696
Views & Citations10
Likes & Shares
Three therapeutic
modules are evaluated in this study, hormones treatment (HT); a combination of
hormones with chemotherapy, radiotherapy or surgery (Mixed therapy, MT); and
observation (control group, CG), in prostate cancer patients. Comparison of the
fear of disease progression (FoP), emotional distress (ED) and quality of life
(QOL) indicated significant differences between the three patient groups. A
cross-sectional research design with questionnaires investigating FoP, ED and QOL
was used in this study. The participants were prostate cancer patients from a
regional hospital in Taiwan. Descriptive statistics were used to analyze data.
The control group had less emotional distress and a higher quality of life than
the other two treatment groups. This result shows that cancer treatment has a
negative impact on patient's life or mood. The results also show that the mixed
treatment can reduce patient's fear of cancer.
Keywords: Hormones therapy, Combination therapy, Prostate cancer, Fear of
disease progression, Emotional distress, Quality of life
INTRODUCTION
METHOD AND DESIGN
In this study, a cross-sectional study design
was used in the urology department of a regional hospital in southern Taiwan
for more than three months. The inclusion criteria were: (1) more than 20 years
of age; (2) a diagnosis of prostate cancer; (3) being conscious; and (4)
understanding that one has a diagnosis of prostate cancer. The exclusion
criteria were: (1) patients with a history of mental illness; (2) patients who
were unable to communicate; (3) patients how had other cancer diagnoses from
January 5 to January 1, 2016. A total of 38 cases were collected. Of these, 12
received the mixed treatment, 17 were treated with sertraline and 9 were in the
observation group. The treatment time of each group was three months.
RESULTS
The demographic data showed that all
participants were married. In the mixed treatment group, the average age was 70
years. Three participants had metastasis and nine did not. For the hormone
therapy group, there were seven participants with metastasis and ten without
metastasis. The average age was 76.12 years. In the observation group, no
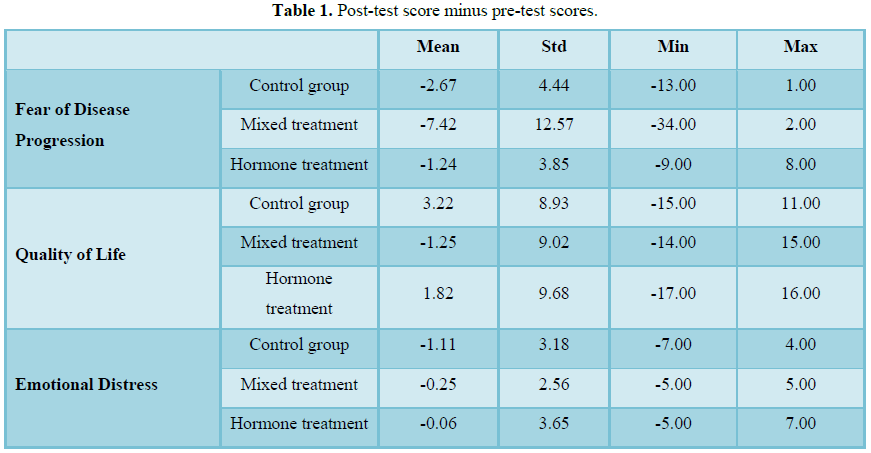
patient had metastasis, and the average patient age was 68.78 years old. Table
1 shows the fear of disease, quality of life problems and emotional
distress for the three treatment groups as well as the pre-test and post-test
score differences. The results showed that the mixed treatment group scored
better that the hormones treatment and observation group in regard to fear of
disease progression and the observation group scored better than the other two
groups in terms of quality of life. It is possible that the mixed treatment
needed to be given because the patients treatment protocol. There were no side
effects of medication or changes in physiological function after surgery in the
observation group. Therefore, the observation group had fewer problems
regarding quality of life. In terms of emotional disturbance, the observation
group also outperformed the other two groups, which may reflect that the side
effects of the treatment can cause the patient physical and mental discomfort.
