6979
Views & Citations5979
Likes & Shares
Background:
Finasteride is one of the common drugs used in androgenetic alopecia.
Literature speaks about sexual side effects in about 2% of the patients. To
overcome this, we used topical Finasteride.
Objective:
To know the efficacy of topical Finasteride it is compared with oral
Finasteride along with minoxidil.
Materials
and Methods: We
randomized about 107 subjects, aged 18-40 years, who came for outpatient
consultation for male pattern androgenetic alopecia into two groups. One group
(group A) treated with Finasteride 1 mg
tablet and topical 5% minoxidil solution, another group (group B) treated with 0.1%
topical Finasteride with 5% minoxidil solution for 06 months of study period.
Results:
Analysis of the extent of bald area, hair count and number of terminal
hair showed no significant difference in both the groups.
Conclusion:
Analysis showed no significant difference in the therapeutic response,
both topical and oral Finasteride found to be equally effective. So, topical Finasteride found to
be a safe alternative drug, with high compliance that avoids the unnecessary
fear of sexual side effects in the mind of the patients.
INTRODUCTION
Loss of hair is a worrisome problem for many men. The main cause of the
same is androgenetic alopecia. The supposed to be the drug of choice in male
pattern androgenetic alopecia treatment is finasteride. Finasteride 1mg is used
all over the world for the treatment of androgenetic alopecia [1]. It is
approved in the USA and many other countries. On oral Finasteride administration about 2% [2] of the
patients had side effects, the common one was erectile dysfunction, loss of
libido and decreased ejaculate volume. However, a study conducted by this
article author & another study conducted by Tosti et al. [3] showed that
the sexual and erectile function of those subjects who were treated with
Finasteride orally was not reduced compared with their age related
controls. Finasteride’s efficacy is
proven by various clinical trials in adult men with predominant vertex,
anterior and midscalp region [4-6].
The main mechanism in androgenetic alopecia is miniaturization of hair due to the effect of androgen especially dihydrotestosterone. Finasteride is a type 2,5 alpha reductase inhibitor, it inhibits dihydrotestosterone conversion from testosterone. Dihydro testosterone is active form of testosterone; produced from testosterone by type 2, 5 alpha reductase [7]. Although, testosterone, is responsible for sexual function after puberty, and it is not by the dihydrotestosterone. In spite of the explanation and clinical trials, people were afraid to use oral Finasteride. To overcome this, topical finasteride was attempted in patients of androgenetic alopecia.
MATERIALS
& METHODS
We randomized about 107 subjects, aged 18-40 years, who came for outpatient consultation for male pattern androgenetic alopecia into two groups. They were diagnosed clinically as male pattern hair loss [8]. One group (group A) treated with Finasteride 1 mg tablet with topical 5% minoxidil solution and another group (group B) treated with 0.1% topical Finasteride with 5% minoxidil solution after informed consent from both of them.
Inclusion criteria were as follows: Age 18-40 years, maximum diameter of the bald area less than 10 cms, with good physical health, patient stopped previous treatments for androgenetic alopecia for a period of six months. Exclusion criteria were patients on treatment for hair loss and those patients who various other cause for hair loss other than androgenetic alopecia.
Group A were provided with 5% minoxidil solution to apply twice daily and Tab.Finasteride 1mg to be taken orally once a day. The other group, group B is provided with 5% minoxidil and 0.1% Finasteride solution combination solution to apply on the scalp twice daily.
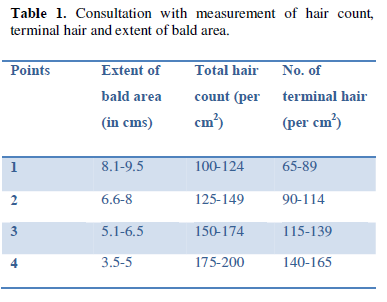
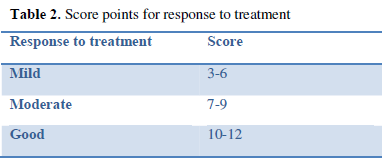
To evaluvate the medicines effect, patient were consulted before the study, after fortnight then every month end for follow up. Every time during consultation, the extent of the bald area, total hair count and terminal hair count in per cm2 area was studied. On the directions of the study conducted by Hajheydari et al. [9] extent of the bald area (in cms), total hair count (per cm2) & number of terminal hair (per cm2) is provided by with the following points as given in Table 1. The responses of the treatment were scored as given in table 2. By calculating the number of people falling in good, moderate and mild, those results were depicted in Table 4 in an month wise manner.
