding response bias, and sixteen items provided direct scores of impulsiveness. The items were, according to [34], divided into three factors: Distractiveness (originally called Attentional impulsiveness) with Chronbach’s α = .72 (8 items); Non-planning impulsiveness with a Chronbach’s α = .72 (8 items); and Motor impulsiveness, comprising 9 items (Chronbach’s α = .67).According to the factor analysis study [36], BIS items may be chosen to produce three factors, inability to plan, lack of self-control and sensation/novelty seeking that are tangential to the three subscales, non-planning, motor and cognitive impulsiveness. BIS has been translated into several different languages with test-retest reliability ranging from .71 – .89[37,38].The Barratt Impulsiveness Scale 11 – has three 2nd order factors these are: distractiveness, motor impulsiveness and non planning impulsiveness each is also divided into two 1st order factors. In our study we found distractiveness α = .41 the two 1st order factors attention α = 0.16 and cognitive instability α = .55. The second order motor impulsiveness α = .60 is divided into 1st order of motor α = .55 and perseverance consisting of only one variable. The second order non planning impulsiveness α = .60 is divided into self-control with α = .56 and cognitive complexity consisting of only two variables. The reliability of the whole questionnaire without the subdivisions into the 2nd and 1st order factors is α = .57.
Locus of Control (LOC).Locus of Control was measured using a modified version [39], using an abbreviated version of the Rotter scale [40], and developed [41], for use mainly in Swedish work settings. The scale has a minimum score of 8 and a maximum of 40, with a lower score representing an external locus of control orientation and a higher score representing an internal locus of control orientation. Several empirical studies have shown that perceived control is strongly work-related with rehabilitation outcomes, not lest empowerment [42,43]. Possible considerations pertaining to cross- confounding with other constructs appear to have been rebutted by Lefcourt [44]. In the current study the score was reversed for four of the 8 items (on a 5-point scale) was to enable recalculation to represent External locus of control (Chronbach’s α = .70).
Situational Intrinsic Motivational Scale (SIMS). The SIMS instrument provides an estimation of the constructs (factors), intrinsic motivation, identified regulation, external regulation and amotivation [15] in both field and laboratory settings. It was have shown [14] that SIMS is composed of four internally consistent values (Chronbach’s α) for each factor, showing: intrinsic motivation = .95, identified regulation = .80, external regulation= .86 and amotivation = .88, with self-report internal consistency scales in the .70 - .80 range acceptable for research purposes. The construct validity of SIMS has been shown to be supported by correlations with other constructs, e.g., perceived competence, concentration and behavioral intentions. The present version of SIMS included four items for each factor, e.g., intrinsic motivation: “Because I think this activity is interesting”, identified regulation: “Because I am doing it for my own good”, external regulation: “Because I am supposed to do it”, and amotivation: “there may be good reasons to do this activity, but personally I don’t see any”. The statements have seven response alternatives [1=not at all, 2= very little, 3= a little, 4=moderately, 5=enough, 6=a lot, 7=exactly] that provided the eigen values of 5.70, 2.63, 1.33, and .73, for each factor respectively. It was shown [14] both that perceived competence, concentration and behavioral intentions of future persistence toward the activity were associated with SIMS factors according to the self-determination continuum and specific and positive interrelations between Academic Motivation Scale factors [45] and the SIMS factors. The internal consistency (Chronbach’s α) in our study for the four factors were: intrinsic motivation= .87, identified regulation=.81, external regulation = .82, and amotivation= .74.
Statistical Analyses
Data were analyzed using SPSS version 20 software. Pillai’s Multivariate Analysis of Variance (MANOVA) was applied with type of group as independent variables and with dispositional optimism, external locus of control, internal locus of control, motor impulsiveness, identified regulation, external regulation, amotivation, distractiveness, motor impulsiveness, non-planning impulsiveness and positive mood as dependent variables. We analyzed our data with MANOVA instead of multiple ANOVAS because the MANOVA also determines the interactions taking place amongst the dependent variables [46]. One-way ANOVA was performed to analyze the mean differences between the patient group and the healthy volunteers’ group. A linear regression analysis was performed to examine to which extent positive mood may be predicted from the dependent variables.
