807
Views & Citations10
Likes & Shares
Background: Mycosis fungoides (MF) is a primary
cutaneous T-cell lymphoma that usually presents clinical indolent behavior,
although some patients evolve towards advanced stages of the disease, despite
adequate treatment, having therefore worse prognosis. The refinement of the
prognostic evaluation of these patients is considered of interest.
Aim: Evaluate histopathological factors with
prognosis importance.
Methods: We proceed a cross-sectional study based on
the review of the first histopathological examinations of patients with early
stage MF (IA and IB), with at least 5 years follow-up. Several
histopathological variables were analyzed and related to progression of disease
and death. Prevalence ratios and their respective confidence intervals were
calculated as association measurements; a p value of 5% was adopted.
Results: Sixty-one patients, with medium follow-up of
8.2 years, presented 26.2% of staging progression and 6.6% of MF related death.
Parakeratosis (PR: 2,636, p=0.03 e CI 95%: 1.1-6.0) and superficial and deep
perivascular pattern of the lymphoid infiltrate (PR: 3.056, p=0.036 e CI 95%
1.4-6.5) were associated with disease progression and death (PR: 27.50, p=0.02
e CI 95%: 3.3-224.6). On the other hand, histopathological features usually
related to poor prognosis, such as the presence of Pautrier's microabscesses,
folliculotropism and enlarged nuclei atypical lymphocytes, were not associated
with the outcomes studied.
Conclusion: Parakeratosis and a superficial and deep
lymphoid infiltrate pattern may have prognostic value. Retrospective character
and small sample are limitations of this study. These findings should be tested
in prospective studies with different samples.
Keywords: Lymphoma, Lymphoma, T-cell, Cutaneous,
Mycosis fungoides
INTRODUCTION
Mycosis fungoides (MF) is a low-grade
malignant T-cell epidermotropic lymphoma that onsets on the skin. It is the
most prevalent form of primary cutaneous T-cell lymphoma (CTCL), which accounts
for approximately 50% to 65% of cases. The disease often takes an indolent course,
but in approximately one-third of the patients, the disease progresses to an
aggressive malignancy with a poor prognosis [1,2].
The staging classification system for MF is known as TNMB and it is
based on the evaluation of skin involvement patterns (T), lymph node
involvement (N), disease extension to other organs (M) and, finally, to
peripheral blood (B). TNMB stage represents the main prognostic factor for
patients with MF [3].
Early-stage MF (Stages IA, IB and IIA), which
represents the majority of the patients at the time of the diagnosis, shows a
favorable prognosis, with 10-years specific survival rates of more than 95% for
stage IA and about 80-85% for stage IB [4-7].
While the majority of patients
with early-stage MF will not advance to late-stage disease, such progression
may occur. Rates of progression may vary between 4-13% of patients with
clinical stage IA and 21 to 27% with stage IB [5-9].
Therefore, it is essential to
distinguish this group of patients that are at greater risk of having worse
outcomes. It is of interest to investigate other possible factors capable of
refining prognostic evaluation, besides the TNMB staging system.
Histopathological exams of patients diagnosed
with early-stage MF from the Photo dermatology Sector of the University
Hospital Clementino Fraga Filho (HUCFF) of the Federal University of Rio de
Janeiro (UFRJ), were reviewed in order to investigate possible
histopathological features that could be related to prognosis.
MATERIALS
AND METHODS
The current research is an observational,
cross-sectional study based on the review of histopathological examinations
performed in patients diagnosed with early-stage MF.
Inclusion criteria
·
Early-stage MF, defined by Pimpinelli et
al. [10]. The aforementioned criteria were retrospectively applied based on the
first biopsy examination performed at our institution. Four points at least
were required (as proposed by the algorithm). We highlight that our institution
does not have access to clonality T-cell receptor gene rearrangements
examination. In this way, clinical, histopathological and immunohistochemical
criteria (CD 2, 3, 5 and 7) were used;
·
Adult patients, with 18 years old or
more;
·
TNMB staging IA or IB (Disease
restricted to the skin);
·
Five-year follow up or more.
Exclusion criteria
·
Insufficient data on medical charts;
·
Unavailable histopathological exams for
revision or insufficient material on paraffin blocks to perform
immunohistochemical analysis;
·
Positive serology to HTLV 1 and 2.
