654
Views & Citations10
Likes & Shares
Aspergillus is an opportunistic pathogen in oral cavity. The fungal hyphae are characteristically dichotomous, septate and branch at 45° acute angle. This case reports an intra-oral verrucal lesion over the dorsum of tongue with Aspergillus infection. On histopathologic examination, a verrucal lesion was seen with PAS-positive dichotomous, septate hyphae branching characteristically at 45° along with numerous spores.
Keywords: Verrucal, Aspergillus, Post-irradiation
INTRODUCTION
Aspergillus is a filamentous fungus found in varied sources like soil, plant waste etc. in immunocompromised individuals, Aspergillus appears in filamentous forms usually within the paranasal sinuses. Its occurrence in immunocompetent individuals has been sparsely reported. Head and neck radiation therapy alters the oral microflora significantly. Radiation-induced altered tissue response predisposes the mucosal microenvironment towards growth and sustenance of pathogenic microflora. Candidal overgrowth is the most commonly encountered oral condition post-irradiation. Other microorganisms include Streptococcus mutans, Lactobacilli and Spirochetes [1,2]. There is limited literature available in intraoral Aspergillus infection. Sethi et al. [3] reported Aspergillus lesion in an immunocompetent host. Similar finding was reported by Khatri et al. [4] affecting hard palate and nasal cavity. Uncommonly Aspergillus also has been reported in radiation sensitized oral mucosa1. This case report highlights Aspergillus infestation over a verrucal growth on dorsum of tongue in a 72 year old female patient.
CASE REPORT
A 72 year old female reported with the chief complaint of a small growth over the dorsum of tongue. Patient had undergone hemiglossectomy two years back for Verrucous Carcinoma of the tongue followed by a course of radiotherapy. The lesion was locally excised twice at a private clinic and after each excision, the lesion recurred. A biopsy was send obtained for histopathologic examination.
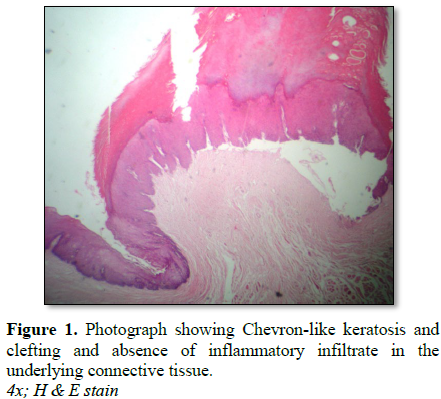
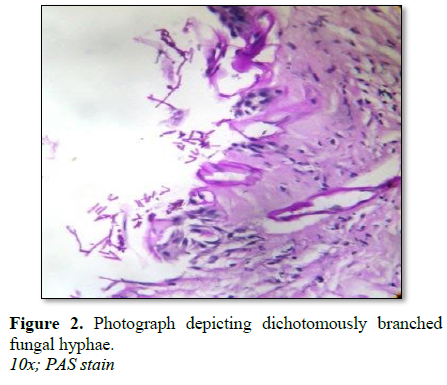
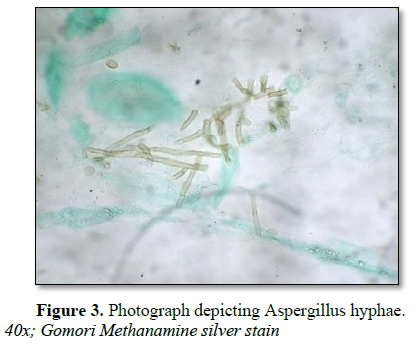
Grossly, the excised lesional tissue was white to pink in color with a rough to smooth surface, was firm in consistency and measured 1.8 × 1.2 × 0.8 cm. On histopathological examination, the lesion exhibited features of a hyperparakeratinised, stratified, squamous epithelium with a chevron-like keratosis and globular keratin formation in superficial layers. The lesion was elevated compared to adjacent mucosa and demarcated from the same by a constriction (Figure 1). Suprabasal and subepithelial clefting were evident. PAS-positive (Figure 2) and Gomori methanamine silver positive dichotomous, septate hyphae branching at 45° along with numerous spores (Figure 3) were seen within the areas of clefting and at the periphery of the verrucal growth as well in the superficial parakeratinized layers. Connective tissue was moderately collagenous with minimal inflammatory infiltrate. Laboratory culture was positive for Aspergillus growth.
DISCUSSION AND CONCLUSION
Shifts in microbial flora following radiation therapy have been reported till six months after cessation of exposure. The most common demonstrated species alteration have been studied in Candidal subpopulations although, Aspergillus spp. and Torulopsis glabtrata, can also be occasionally isolated [1]. The present case is the first ever reported case of an oral verrucal lesion with a superimposed Aspergillus infection two years, post-irradiation. Verrucal overgrowth in response to therapeutic radiation exposure has been reported previously on skin, however, never in oral cavity. Aspergillus is an opportunistic pathogen in man and can become pathogenic on previously damaged tissue [2]. In early stages of Aspergillus infection, epithelial cells show a loss of intercellular bridges, resulting in detachment of cells [3]. These features were seen in our case as areas of clefting. Underlying connective tissue stroma shows nil to minimal inflammatory cell infiltrate in early Aspergillus infection [2] which was consistent feature in the present case (Figure 2). Microbial culture was positive. Cases of Aspergillus infection have been reported in immunocompetent people as well [3,4]. The growth was completely excised and antimicrobial drug therapy was instituted. Healing was complete and uneventful [5,6].
CONFLICT OF INTEREST STATEMENT
There are no conflicts of interest.
1. Makkonen TA, Borthen L, Heimdahl A (1989) Oropharyngeal colonization with fungi and gram-negative rods in patients treated with radiotherapy of head and neck. Br J Oral Maxillofac Surg 27: 334-340.
2. Dreyer F, Bohle RM, Pohl Y, Rosseu S (1997) Sequestration of the alveolar bone by invasive aspergillus in acute myeloid leukaemia. J Oral Pathol Med 26: 437-440.
3. Myoken Y, Sugata T, Kya T (1996) Pathologic features of invasive oral aspergillosis with hematologic malignancies. J Oral Maxillofac Surg 54: 263-270.
4. Meikel D, Yarington C, Winterbauer R (1985) Aspergillosis of maxillary sinus in otherwise healthy patients. Laryngoscope 95: 776-779.
5. Dimitrakopoulos I, Lazaridis N, Asimaki A (2005) Craniofacial invasive aspergillosis in an immunocompetent patient: A case report. J Oral Maxillofac Surg 63: 84-88.
6. Martin MV, Tikriti UA, Bramley PA (1981) Yeast flora of the mouth and skin during and after irradiation for oral and laryngeal cancer. J Med Microbiol 14: 457-467.
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Journal of Allergy Research (ISSN:2642-326X)