RESULTS
Psychiatric diagnostic system used was (DSM-IV and ICD-10). The patients fulfilled the criterion for the following psychiatric conditions at the inclusion into the study, but were treated by medication and/or psychotherapy before they participated in answering the questionnaires. At that time they did not exhibit symptoms of depression, anxiety or psychosis: Depressive disorders (F32 and F33; DSM 296) = 43%, Anxiety disorders F 41, DSM 300) = 33%, Trauma- and Stressor-Related disorders (F43; DSM 308, DSM 309) = 33%, Attention-Deficit/Hyperactivity disorder (F90; DSM 314) = 21,4 %, Obsession-Compulsive disorder (F42; DSM 300.3) = 12 %, Schizotypal Personality disorder (F21, F22; DSM 301, DSM 297) = 7%, Personality disorder Cluster B = 5%, Substance-Related and Addictive disorders (F10; DSM 303) = 5%. Forty-two % of the patients fulfilled more than one diagnosis. Most common was the combination of Depressive disorder combined with Anxiety disorder and/or Trauma-and Stressor-Related disorders. Type of deafness: deaf = 63,5 %, and hard-of-hearing = 36,5%. Etiology of deafness: unknown = 38,0%, hereditary = 30,9%, Rubella = 16,7%, meningitis = 2,4%, prematurity = 2,4%, infection = 4,8% and other = 4,8 %. Hearing status of parents: none deaf parent = 85,7%, one deaf 4,8 = % and two deaf parents = 9,5 %. Hearing status of siblings and relatives: one deaf = 4,8 % and more than one deaf = 21,4 %. Family communications: Speech, writing, and gesture = 73,8 %, some sign = 11,9 % and fluent sign = 14,3%.
The patients mean for PA was 3.08 (SD = .76) and the controls M = 3.41 (SD = .52). The patients mean for NA was 2.55 (SD = .86) and the controls M = 1.79 (SD = .59).
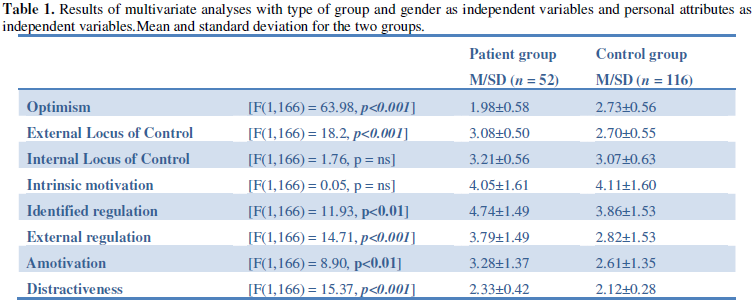
Pillai’s multivariate analysis of variance (MANOVA) (2x2 factorial design) was applied with type of group (patients and healthy controls) and gender as independent variables and optimism, locus of control (extern and intern), intrinsic motivation, identified regulation, external regulation amotivation, distractiveness, non-planning impulsiveness, motor impulsiveness, and positive mood as dependent. The results indicated a significant effect for group F (10, 158) = 9.61; p<.001, Eta2 = 0.41, power = 1.00), but no significant group effect was found for gender (p = .29). The analysis did not indicate any significant interaction for group and gender (p = .38). With positive mood as independent variable in a one-way ANOVA, significant effects demonstrating differences in vulnerability between individuals in the patient group and the healthy volunteers’ group were found. Patients expressed significantly more external locus of control, identified regulation, external regulation, amotivation, distractiveness and motor impulsiveness. Controls were found to have significantly higher optimism and positive mood. There were no significant differences between the groups for internal locus of control, intrinsic motivation, and non-planning impulsiveness (see Table 1).