Study population comprised MF
patients diagnosed, treated and followed-up in the Photo dermatology Sector of
HUCFF/UFRJ, between January 2000 and December 2015. Early stage cases were
selected based on the current TNMB staging system [3]. All patients underwent
laboratory exams (complete blood white count, serum LDH and beta-2-microglobulin)
and imaging exams (chest x-ray and abdominal ultrasound for the majority and,
more recently, computed tomography scans including thorax, abdomen and pelvis).
The first histopathological
examinations that which confirmed a diagnosis of MF were selected. All patients
were stage IA or IB at the time of diagnostic confirmation. All the exams were
reviewed by two dermato pathologists, who did not know the original medical
report and together performed and accorded the analysis of the specific
established histological parameters. Only histological sections stained with
hematoxylin and eosin were evaluated. Some patients had more than one biopsy
taken from different anatomical sites at the same time; in these cases, samples
were evaluated together and the evaluation was set considering the conjoint of
histopathological findings.
The dependent variables evaluated were:
·
Disease progression (staging) treated in
a qualitative, dichotomous and nominal manner. Since patients at stages IA or
IB were included in the study, all those who progressed to stage IIA onwards
were categorized as disease progression.
·
MF-related death (due to lymphoma or to
complications arising from systemic therapies). This variable was also treated
in a qualitative, dichotomous and nominal manner.
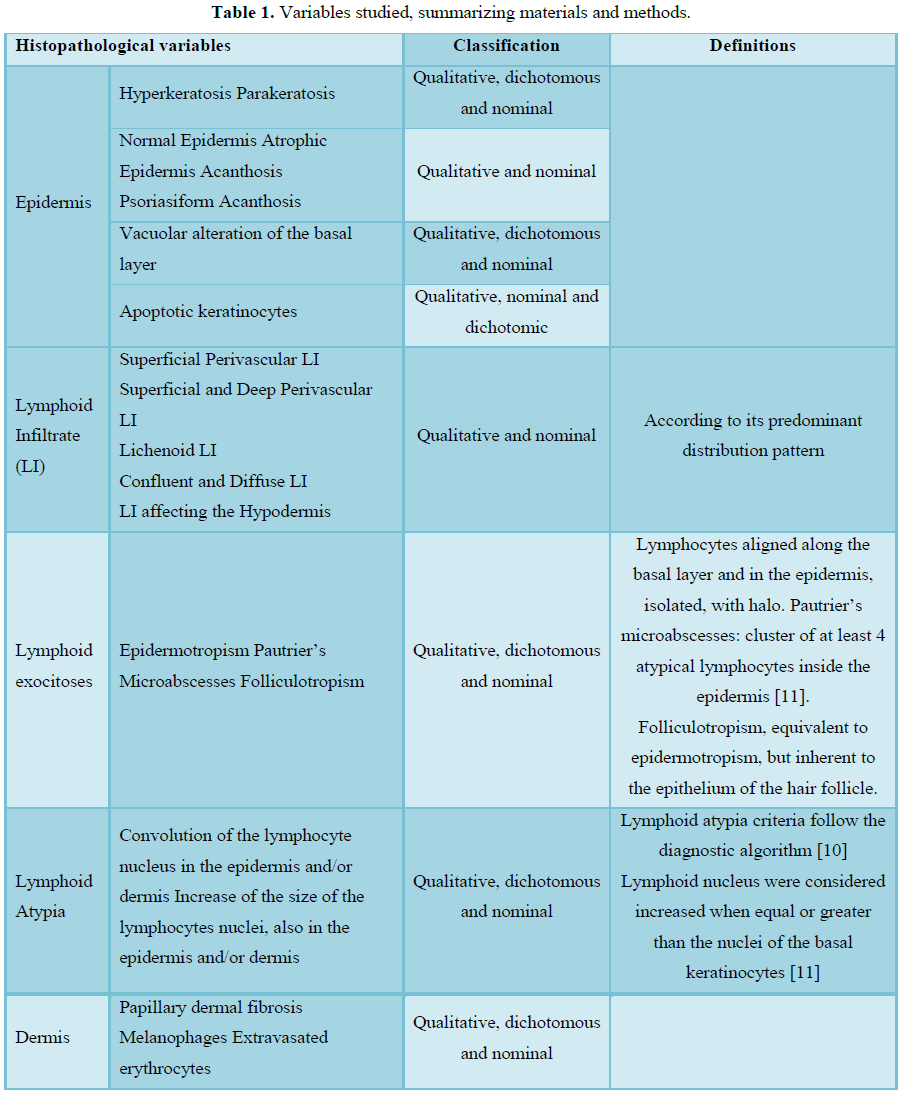
Histopathological independent variables are
summarized in Table 1.