All procedures followed were in accordance with the ethical standards
of the responsible committee on human experimentation (institutional and
national) and with the Helsinki Decleration of 1964, as revised in 2013.
Informed consent was obtained from all patients for being included in the
study.
RESULT
About 107 patients of androgenetic alopecia were randomly enrolled for
the study with their consent. 55 patients were assigned in the group A and 52
patients were assigned to group B.
In group A, 1 patient stopped finasteride due to decreased libido, 1
patient left treatment due to cost factor and 3 patients due to poor
compliance. 50 patients completed the study for 6 months.
In group B, 1 patient stopped medication due to cost factor and one
patient lost to follow up. In this group 50 patients were followed up till the
end of the study period.
There is a good reduction in the size of the bald area by one cm from
the end of the third month onwards in both the groups.
Subjective and objective improvement of hair growth was felt by most of
the patients from the second month end onwards.
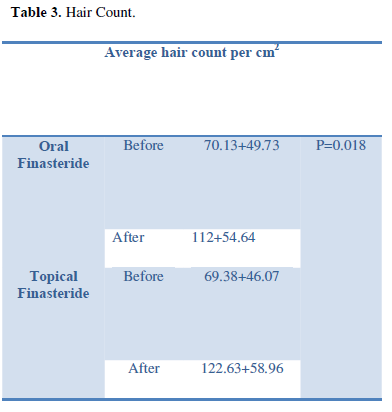
The average hair count before and after therapy was well depicted in Table 3 with p=0.018.
Very few patients felt not much improvement even after 6 months of
treatment.
Three patients in group A and Two patients in group B felt mild burning
sensation and erythema on application of topical medications that was treated
with antihistamines and mild topical steroids.
One patient in group A complained of sexual problem after taking
Finasteride oral medication, but no complaint of any sexual problem in group B
patients.
The results of the study (Table
4) revealed that there is equally good response to both group (group A) treated with oral Finasteride 1 mg with
topical 5% minoxidil and another group (group B) treated with topical
Finasteride with minoxidil (Graph 1).
DISCUSSION
The main
mechanism in androgenetic alopecia is miniaturization of hair follicle. The
mature terminal hair turns to vellus hair [10] due to the effect of androgen
especially dihydrotestosterone. Testosterone is converted to 5 alpha
dihydrotestosterone. The enzyme causing this is 5 alpha reductase. 5 alpha
dihydrotestosterone is five times more potent than testosterone. This
dihydrotestosterone attaches itself to the androgen receptors of the
genetically marked hair follicle that causes the miniaturization. Not only
miniaturizations occur even the rate of hair growth reduces [11].
Finasteride, a azasteroid is a type 2
isoenzyme, 5 alpha reductase inhibitor [12,13], which inhibits
dihydrotestosterone conversion from testosterone. This type 2 isoenzyme is
present in the hair follicles and its activity is important in controlling the
end organ hyperactivity causing androgenetic alopecia.
The
results of the study (Table 4)
revealed that there is equally good response to both group (group A) treated with oral Finasteride 1 mg with
topical 5% minoxidil and another group (group B) treated with topical
Finasteride with minoxidil. Both groups started getting response to the therapy
from the end of second month onwards.