Regression Analysis
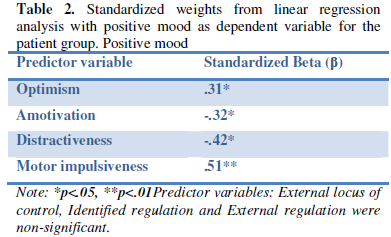
Results from the patient group is shown in table 2. In order to assess the extent to which positive mood may predict the result outcome pertaining to the variables estimated in optimism, external locus of control, identified regulation, external regulation, amotivation, distractiveness and motor impulsiveness, a regression analysis was performed with each of the former as independent variables and positive mood as dependent variable. Regression analyses indicated that positive mood (F (7, 44) = 5.141, p<.001, adj. R2=.36) was predicted by optimism and motor impulsiveness, and was counter predicted by amotivation and distractiveness.
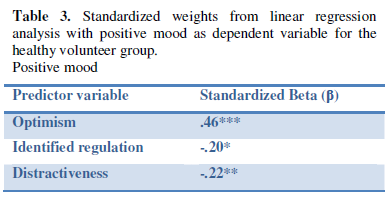
For results from healthy volunteers see table 3. In order to assess the extent to which positive mood may predict the result outcome to the variables estimated in the independent variables, regression analyses were performed with positive mood as dependent variable. The analyses indicated that positive mood (F (7, 107) = 11.06, p<.001, adj. R2=.38) was predicted by optimism and was counter predicted by identified regulation and distractiveness.
The aim of this study was to investigate the differences between attributes associated presenting positive mood and attributes showing an association in deaf/hard-of-hearing patients with psychiatric disorders. The variables that define the patient group are less optimism, a greater external control, a higher identified regulation, higher amotivation, higher external regulation, more distractiveness, higher motor impulsiveness and a lower positive mood.
The present findings implicate markedly the predictive associations in the patient group between positive mood with optimism, lack of motivation (i.e., amotivation), distractiveness and motor impulsiveness. Impulsiveness total is according to [30] predicated by NA. In clinical samples [35] motor impulsiveness has been related to episodes of mania, but also to ADHD. Stanford also demonstrated that attentional impulsiveness(distractiveness) is related to both episodes of mania and depression and that non-planning has been related to unipolar depression and ADHD.
The results of our study demonstrate a significant difference between the groups where distractiveness and motor impulsiveness both are significantly higher than in the patient group. Non-planning, however, does not indicate a significant difference, but is relatively high in both groups. It is an interesting fact that our study concludes that positive mood is predicted by motor impulsiveness in the patient group, but not in the control group. Motor impulsiveness is strongly associated with positive mood in the patient group, but not in the control group. Is it the case that the patient group experience that motor impulsiveness has a positive value through the induction of a higher positive mood?
The results also show that the deaf and hard-of-hearing patients have less disadvantageous positive mood than patients with anorexia [47] and/or hearing psychiatric patients [23].The patients mean for PA was 3.08 (SD = .76) and the controls M = 3.41 (SD = .52), which is somewhat higher for the patients but not for the controls reported from a study on psychiatrically ill patients with normal hearing [48] with the values M = 2.43 (SD .86) and the controls M = 3.57 (SD .91). A study on patients with anorexia nervosa [47] on the other hand reported lower PA, M = 2.81(SD = .82) for the patients but slightly higher value for the healthy age-matched controls, M = 3.63 (SD = .71). The patients mean for NA was 2.55 (SD = .86) and the controls M = 1.79 (SD = .59), which is slightly lower both for the patients in the study on psychiatrically ill patients with normal hearing M = 2.79 (SD = 1.00) but slightly lower for the controls M = 1.92 (SD .81). NA in our study was lower than the results for patients with anorexia nervosa M = 3.14 (SD = .74) and our controls had a lower NA than the healthy controls for the anorexia nervosa group M = 2.08 (SD = .62). It seems logical that the clinically most ill group the anorexia patients had the lowest PA and highest NA and that the least ill group the deaf and hard-of-hearing patients had the highest PA and the lowest NA. However, it is the triad of the ADS with clinically adverse symptoms that is problematic for the deaf/hard-of -hearing patient group. It is the combination of affective disorders including depressive disorders 43%, anxiety disorders 33%, ADHD 21%, OCD 12% and personality disorders 12% and the high intake of analgesics, low self-esteem, amotivation, low optimism together with problems of communication that together add to the burden of distress of the deaf and hard-or-hearing patient group.