Data were
gathered in Excel (Microsoft® Excel® for Mac
2011/Version: 14.2.0) and analyzed in the SPSS statistical software, version
24.0. The chi-square test (X2)
or Fischer’s exact test, were applied to investigate the association between
qualitative independent variables.
Prevalence ratios and their respective
confidence intervals (CI: 95%) were calculated as association measurements. The
significance criterion was 5%. Finally, Multivariate
Poisson regression was performed to help identify independent predictors
for the events and to estimate their corresponding prevalence ratio.
The current study complies with the National
Health Council Resolution 466/12; it is registered in Plataforma Brasil (Brazil Platform) and was approved by
CEP-HUCFF/UFRJ - CAAE: 59235916.9.0000.5257.
RESULTS
One hundred and
thirty-five (135) patients were selected at the outpatient clinic; however,
only 102 early-stage MF patients were included based on medical reports analysis.
Among the 33
excluded patients, 17 were due to insufficient clinical data, 10 received a
different diagnosis after revision (lymphomatoid papulo Sixty-seven of the 102
patients selected had their first histopathological examinations available for
adequate revision along with paraffin blocks containing biopsied tissue
sufficient for subsequent immunohistochemical analysis of CD 2, 3, 5 and 7.sis
and granulomatous slack skin lymphoma) and 6 had positive HTLV serology.
Of those 67
patients, 61 scored 4 points after retrospective application of Pimpinelli’s
criteria, therefore corresponding to the total sample [10].
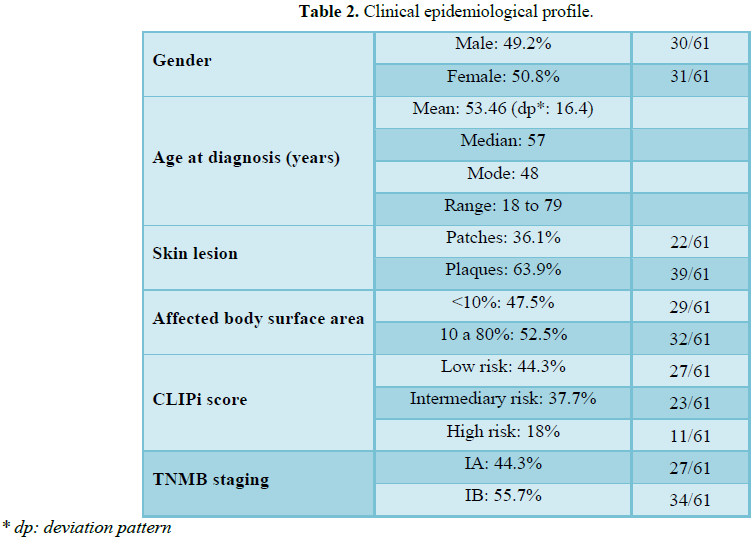
Table 2 summarizes clinical aspects of our sample.
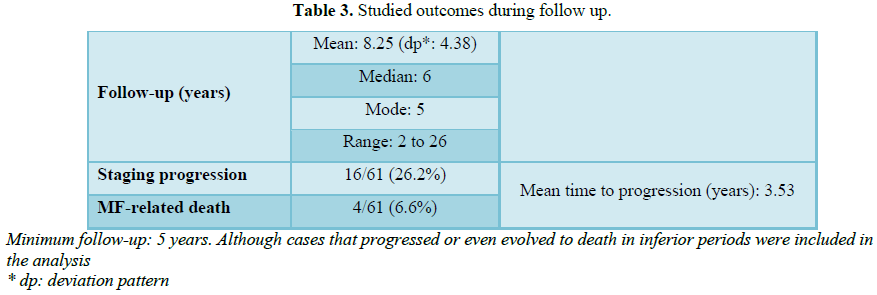
Table 3 shows the outcome variables and reflects the evolution of the
studied sample during outpatient follow-up.