Very few patients, 03 patients in group A and
02 patients in group B 01 patient felt mild burning sensation and erythema on
application of topical medications, that was treated with antihistamines and mild topical steroids showing the topical
preparations were relatively safe. But the undesired side effect loss of libido
was reported by 01 patients of group A who were taking Finasteride, because of
this he was dropped out of the study course. This was proved by many studies in
the past like Leyden et al. [4] and Kaufman et al. [14] has shown 2%
of patients had sexual side effects. However, RCT conducted by this article
author [15] and another study conducted by Tosti et al. [3] proved, sexual and erectile function of those
subjects who were treated with Finasteride orally was not reduced compared with
their age related controls. Patients of group B didn’t complain of the same.
So, topical finasteride found to be a much safe and equally effective drug,
with high compliance that avoids the unnecessary fear of sexual side effects in
the mind of the patients.
CONCLUSION
Not only
oral even the topical Finasteride found to be a much safe and equally effective
drug, with high compliance that avoids the unnecessary fear of sexual side
effects in patients.
1. Roberts JL,
Fielder V, Imperato-McGinley J (1999) Clinical dose ranging studies with
Finasteride, a type 2 5 alpha reductase. J Am Acad Dermatol 40: 930-937.
2. Kenneth AA, Jeffrey TS Hsu (2001) Manual of
Dermatologic therapeutics.
3. Tosti A, Piraccini
BM, Soli M (2001) Evaluvation of sexual function in subjects taking finasteride
for the treatment of androgenic alopecia. JEADV 15: 418-421.
4.
Leyden J, Dunlap
F, Miller B (1999) Finasteride in the treatment of men with frontal male
pattern hair loss. J Am Acad Dermatol 40: 930-937.
5. Brenner
S, Matz H (1999) Improvement in androgenic alopecia in 53-76 years old men using
oral Finasteride. Int J Dermatol 38: 928-930.
6. Price VH, Menefee E, Sanchez M, Ruane P, Kaufman KD
(2002) Changes in hair weight and hair count in men with androgenetic alopecia
after treatment with Finasteride, 1 mg, and daily. J Am Acad Dermatol 46: 517-523.
7. Valia RG, Valia AR (2002) IADVL textbook of
Dermatology.
8.
Olsean EA (2001) Hamilton-Norwood
classification of pattern hair loss in men. Female pattern hair loss. J Am Acad
Dermatol 45: 70.
9.
Hajheydari Z, Akbari J, Saeedi M, Shookoohi L
(2009) Comparing the therapeutic effects of Finasteride gel and tablet in
treatment of the androgenetic alopecia. Indian J Dermatol Venerol Leprol 75: 47-51.
10. Kligman AM (1998) The comparative histopathology of
male pattern baldness and senescent baldness. Clinics in dermatology.
Lippincot, Philadelphia, PA.
11. Hoffmann R, Van Neste D (2005) Recent findings with
computerized methods for scalp hair growth measurements. J Invest Dermatol Symp
Proc 10: 285-288.
12.
Jennifer A
Cafardi (2012) The manual of Dermatology. Springer International.
13.
Klaus W,
Goldsmith LA, Stephen IK, Barbara AG, Amy SP, et al. (2012) Fitzpatrick’s
Dermatology in general medicine.
14.
Kaufman KD,
OLsean EA, Whiting D (1998) Finasteride in the treatment of man with
androgenetic alopecia. J Am Acad Dermatol 39: 578-579.
15.
Narasimhalu CRV (2015) Randomized
questionnaire based case-control research study on evaluation of the sexual
function in Indian patients taking oral Finasteride for androgenetic alopecia.
Dermatol and Therap (Heidelb) 4: 231-234.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4


QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Stem Cell Research and Therapeutics (ISSN:2474-4646)
- International Journal of Clinical Case Studies and Reports (ISSN:2641-5771)
- International Journal of Surgery and Invasive Procedures (ISSN:2640-0820)
- International Journal of Anaesthesia and Research (ISSN:2641-399X)
- Journal of Cardiology and Diagnostics Research (ISSN:2639-4634)
- International Journal of AIDS (ISSN: 2644-3023)
- Journal of Renal Transplantation Science (ISSN:2640-0847)