DISCUSSION
This study site was conducted in a regional
hospital in a non-metropolitan area of southern Taiwan. Most of the cases were
older and the average age was 73 years old, which was in line with their age of
onset. The respondents were retired and did not obviously respond to the impact
and pressure of illness because they may not have been required to go to work.
Prostate cancer treatment includes prostatectomy, prostatectomy, radiation
therapy, hormone therapy and chemotherapy [4] and the mainstay of clinical practice
is hormone therapy. The majority of cases received hormone therapy in this
study, which accounted for 17.7% of the primary treatment options for treatment
with simpler hormones, which is close to half of the total patients.
Emotional distress is common in cancer
patients because it can be difficult to accept the facts of living with cancer:
a disrupted lifestyle, unbearable side effects of treatment and uncertainty of
the disease and treatment, along with the inability to grasp the fear and fear
of approaching death and other factors. The results of this study have put
forward the idea that the side effects of drugs used in cancer can cause
discomfort and lead to physical and psychological problems. Although the
literature shows that once a person has been diagnosed with cancer, negative
emotions, such as distressed sadness, fear of fear, disgust, rejection or
avoidance and censure and other negative or irrational thoughts and behaviors,
may occur [5,6]. However, the patient may be less psychologically responsive
because of being older and instead focus more on physical changes. Therefore,
future care for prostate cancer cases should be based on reducing physical
emotions as the primary goal of medical care. In addition, the patient’s fear
of being exposed to an unpredictable process during treatment, such as
incontinence, pain, tiredness, nausea, vomiting, and loss of body, home and
social functions, should be considered. The year-long follow-up results
indicate that patients undergoing radical surgery have more post-operative
erectile dysfunction and urinary incontinence and are 3 to 5.5 times more
likely to have long-term negative effects than healthy men [7], which affects
the quality of life of patients with prostate cancer [8]. The results are consistent
with an issue that must be taken seriously.
Regarding the fear of disease progression,
the literature shows that suffering from a disease is a life-threatening
process. In particular, when patients face the impact of cancer, they can
experience physical and psychological distress and fear due to the illness [9].
Fear of the progression of the disease is experienced through personal feelings
because the unknown course of the disease threatens physical health, which is
an emotion stemming from the fear of a possible future recurrence of serious
illness experiences and the inability to control their thoughts regarding these
issues the series of treatment [10,11]. In recent years, for prostate cancer,
monitoring behavior and providing additional support to the high-risk group of
patients has been applied, similar to the additional support provided to breast
cancer patients [12]. Studies of rectal cancer and lung cancer have shown that
fear of disease progression or relapse has become a problem for the most common
or second most common cancer patients, with 49% of prostate cancer patients
showing fear of disease progression or recurrence [13,14]. A European study of
patients with cancer showed that 13% of cancer patients had moderate or severe
fear of disease progression, which was associated with the prognosis of their
cancer. The length of diagnosis was not correlated with the type of cancer.
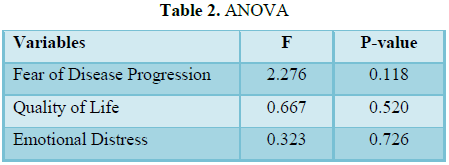
There were no statistically significant differences between the three groups in
this study, mainly due to the small number of cases.
In terms of quality of life [15] concluded
that quality of life of cancer patients should include both positive and
negative feelings of physical, emotional, social and cognitive functions. The
most important subjective feelings are the mood of the patients and the
treatment side effects. Cognition and quality of life are mostly biased
subjective concepts, that is, they stem from the individual's subjective
cognitive, positive and negative emotional response, and physical, mental and
spiritual health are used to assess overall satisfaction with life. For cancer
patients, quality of life can be used as an important indicator for evaluating
health and medical measures [11,16]. Arndt et al. [17] and is particularly
important in young adults younger than 50 years of age compared to older patients.