CONCLUSION
The results contribute towards an understanding of some aspects of the
complex ADS syndrome. Although the psychiatrically ill deaf and hard-of-hearing
patients expressed less severe loss of positive mood compared to patients with
anorexia nervosa and a group of hearing psychiatric patients they were worse
affected than other groups due to the complex ADS syndrome that besides
psychiatric disorders and mood disorder includes a handicap of communication.
Impulsiveness seems to be associated with positive mood in the patient group.
Nevertheless, we do not have enough data to explain the role of impulsiveness
in the dynamic of positive mood of the deaf and hard-of-hearing patient group.
Suffice it to say, the pattern of personal attributes reported by the present
group of deaf and hard-of-hearing patients implies that an element of
disempowerment constrains their behavioral repertoire; interventions that place
a premium upon the acquisition of personal empowerment ought to be sought as
offering a high degree of benefit.
LIMITATIONS
The particular condition
of this patient-group implies that the number of individuals available for
participation was limited. Nevertheless, the present findings seem robust. The aim of the study was to study
deaf and hard-of-hearing psychiatrically ill patients in order to understand if
and how these individuals may
differ from healthy individuals. The purpose
therefore was to look for weaknesses and strong sides of the
profile of the patients and healthy individuals and use the results clinically
as indications to which resources may
be missing in the ADS group and could then
be trained to benefit the health of this group. A second control group would
have been a strength, but we did not find deaf and hard-of-hearing volunteers
without psychiatric disorders who were willing to undergo a psychiatric
examination to establish their psychiatric health and then volunteer to answer
the questionnaires. Thus, this limitation
remains to be considered in a future study.
ACKNOWLEDGEMENTS
Psychologists
Johannes Einestam and Vera Lundborg, specialist nurse Anette Ohlson,
occupational therapist Pernilla Malmros and social counselor Eva Lundholm
helped in collecting the data often in cooperation with sign interpreters.
1. Zöller MET,
Archer T (2015) Emotional
disturbances Expressed by Deaf Patients: Affective Deaf Syndrome. Clin Exp
Psychol 2: 109.
2. Garcia D (2011) Adolescents’
happiness: The role of the affective temperament model on memory and
apprehension of events, subjective well-being, and psychological well-being
Doctoral thesis). University of Gothenburg, Sweden.
3. Clark A, Watson LA (1988) Mood and
the mundane: relations between daily life events and self-reported mood. J Pers
Soc Psychol 54: 296-308.
4. Clark LA, Watson D (1991)
Tripartite model of anxiety and depression: Psychometric evidence and taxonomic
implications. J Abnorm Psychol 100: 316-336.
5. Watson D,
Pennebaker JW, Folger R (1986) Beyond negative affectivity: measuring stress and satisfaction in the
workplace. J Organ Behav Manage 8: 141-157.
6. McCrae RR, Costa PT (1987)
Validation of the five-factor model of personality across instruments and
observers. J Pers Soc Psychol 1: 81-90.
7. Watson D, Clark LA, Tellegen A
(1988a) Development and validation of brief measures of positive and negative affect:
the PANAS scales. J Pers Soc Psychol 54: 1063-1070.
8. Watson D, Carey LA, Carey G
(1988b) Positive and negative affectivity and their relation to anxiety and
depressive disorders. J Abnorm Psychol 97: 346-353.