Out of the 16
patients who progressed in staging, 25.0% advanced to IIA (N1); 12.5%, to IIB
(T3); and 50%, to IIIA (T4). Of the 2 remaining patients, 1 progressed to stage
IIIB (T4 + B1) and 1, to stage IVA (T4 + B2).
Eight (8)
patients died along the follow up period and the outcome was associated with MF
in 4 of them. All had progressed in staging and died due to infectious
complications associated with chemotherapy.
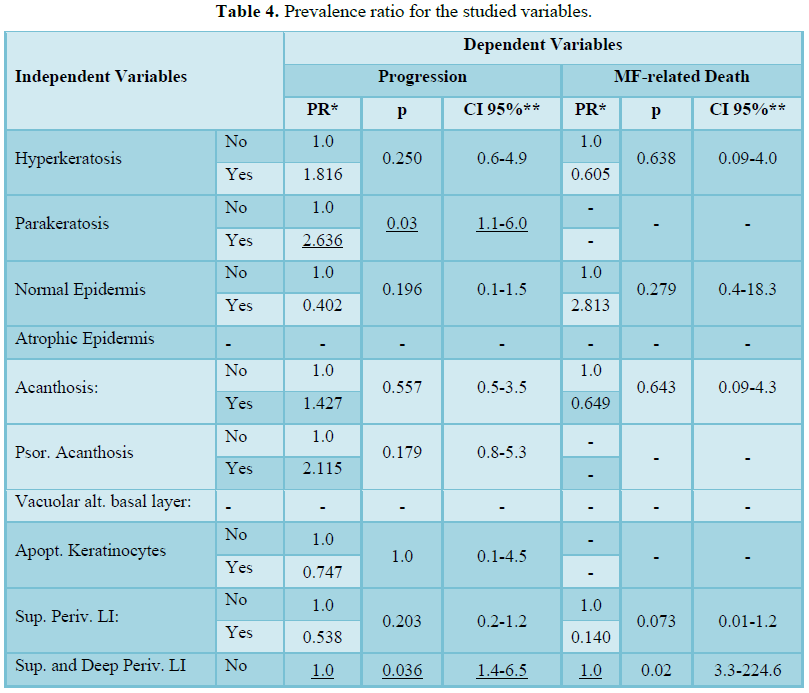
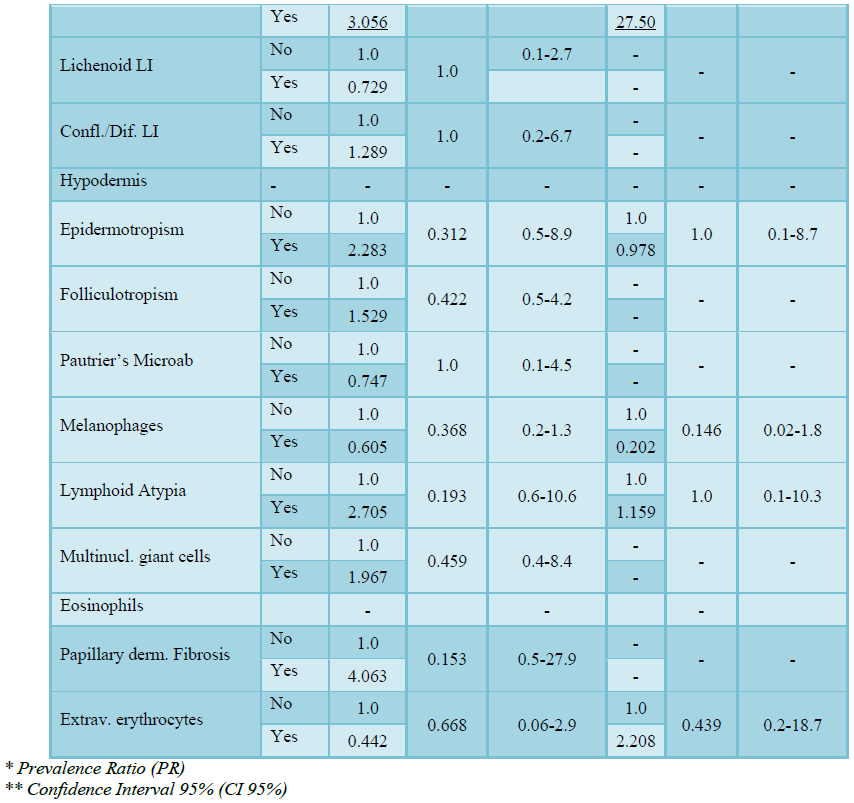
Results of
association measurements between independent histopathological and dependent
variables are shown in Table 4.