Most of the cases in this study were retired, and therefore had less stressful
lives. In addition, regarding the idea of “functional life quality”, the
simpler hormone therapy had a lower functional quality of life than the
observational group, but the mixed treatment and simpler hormone therapy still
had a functional quality of life at a high standard. Although the statistical
tests did not reach significant levels because of the small number of cases, we
can still make some reasonable inferences from the means.
1.
Fitzmaurice C, Allen C, Barber RM, Barregard L,
Bhutta ZA, et al. (2017) Global, regional and national cancer incidence,
mortality, years of life lost, years lived with disability and
disability-adjusted life-years for 32 cancer groups, 1990 to 2015: A systematic
analysis for the global burden of disease study. JAMA Oncol 3: 524-548.
2.
Siegel RL, Miller KD, Jemal A (2015) Cancer statistics
2015. Cancer J Clin 65: 5-29.
3.
Carter N, Bryant-Lukosius B, DiCenso A, Blythe J,
Neville AJ (2011) The supportive care needs of men with advanced prostate
cancer. Oncol Nurs Forum 38: 189-198.
4.
Miller KD, Siegel RL, Lin CC, Mariotto AB, Kramer
JL, et al. (2016) Cancer treatment and survivorship statistics 2016. Cancer J
Clin 66: 271-289.
5.
Brandes K, van der Goot MJ, Smit EG, van Weert JC,
Linn AJ (2017) Understanding the interplay of cancer patients instrumental
concerns and emotions. Pat Educ Counsel 100: 839-845.
6.
Jimenez RB, Perez GK, Rabin J, Hall D, Quain K, et
al. (2017) Fear of recurrence among cancer survivors. J Clin Oncol 10053.
7.
Mohamad Al-Ali B, Ponholzer A, Augustin H, Madersbacher
S, Pummer K (2017) The long-term effect of radical prostatectomy on erectile
function, urinary continence and lower urinary tract symptoms: A comparison to
age-matched healthy controls. BioMed Res Int.
8.
Orom H, Nelson CJ, Underwood W, Homish DL, Kapoor DA
(2015) Factors associated with emotional distress in newly diagnosed prostate
cancer patients. Psycho-oncology 24: 1416-1422.
9.
Parker PA, Davis JW, Latini DM, Baum G, Wang X, et
al. (2015) Relationship between illness uncertainty, anxiety, fear of
progression and quality of life in men with favorable-risk prostate cancer
undergoing active surveillance. BJU Int.
10.
Kate J (2015) Fear of recurrence persists for many
cancers survivors. Paper presented at the European Society for Radiotherapy and
Oncology (ESTRO). 3rd Forum: Barcelona, Spain.
11.
Kirschner-Hermanns R, Jakse G (2002) Quality of life
following radical prostatectomy. Crit Rev Oncol Hematol 43: 141-151.
12.
Mehnert A, Berg P, Henrich G, Herschbach P (2009)
Fear of cancer progression and cancer-related intrusive cognitions in breast
cancer survivors. Pycho-oncology 18: 1273-1280.
13.
Herschbach P, Berg P, Dankert A, Duran G,
Engst-Hastreiter U, et al. (2005) Fear of progression in chronic diseases: Psychometric
properties of the fear of progression questionnaire. J Psychosom Res 58:
505-511.
14.
Simard S, Savard J (2009) Fear of cancer recurrence
inventory: Development and initial validation of a multidimensional measure of
fear of cancer recurrence. Support Care Cancer 17: 241-251.
15.
Bottomley A (2002) The cancer patient and quality of
life. Oncologist 7: 120-125.
16.
Lavdaniti M, Nikolaos T (2015) Definitions and
conceptual models of quality of life in cancer patients. Health Sci J 9: 6.
17.
Arndt V, Koch-Gallenkamp L, Jansen L, Bertram H,
Eberle A, et al. (2017) Quality of life in long-term and very long-term cancer
survivors versus population controls in Germany. Acta Oncologica 56: 190-197.
-
 Table 1
Table 1 -
Table 2
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Pathology and Toxicology Research
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Journal of Allergy Research (ISSN:2642-326X)