9. Spector PE, O’Connell BJ (1994)
The contribution of personality traits, negative affectivity, locus of control
and Type A to the subsequent reports of job stressors and job strains. J Occup
Organ Psychol 67: 1-11.
10. Lindahl M, Archer T (2013)
Depressive expression and anti-depressive protection in adolescence. Stress,
positive affect, motivation and self-efficacy. Psychol4: 495-505.
11. Vallerand TJ (1997) Advances in
experimental social psychology: Toward a hierarchical model of intrinsic and
extrinsic motivation. Academic Press, New York.
12. Deci EL (1971) Effects of
externally mediated rewards on intrinsic motivation. J Pers Soc Psychol 18:
105-115.
13. Deci EL, Ryan RM (1985) Intrinsic
motivation and self-determination in human behavior. Plenum, New York.
14. Guay F, Vallerand RJ, Blanchard C
(2000) On the Assessment of Situational Intrinsic and Extrinsic Motivation: The
Situational Motivation Scale (SIMS). Motiv Emotion 24: 175-213.
15. Deci EL, Ryan RM (1991) Nebraska
Symposium on motivation: Perspectives on motivation. A motivational approach to
self. Integration in personality. University of Nebraska press, Lincoln.
16. Vallerand RJ,
Reid G (1988) On the
relative effects of positive and negative verbal feedback on males’ and
females’ intrinsic motivation. Can J Behav Sci 20: 239-250.
17. McAuley E, Duncan T, Tammen VV (1989)
Psychometric properties of the intrinsic motivation inventory in a competitive
sport setting: A confirmatory factor analysis. Res Q Exerc Sport 60: 48-58.
18. Moeller FG, Barratt ES, Dougherty
DM, Schmitz JM, Swann AC (2001) Psychiatric aspects of impulsivity. Am J
Psychiatry 158: 1783-1793.
19. Potenza MN (2007) To do or not to
do? The complexities of addiction, motivations, self-control and impulsivity.
Am J Psychiatry 164: 4-6.
20. American Psychological Association
(1994) Diagnostic and statistical manual of mental disorders. (4th
edn), Washington, DC.
21. Lynskey MT, Hall W (2001)
Attention deficit hyperactive disorder and substance use disorders: is there a
causal link? Addiction 96: 815-822.
22. Socialstyrelsen
(2011) Internationell statistisk klassifikation av sjukdomar och relaterade
hälsoproblem. Systematisk
förteckning. Svensk version (ICD-10-SE). The ICD-10 classification of mental
and behavioural disorders: clinical descriptions and diagnostic guidelines.
WHO, Geneva.
23. Zöller ME,
Karlsson E, Archer T (2009) Self-rated affect among adults presenting psychiatric diagnosis. Indiv
Differ Res 7: 14-28.
24. Endler NS,
Kocovski NL, Macrodimitris SD (2001) Coping, efficacy, and perceived control in acute vs. chronic illness.
Pers Indiv Differ 30: 617-625.
25. Bisschop MI,
Kriegsman DMW, Beekman ATF, Deeg DJH (2004) Chronic diseases and depression: the
modifying role of psychosocial resources. Soc Sci Med 59: 721-733.
26. Frank E, De
Raedt R (2007) Self-esteem
reconsidered: unstable self-esteem outperforms level of self-esteem as vulnerability
marker for depression. Behav Res Ther 45: 1531-1541.
27. Grinker R,
Vernon M, Mindel E, Rothstein DA, Easton H, et al. (1969) Psychiatric diagnosis, therapy and
research on the psychotic deaf. Department of Health, Education and Welfare,
Washington, DC.
28. Black PA, Glickman NS (2006)
Demographics, psychiatric Diagnoses, and Other Characteristics of North
American Deaf and Hard-of Hearing Inpatients. J Deaf Stud Deaf Educ 11:
303-321.