The incidence
of hyperkeratosis did not show correlation with disease progression or death.
On the other hand, the incidence of parakeratosis indicated higher prevalence
of staging progression (PR=2.636, p=0.03 and CI 95% 1.1-6.0).
Epidermal
changes (epidermis presenting normal thickness, atrophy, acanthosis,
psoriasiform acanthosis, vacuolar changes in the basal layer and, finally,
apoptotic basal keratinocytes) did not correlated with dependent variables.
Superficial
perivascular-pattern lymphoid infiltrates was present in 77% of the patients,
whereas the lichenoid-pattern was found in 13.1% of them. Superficial and deep
perivascular infiltrates, were found in 9.8% of the cases. It is worth
emphasizing that the lymphoid infiltrates was classified by taking into
consideration the predominant pattern in comparison to another more focal
pattern eventually combined. There was statistically significant correlation
between the identification of the lymphoid infiltrate of superficial and deep
perivascular pattern and the incidence of both disease progression (PR: 3.056,
p=0.036 and CI 95% 1.4-6.5) and disease- related death (PR: 27.50, p=0.02 and
CI 95% 3.3-224.6). The same outcome was not observed in other lymphoid
infiltrate patterns investigated in the current study.
Variables such
as Pautrier’s microabscesses (PM), folliculotropism and lymphocytic atypia did
not show statistically significant correlation to the analyzed dependent
variables.
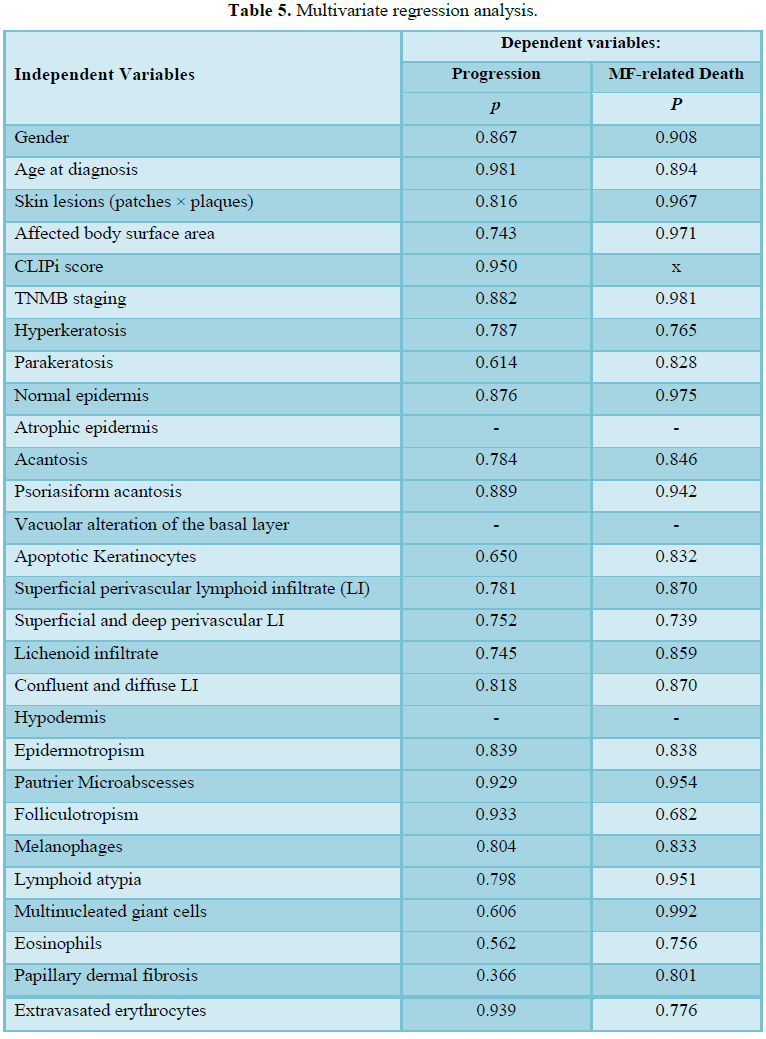
No
statistically significant association was found in the multivariate regression
test when all variables were studied (Table
5).
DISCUSSION
We carried out an observational,
cross-sectional study focused on reviewing the first histopathological exams
performed in 61 patients diagnosed with early-stage (IA and IB) MF, based on
criteria set by Pimpinelli et al. [10].
PM incidence, atypical lymphocytes with
cerebriform nuclei in the dermis, folliculotropism and large cells suggesting
progression to large-cell transformation are acknowledged as the worst
histopathological prognostic factors [12-14].The aforementioned factors were
compiled from different studies and not all of them are unanimous among the
authors.
Disease progression presented statistically
significant association between the incidence of parakeratosis and the
superficial/deep perivascular pattern of the lymphoid infiltrate.
Patients presenting parakeratosis recorded
higher prevalence of disease progression than patients who did not present it.
The magnitude of the increased prevalence reached 2.6x. Likewise, the
superficial/deep perivascular pattern was significantly associated with increased
prevalence of staging progression during follow-up.
Superficial and deep perivascular infiltrate
was the only variable associated with disease-related death, the prevalence
being 27 times higher. The likelihood of certainty of this finding is low given
the small numbers involved.
Studies focused on analyzing
histopathological prognostic factors remain scarce. Vonderheid et al. [4]
investigated possible histopathological and immunohistochemical factors with
prognostic influence and found association between worse outcomes and factors
such as the incidence of large MPs (clustering of 10 or more atypical
lymphocytes) and lymphocytes with hyperchromatic and vesicular nuclei in the
dermis. However, there was no association between infiltrate structure and the
investigated events [4].
Smoller et al. investigated 24
histopathological criteria in patients belonging to 2 MF groups: 21 patients
with stable disease who followed a usual and slowly progressive course versus
26 patients who were rapidly progressive and had worse prognosis. The incidence
of parakeratosis and the lymphoid infiltrate pattern were taken into
consideration among the investigated criteria. There was no statistical
significance in any of the two parameters; the degree of epidermal acanthosis
was the only factor likely to have prognostic influence. Rapidly-progressive
patients tended to have a canthotic epidermis. Their distinct findings as
compared to ours may be related to sampling. Although total number was similar,
Smoller et al. [15] study involved a larger number of patients with rapidly-progressive
disease course.
The degree of infiltration of clinical
lesions correlates to the intensity and depth of the lymphoid infiltrate [16].
According to Marti et al. [17] the greater the infiltrate thickness (measured
from the granular layer to the end of the dermal infiltrate), the worse the
prognosis. Four of the 6 cases classified as superficial and deep perivascular
lymphoid infiltration had focal lichenoid pattern. Thus, worse prognosis may be
associated with the increased number of lymphoid cells infiltrating the skin,
which corresponds to increased tumor burden. In fact, the concept is taken into
account in the TNMB staging since it considers spots, plaques or tumors
clinical lesions. On the other hand, there was no association between lichenoid
infiltrate and the evaluated outcomes.
Parakeratosis is an abnormal epithelial
cell-maturation process that leads to nuclei retention in the stratum corneum,
which is normally anucleate. It is observed in many pathological skin
conditions, accompanied or not to changes in the malpighian layer though its
association to an accelerated cell turnover, and is often seen in patients with
early-stage MF [18,19]. Based on results of the exploratory analysis conducted
after the identification of such association, we found that the incidence of
parakeratosis was associated with epidermal acanthosis (RP: 1.623; p=0.006; CI
95%: 1.2-2.1), which in turn was more often, although not significantly,
associated with epidermotropism (p=0.3). So, we hypothesize that a greater
epidermal lymphoid permeation with sequent epidermal reaction could lead to
parakeratosis. Therefore an increased tumor burden in this setting could
justify such unprecedented association. From another point of view, intense
pruritus correlates to worse MF prognosis [13]. Scratching can cause
excoriation and histopathologically result in spongiosis and tissue healing,
parakeratosis included in the process. Since “pruritus” was not a clinical
variable it was not possible to test such hypothesis at this time.
However, it is worth highlighting that Smoller
et al. [15] investigated the prognostic value of parakeratosis and did not find
such association.
We did not find statistically significant
association between the incidence of Pautrier’s microabscesses and disease
progression, despite the positive Pautrier’s microabscess prevalence ratio,
which would denote tendency to higher progression prevalence.