29. Pollard RQ (1994) Public mental
health service and diagnostic trends regarding individuals who are deaf or
hard-of-hearing. Rehabil Psychology 39: 147-160.
30. Palomo T,
Beninger RJ, Kostrzewa RM, Archer T (2008) Affective status in relation to impulsive,
motor and motivational symptoms: personality, development and physical
exercise. Neurotox Res 14: 151-168.
31. Huebner ES, Dew
T (1995) Preliminary
validation of the positive and negative affect schedule with adolescents. J
Psychoeduc Assess 13: 286-293.
32. Watson D, Clark L (1984) Negative affectivity:
the disposition to experience aversive negative states. Psychol Bull 96:
465-490.
33. Scheier MF, Carver CS (1985)
Optimism, coping, and health: assessment and implications of generalized
outcome expectancies. Health Psychol 4: 219-247.
34. Patton JH,
Stanford MS, Barratt ES (1995) Factor structure of the Barratt Impulsiveness Scale. J Clin Psychol 51:
768-774.
35. Stanford MS, Mathias CW, Dougherty
DM, Lake SL, Anderson NE, et al. (2009) Fifty years of the Barratt
Impulsiveness Scale: An update and review. Pers Indiv Differ 47: 385-395.
36. Li, C. R., Chen,
C-H. (2007).
Obsessive-compulsiveness and impulsivity in a non-clinical population of
adolescent males and females. Psychiatry Res 149: 129-138.
37. Fossati A, Di Ceglia A, Acquarini
E, Barratt ES (2001) Psychometric properties of an Italian version of the
Barratt Impulsiveness Scale-11 (BIS-11 in nonclinical subjects. J Clin Psychol
57: 815-828.
38. Someya T, Sakado
K, Seki T, Kojima M, Rest C, et al. (2001) The Japanese version of the Barratt
Impulsiveness Scale, 11th version, (Bis-11): its reliability and
validity. Psychiatry Clin Neurosci 55: 111-114.
39. Millet P (2005) Locus of control
and its relation to working life: studies from the fields of vocational
rehabilitation and small firms in Sweden. Doctoral Dissertation,
Arbetslivsinstitutet [Work life Institute], Luleå Technical University, Luleå,
Sweden.
40. Rotter JB (1966) Generalized
expectancies for internal versus external control of locus of reinforcement.
Psychol Monogr: Gen Appl 80.
41. Andersson G (1976)
Internal-external locus of control: some methodological notes on the research
and a factor analysis of a revised I-E scale. Department of Psychology Reports,
University of Göteborg.
42. Partridge C, Johnston M (1989)
Perceived control of recovery from physical disability: measurements and
prediction. Br J Clin Psychol 28: 53-60.
43. Erbin-Roesemann
MA, Simms L (1997) Work
locus of control: the intrinsic factor behind empowerment and work excitement.
Nurs Econ 15: 183-190.
44. Lefcourt HM (1991) Measures of
personality and Social Psychology: Locus of control. Academic Press: San Diego,
CA.
45. Vallerand RJ, Blais MR, Brière NM,
Pelletier LG (1989) Construction and validation of the Academic Motivation
Scale. Can J Behav Sci 21: 323-349.
46. Tabachnick BG, Fidell LS (2007)
Using Multivariate Statistics. (5th edn), Pearson Education, Inc.,
Boston.
47. Lundblad S, Garcia D, Hansson B,
Archer T (2015) Emotional Well-Being in Anorexia Nervosa: Negative Affect,
Sleeping Problems, Use of Mood-enhancing Drugs and Exercise Frequency. Arch
Depress Anxiety 1: 001-005.
48. Zöller M, Archer T (2009)
Predicting stress in male and female psychiatric patients and healthy
volunteers. Soc Behav Pers 37: 1081-1094.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5


QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Rheumatology Research (ISSN:2641-6999)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Allergy Research (ISSN:2642-326X)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- International Journal of Diabetes (ISSN: 2644-3031)