Folliculotropism is pointed out as worse
prognosis factor, being one of the criteria adopted in the CLIP score
[5,12,20]. According to the study conducted by Nikolau et al. [13] with 473
patients from two different lymphoma centers, the incidence of folliculotropism
was associated with disease progression to more advanced stages in patients
with early-stage MF. However, similar to the large-cohort study conducted by
Talpur et al. [20] we did not find significant association between the
incidence of folliculotropism and the two investigated outcomes. It is important
to note that only a few patients had folliculotropism, making it unlikely to
find a significant association with the studied events.
The finding of enlarged lymphocytes
(representing at least 25% of the lymphoid infiltrate) was associated with
worse prognosis, based on the literature [20-22]. Cytologic criteria of
lymphocytic atypia, such as increased lymphocyte nuclear size, were not
significantly associated with the investigated outcomes.
Important limitations of the present study
are: retrospective nature, small sample, and relatively low incidence of
events. Our findings with statistically significant associations should be
interpreted and acquired effect in the context of the total histological
picture that describes early MF and in parallel to previous reported changes
that were also associated with progression of the disease.
CONCLUSION
Prospective studies conducted with meaningful
samples have shown most patients with early-stage MF evolve slowly and
characteristically have a good prognosis. Yet, a small group of patients follow
a rapidly-progressive course with considerable higher morbidity and mortality.
Thus, it is essential to identify relevant factors to contribute to better
prognostic analysis besides the current staging model.
After focusing on analyzing histopathological
aspects of the first biopsies conducted in a group of early-stage MF patients,
it is possible to suggest that parakeratosis and superficial and deep
perivascular lymphoid dermal infiltrate pattern are additional features that
may play a prognostic role. New studies are needed to get deeper insights on
the subject.
AUTHORS
CONTRIBUTIONS
1.
Gustavo Moreira Amorim:
Project development, data collection, data analysis, writing (ORCID number:
0000-0001-6067-9463).
2.
Danielle Carvalho
Quintella: Histopathological review. Interpretation of the collected data, text
correction (ORCID number: 0000-0001-90139417).
3.
João Paulo Niemeyer
Corbellini: Contribution to the project design, interpretation of the collected
data, text correction (ORCID number: 0000-0001-81043915).
4.
Marcia Ramos-e-Silva:
Contribution to the project design, text correction (ORCID number:
0000-0003-1625-0760).
5.
Tullia Cuzzi: Contribution
to the project design, histopathological review, interpretation of the
collected data, text correction (ORCID number: 0000-0002-3331-5290).
REFERENCES
1.
Wilcox RA
(2017) Cutaneous T-cell lymphoma: 2017 update on diagnosis, risk -
Stratification and management. Am J Hematol 92: 10850-1102.
2.
Amorim
GM, Niemeyer-Corbellini JP, Quintella DC, Cuzzi T, Ramos-e-SilvaM (2018)
Clinical and epidemiological profile of patients with early stage mycosis
fungoides. An Bras Dermatol 93: 546-552.
3.
Olsen E,
Vonderheid E, Pimpinelli N, Willemze R, Kim Y, et al. (2007) Revisions to the
staging and classification of mycosis fungoides and Sezary syndrome: A proposal
of the International Society for Cutanoues Lymphomas (ICSL) and the cutaneous
lymphoma task force of the European Organization of Research and Treatment of
Cancer (EORTC). Blood 110: 1713-1722.
4.
Vonderheid
EC, Pavlov I, Delgado JC, Martins TB, Telang GH, et al. (2014) Prognostic
factors and risk stratification in early mycosis fungoides. Leuk Lymphoma 55:
44-50.
5.
van Doorn
R, Van Haselen CW, van Voorst Vader PC, Geerts ML, Heule F, et al. (2000)
Mycosis fungoides: Disease evolution and prognosis of 309 Dutch patients. Arch
Dermatol 136: 504-510.
6.
Kim YH,
Liu HL, Mraz-Gernhard S, Varghese A, Hoppe RT (2003) Long-term outcome of 525
patients with mycosis fungoides and Sezary syndrome: Clinical prognostic factors
and risk for disease progression. Arch Dermatol 139: 857-866.
7.
Agar NS,
Wedgeworth E, Crichton S, Mitchell TJ, Cox M, et al. (2010) Survival outcomes
and prognostic factors in mycosis fungoides/Sézary syndrome: Validation of the
revised International Society for Cutaneous Lymphomas/European Organization for
Research and Treatment of Cancer staging proposal. J Clin Oncol 28: 4730-4739.
8.
Eklund Y,
Aronsson A, Schmidtchen A, Relander T (2016) Mycosis fungoides: A retrospective
study of 44 Swedish cases. Acta Derm Venereol 96: 669-673.
9.
Desai M,
Liu S, Parker S (2015) Clinical characteristics, prognostic factors, and
survival of 393 patients with mycosis fungoides and Sézary syndrome in the
south-eastern United States: A single-institution cohort. J Am Acad Dermatol
72: 276-285.
10.
Pimpinelli
N, Olsen EA, Santucci M, Vonderheid E, Haeffner AC, et al. (2005) Defining
early mycosis fungoides. J Am Acad Dermatol 53: 1053-1063.
11.
Santucci
M, Biggeri A, Feller AC, Massi D, Burg G (2000) Efficacy of histologic criteria
for diagnosing early mycosis fungoides. An EORTC Cutaneous Lymphoma Study Group
Investigation. Am J Surg Pathol 24: 40-50.
12.
Wernham
AG, Shah F, Amel-Kashipaz R, Cobbold M, Scarisbrick J (2015) Stage I mycosis
fungoides: Frequent association with a favourable prognosis but disease
progression and disease specific mortality may occur. Br J Dermatol 173:
1295-1297.
13.
Nikolaou
V, Papavid E, Patsatsi A, Siakantaris M, Economidi A, et al. (2017) Prognostic
indicators for mycosis fungoides in a Greek population. Br J Dermatol 176:
1321-1330.
14.
Scarisbrick
JJ, Kim YH, Whittaker SJ, Wood GS, Vermeer MH, et al. (2014) Prognostic
factors, prognostic indices and staging in mycosis fungoides and Sézary
syndrome: Where are we now? Br J Dermatol 170: 1226-1236.
15.
Smoller
BR, Detwiler SP, Kohler S, Hoppe RT, Kim YH (1998) Role of histology in
providing prognostic information in mycosis fungoides. J Cutan Pathol 25:
311-315.
16.
Lever WF,
Schaumburg-Lever G (1990) Lymphoma and leukemia. Lever WF, Schaumburg-Lever G, eds.
Histopathology of the skin 7th Edn. Philadelphia, Pa Lippincott, pp:
806-846.
17.
Marti RM,
Estrach T, Reverter JC, Mascaró JM (1991) Prognostic clinicopathologic factors
in cutaneous T-cell lymphoma. Arch Dermatol 127: 1511-1516.
18.
Ahn CS,
ALSayyah A, Sangueza OP (2014) Mycosis fungoides: An update review of
clinicopathologic variants. Am J Dermatopathol 36: 933-948.
19.
Nagaraghi
ZS, Seirafi H, Valikhani M, Farnaghi F, Kavusi S (2003) Assessment of
histologic criteria in the diagnosis of mycosis fungoides. Int J Dermatol 42:
45-52.
20.
Benton
EC, Crichton S, Talpur R, Agar NS, Fields PA, et al. (2013) A cutaneous
lymphoma international prognostic index (CLIPi) for mycosis fungoides and
Sezary syndrome. Eur J Cancer 49: 2859-2868.
21.
Talpur R,
Singh L, Daulat S, Liu P, Seyfer S, et al. (2012) Long-term outcomes of 1.263
patients with mycosis fungoides and Sézary syndrome from 1982 to 2009. Clin
Cancer Res 18: 5051-5060.
22.
Vergier
B, de Muret A, Beylot-Barry M, Vaillant L, Ekouevi D, et al. (2000)
Transformation of mycosis fungoides: Clinicopathological and prognostic
features of 45 cases. French Study Group of Cutaneous Lymphomas. Blood 95:
2212-2218.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Ophthalmology Clinics and Research (ISSN:2638-115X)
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- Stem Cell Research and Therapeutics (ISSN:2474-4646)
- International Journal of Surgery and Invasive Procedures (ISSN:2640-0820)
- Journal of Alcoholism Clinical Research
- International Journal of Clinical Case Studies and Reports (ISSN:2641-5771)
- International Journal of AIDS (ISSN: 2644-3023)


